
Abstract
Introduction
Patients in intensive care units (ICUs) have poor oral health due to several factors, such as mechanical ventilation and reduced consciousness, which can lead to serious complications.
Objective
This study aimed to investigate the impact of a multimedia evidence-based oral care training program on the oral hygiene of ICU patients.
Methods
This randomized controlled trial involved 60 nurses and 56 patients in two general ICUs, allocated into control and intervention groups using cluster randomization. Nurses in the intervention ICU received multimedia educational content based on an evidence-based oral care algorithm, along with face-to-face training for one month. They then provided the intervention to patients. During the next 3 months, the oral hygiene scores of newly admitted patients were evaluated using the Beck Oral Assessment Scale (BOAS) three times: upon admission to the ICU, 24 h, and 48 h after admission. The control group continued with usual oral care as before. Data were analyzed using SPSS-26 software. The Chi-square test, Fisher's Exact test, Independent T-test, Mann-Whitney U test, and repeated measures analysis of variance (ANOVA) were used.
Results
There were no significant differences between the patients’ and nurses’ groups regarding baseline characteristics. Also, BOAS scores of patients upon admission did not significantly differ between groups (P = .863). In the intervention group, patients’ BOAS scores significantly decreased (improved) from 12.11 ± 1.03 to 7.93 ± 1.61 (24 h after admission) and then to 6.11 ± 1.26 (48 h after admission) (P < .001). However, BOAS scores in the control group did not improve significantly within 24 or 48 h after admission.
Conclusion
This study indicates that multimedia training of an evidence-based, comprehensive oral care algorithm improves the oral hygiene of ICU patients, especially those requiring higher levels of care.
Keywords
Introduction
Oral hygiene can have a significant impact on patients’ overall health and clinical outcomes. Maintaining oral health not only provides comfort to patients, but also prevents several complications such as oral mucosal damage, dry mouth, and oropharyngeal or pulmonary infections. Therefore, an important aspect of nursing care is the provision and maintenance of oral hygiene, especially for patients in intensive care units (ICUs) who are highly dependent on caregivers and often unable to perform basic oral hygiene practices (Adib-Hajbaghery et al., 2011; Salarzehi et al., 2020; Sreenivasan et al., 2018).
Although all ICU patients may have poor oral hygiene, this problem is more common in patients on mechanical ventilation (MV), which is a typical therapeutic strategy in ICUs. A major side effect of MV is ventilator-associated pneumonia (VAP), which is one of the most common hospital-acquired infections, accounting for approximately one-third of all nosocomial infections (Darbanian et al., 2024; Gharebaghi, 2020). Reports indicate that 28% of ventilated patients develop VAP within the first 48 h of ICU admission, and 24% to 50% of patients succumb (Kiabi et al., 2023). Meanwhile, poor oral hygiene is a major risk factor for VAP (Sreenivasan et al., 2018). Poor oral hygiene can also lead to nonventilator-associated hospital-acquired pneumonia (NVHAP), which accounts for up to 74% of hospital-acquired pneumonia (HAP) cases (Kozub et al., 2025; Livesey et al., 2024). Recent studies have shown that proper oral care is the most effective way to prevent NVHAP (Munro et al., 2021).
In addition, the natural oral flora contains approximately 350 bacterial species, predominantly gram-positive streptococci, and several types of viruses and fungi that tend to accumulate in different regions of the oral cavity. Within 48 h of admission to the ICU, the natural oral flora shifts in favor of gram-negative organisms (Salarzehi et al., 2020). This change leads to bacterial accumulation, proliferation of opportunistic pathogens, dental caries, and subsequent systemic infections such as bacteremia, respiratory infections, and even cardiac infections (Yaghini et al., 2017). Therefore, increased attention should be paid to oral hygiene in ICU patients, especially in mechanically ventilated patients (Khoshnevisan et al., 2022; Wainer, 2020).
Nevertheless, some studies have shown that nurses, especially in ICUs, usually prioritize the care needs of patients based on the urgency of medical problems and the reasons for admitting patients, so oral care has been given a lower priority. Nurses need more knowledge and training for oral care and making decisions about when, how often, and how to provide it (Adib-Hajbaghery et al., 2011; Sreenivasan et al., 2018).
Review of Literature
It is widely accepted that “good and frequent oral care” is critical for ICU patients and can be provided through various approaches such as mouthwashes, gels, toothbrushes, and suctioning (Wainer, 2020). Rahmani et al. emphasized in their study that interventions such as toothbrushing and mouthwashing are essential to remove plaque and oral microbes (Karimi et al., 2023). In addition, the use of mouthwashes has been shown to improve oral hygiene. Nevertheless, toothbrushing is considered a primary mechanical intervention and an essential method for removing plaque, a potential source of infection in ICU patients (Salarzehi et al., 2020).
Despite numerous studies on oral care, less attention seems to have been paid to creating a comprehensive guideline for patients with different levels of care needs. For example, while many studies have proposed guidelines specifically for oral care in patients on invasive mechanical ventilation (Atashi et al., 2018; Galhardo et al., 2020; Haghighi et al., 2017; Salarzehi et al., 2020; Tsuda et al., 2020; Zhang et al., 2020), there remains an urgent need for an algorithm that also includes patients on noninvasive mechanical ventilation or those who do not require mechanical ventilation at all. This gap was addressed in the present study.
Improving nurses’ knowledge in this area leads to accurate decision making and improves the quality of care provided to hospitalized patients (Alja’afreh et al., 2018). Among various educational methods, several studies suggest that video demonstrations can effectively enhance nurses’ sense of learning. For example, Dehghan-Nayeri et al. conducted a study on the effectiveness of workshop and multimedia-based training methods on nurses’ decision-making skills regarding ventilator weaning and demonstrated a positive effect on their decision-making skills (Dehghan-Nayeri et al., 2020). This finding suggests that multimedia-based learning can serve as an effective approach to improve knowledge, attitudes, and practice (Dehghan-Nayeri et al., 2020; Hsu et al., 2022).
Unlike traditional methods, multimedia training has the potential to boost motivation and cognitive capacity among learners. Furthermore, this approach can engage trainees more effectively, deliver educational content more efficiently than traditional methods, and foster deeper learning. As such, multimedia-based learning can be considered an effective strategy to enhance knowledge, improve attitudes, and modify practices among learners (Chu et al., 2019; Hsu et al., 2022).
Despite the studies conducted on oral healthcare in ICU patients, limited research has focused on multimedia evidence-based training programs designed as algorithms or clinical guidelines for nurses, specifically addressing comprehensive oral care principles for both conscious and unconscious patients. Given the critical importance of oral hygiene in ICU patients, this study aimed to evaluate the impact of implementing a multimedia evidence-based training program on oral hygiene among patients in ICUs.
Methods
Study Design and Setting
This randomized controlled trial with parallel groups was conducted between July and October 2024 at an educational hospital in Tehran, Iran. Two general ICUs were selected for sampling.
Research Questions
The study aimed to address the following question: Does implementing an evidence-based oral care algorithm affect the oral health of ICU patients?
Study Participants and Sampling
Convenience sampling was adopted. Eligible nurses from two general ICUs in an educational hospital were included in the study based on the following criteria: (1) having at least a bachelor's degree in nursing, (2) having a minimum of 6 months’ work experience in intensive care units, and (3) willingness to participate in the study. Exclusion criteria were: (1) being transferred from the ICU to another ward or hospital, (2) incomplete completion of the questionnaires, and (3) withdrawal from the study during it.
In addition, patients admitted to the ICU during the study period who met the inclusion criteria were consecutively enrolled. These patients included a range of newly admitted individuals of both sexes undergoing either invasive or noninvasive mechanical ventilation or requiring oxygen therapy. Patients were excluded if they were undergoing chemotherapy or radiation therapy, if they had immune system defects, fractures, or surgery in the jaw or mouth, or active periodontal disease. Patients were also excluded from the study if they experienced a change in ventilatory status, worsening of their medical condition, or death during the outcome assessment period. Efforts were made to ensure as much homogeneity as possible between the control and intervention groups.
The sample size of patients was calculated using G*Power software and taking into account three measurements for two groups, with α=0.05 and power = 0.80. With an effect size of 0.25, the sample size in each group was calculated to be at least 28, considering the attrition rate of 10%, the final sample size was 31 participants in each group, and a total of 62.
Randomization and Blinding
As it was impossible to randomly assign each individual to the groups due to contamination bias and the possibility of information sharing between nurses, cluster randomization was used in this trial. This involved tossing a coin with heads and tails to assign each marker to an ICU. After tossing, the selected ICU (ICU-A) was randomly assigned to the intervention site. Therefore, the nurses of ICU-A were assigned to the intervention group, and those of ICU-B were assigned to the control group. Each ward was a general ICU, having 20 beds.
Due to the nature of this study, it was impossible to blind the caregivers (nurses). Since the outcome measurements were conducted by an outcome assessor, blinding the patients was unnecessary. Therefore, only the outcome assessor and the statistician were blinded.
Outcome Measures
Data collection was carried out using demographic questionnaires to gather information on the demographic characteristics of nurses and patients, as well as the BOAS for scoring and assessing oral hygiene in patients before and after the intervention.
Baseline Characteristics
Individual information of nurses and patients was collected using a demographic information form. Nurses’ demographic data included age, gender, educational degree, and history of participating in oral care training courses.
Patient demographics included age, sex, education level, level of consciousness (including alert, confused, lethargic, stuporous, or comatose), ventilator status (including invasive mechanical ventilation, noninvasive mechanical ventilation, or requiring oxygen therapy), and underlying medical conditions.
Beck Oral Assessment Scale (BOAS)
The BOAS was used to assess patients’ oral hygiene. This scale provides a practical and clinical assessment of the oral cavity in critically ill patients (Haghighi et al., 2017). Its validity and reliability were confirmed in a study by Salarzehi et al. (2020). The scale consists of five subcategories: (1) lips, (2) gingiva and oral mucosa, (3) tongue, (4) teeth, and (5) saliva. Each category is scored on a four-point scale ranging from 1 to 4. The total score ranges from 5 to 20, with lower scores indicating better oral health and higher scores indicating greater dysfunction. The scores are interpreted as follows: 5 indicates no dysfunction, 6 to10 indicates mild dysfunction, 11 to 15 indicates moderate dysfunction, and 16 to 20 indicates severe dysfunction (Haghighi et al., 2017).
Study Intervention
Pre-Intervention Phase
In this phase, a 10 min evidence-based comprehensive oral care training video was recorded by two researchers. After the final review, the video was sent via virtual messenger to the nurses in the intervention group. This video was recorded based on an oral care algorithm tailored to three patient categories: alert patients, patients on noninvasive mechanical ventilation, and patients on invasive mechanical ventilation.
The video provided instructions on comprehensive oral care practices, including the use of a toothbrush, mouthwash, and artificial saliva to maintain oral hydration, effective suctioning, checking the tracheal tube cuff, moisturizing the lips, and other relevant care procedures (see Figure 1; Aitken et al., 2023; Mohseni et al., 2024; Sedighi et al., 2024). To validate the content of the algorithm and video, feedback was obtained from ten clinical experts in the field of critical care.
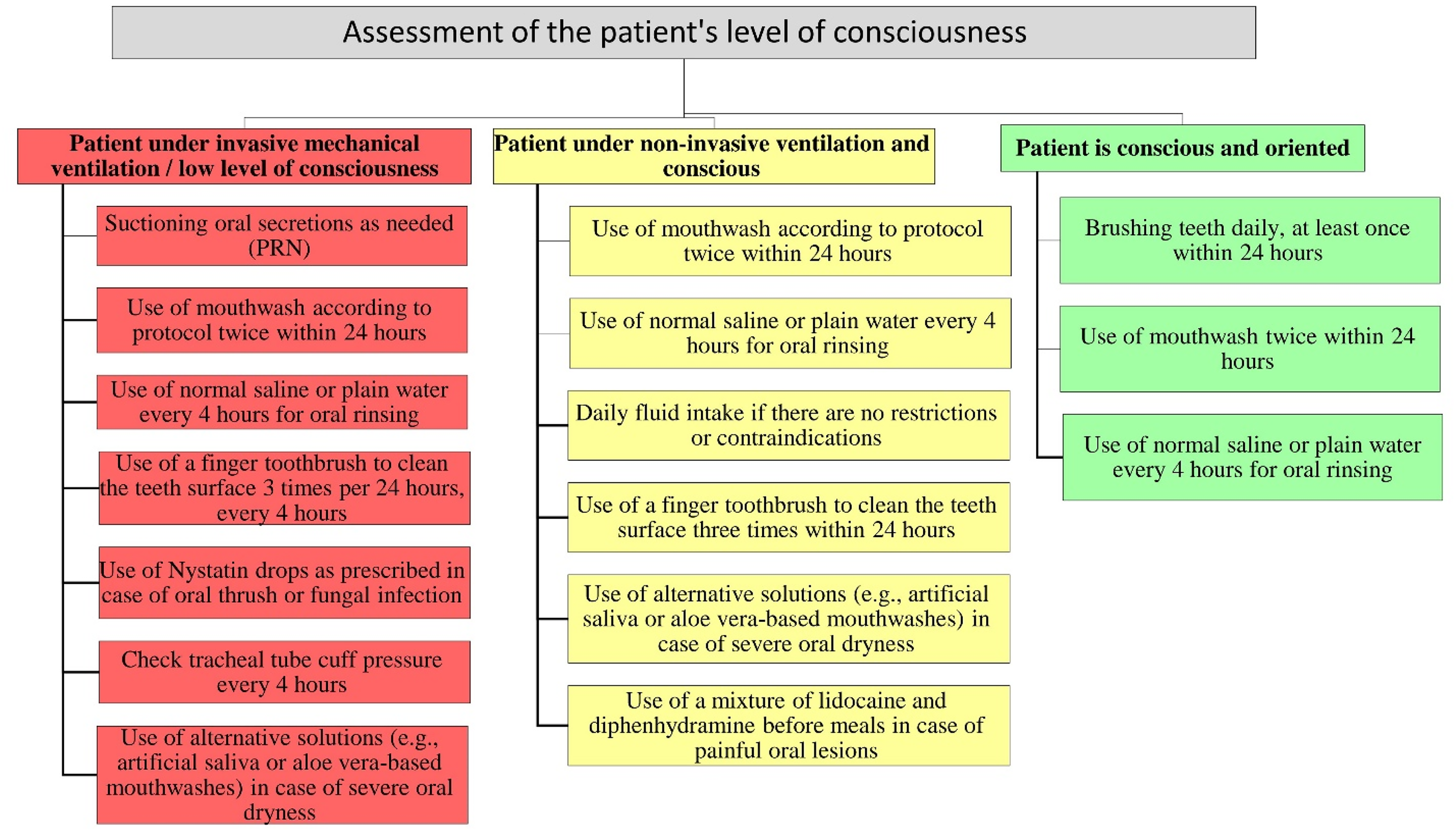
Evidence-based oral care algorithm for patients admitted to intensive care units.
In addition, the evidence-based oral care algorithm was attached to the intervention ICU beds. Then, two researchers provided practical training to nurses in the intervention ICU on different work shifts for 1 month (at least two practical training sessions for each nurse). In addition, the implementation of the evidence-based oral care was monitored by the researchers on different work shifts, and the fidelity of the intervention was measured using a checklist (according to the algorithm and the training video), and possible deficiencies were corrected.
Intervention Phase
After ensuring that the nurses in the intervention group learned the comprehensive oral care algorithm and its continuous implementation, new patients admitted to both ICUs were selected based on the study criteria during 3 months. After obtaining informed consent from the patients or their legal representatives, the oral health status of patients in both groups was assessed using the BOAS three times: upon admission to the ICU, 24 h later, and 48 h after admission. Baseline characteristics of the patients were also obtained.
After patients were admitted to the intervention ICU, nurses provided evidence-based oral care based on the algorithm and educational multimedia content. To ensure adherence to the intervention protocol, the researcher regularly visited the ICU in person, equipped with personal protective equipment, to monitor the oral care provided by the nurses in the intervention group. In the control ICU, usual oral care was provided to patients with similar conditions as before. No other concurrent training or directives were introduced in the control ICU that could have influenced the results.
Statistical Analysis
Data were entered and analyzed using SPSS software (v.26.0) with a significance level set at P < .05. The Shapiro–Wilk test was conducted to assess the normality of the data. Descriptive statistics, including mean, standard deviation, frequency, and percentage, were used to summarize the data. The Chi-square test, Fisher's Exact test, Independent T-test, and Mann–Whitney U test were used for baseline characteristics and pairwise comparisons. To compare the before and after results of the BOAS at 24 and 48 h, a repeated measures analysis of variance (ANOVA) was performed. This analysis assessed significant changes over time across groups and evaluated interactions between them. The analyses were conducted using an intention-to-treat (ITT) approach.
Results
Baseline Characteristics
A total of 56 patients and 60 nurses in two general ICUs participated in the study between July and October 2024. Figure 2 shows the selection process. Of the 76 nurses invited to participate in the study, 65 met the eligibility criteria, with 32 assigned to the control group and 33 to the intervention group. Five nurses withdrew from the study (two from the control group and three from the intervention group) (Figure 2(a)). In addition, 76 newly admitted patients were screened for eligibility during 3 months. Nine of them met the exclusion criteria, and four of them refused to participate in the study. Furthermore, seven of them were excluded during the outcome assessment period (Figure 2(b)).

(a) Nurses recruitment flowchart. (b) Patients recruitment flowchart.
The demographic and clinical characteristics of the nurses and patients are presented in Tables 1 and 2, respectively. The two groups of nurses were not significantly different in terms of age, gender, or level of education. In addition, none of them had attended an oral care training course prior to the current study (Table 1). On the other hand, there were no significant differences between the patient groups in terms of age, sex, educational level, level of consciousness, or underlying diseases (Table 2).
Demographic Characteristics of the Nurses.
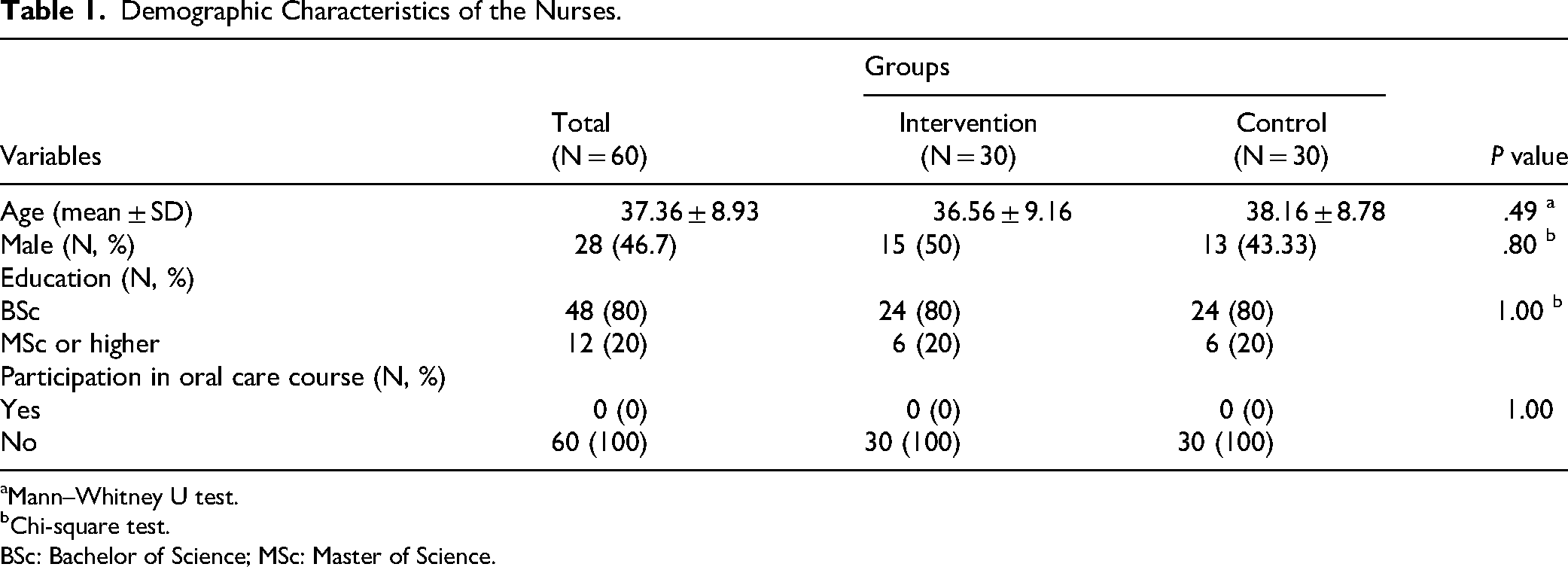
Mann–Whitney U test.
Chi-square test. BSc: Bachelor of Science; MSc: Master of Science.
Demographic and Clinical Characteristics of Patients.

Independent T-test.
Chi-square test.
Fisher's Exact test.
BOAS Scores
The repeated measures ANOVA results revealed a significant effect of time in both control and intervention groups (P < .001), a significant effect of intervention over time (P < .001), and a significant interaction between time and intervention group (P < .001; Table 3).
BOAS Scores Between and Within Effects.
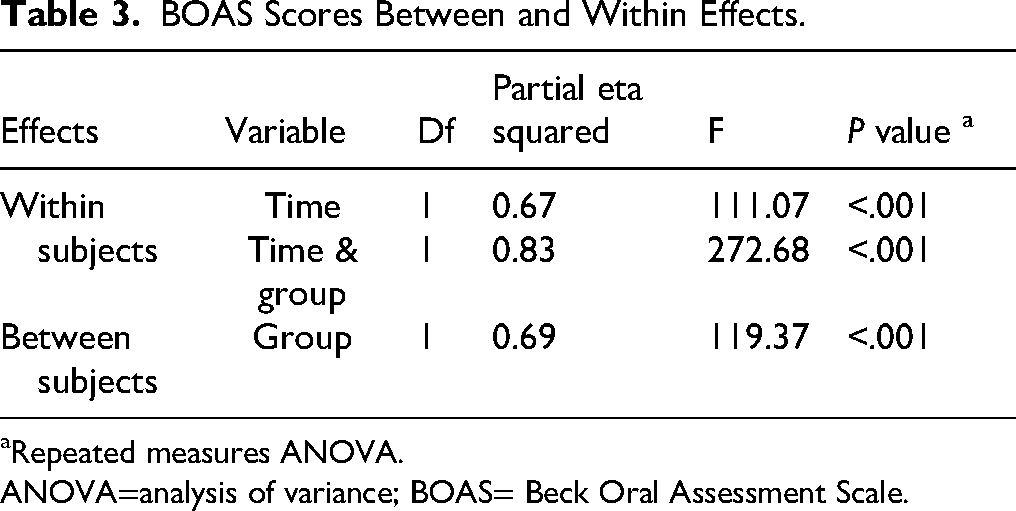
Repeated measures ANOVA.
ANOVA=analysis of variance; BOAS= Beck Oral Assessment Scale.
Figure 3 and Table 4 illustrate the effects of time and intervention on the BOAS scores. In the control group, the BOAS score increased from 12.18 ± 1.92 to 12.79 ± 1.59 (24 h after admission) and then to 13.61 ± 1.87 (48 h after admission). In contrast, patients of the intervention group experienced a decline in the BOAS score, decreasing from 12.11 ± 1.03 to 7.93 ± 1.61 (24 h after admission) and then to 6.11 ± 1.26 (48 h after admission), suggesting that the evidence-based multimedia education program had a positive and impactful effect on oral health outcomes (Figure 3 and Table 4).

Effects of time and intervention on the Beck Oral Assessment Scale (BOAS) scores.
Pairwise Comparisons for BOAS Score.

The preintervention and postintervention (48 h) scores did not have a normal distribution. Both the independent t-test and Mann–Whitney U test were used. Because of the similarity of P value in both tests and the Central Limit Theorem, the results of the Independent T-test were reported.
Postintervention (24 h) scores had a normal distribution, and the Independent t-test was used.
BOAS= Beck Oral Assessment Scale; SD=standard deviation; SE=standard error.
Discussion
The findings of this study indicated that implementing a multimedia training program for comprehensive oral care and its application by ICU nurses significantly improved the oral hygiene of patients on invasive or noninvasive mechanical ventilation, as well as alert patients not requiring mechanical ventilation. To achieve this, an evidence-based oral care program was developed as a comprehensive algorithm.
This algorithm, tailored to each patient's level of consciousness and status of ventilation (requiring invasive or noninvasive mechanical ventilation), was constructed based on multiple references and included interventions such as toothbrushing, mouthwash use, artificial saliva application, oral and tracheal suctioning, tracheal tube cuff pressure assessing, and lip moisturizing (Figure 1). Before the study, oral care was routinely provided to patients once per work shift in both ICUs. After training the nurses of the intervention ICU, they provided standard and appropriate oral care based on the patient's level of consciousness and ventilatory status, according to the algorithm proposed in the study.
To our knowledge, there was no comprehensive guideline for providing oral care to ICU patients. Although some references provided oral care guidelines, they did not offer detailed instructions for different ventilatory and consciousness statuses. The algorithm recommended in the current study addresses these gaps based on updated, evidence-based references.
It appeared that training nurses on this evidence-based oral care algorithm and displaying it prominently for reference during clinical care significantly improved the oral care provided to ICU patients. Using this algorithm, nurses were able to provide comprehensive oral care to patients with varying care needs. As a result, oral hygiene outcomes in the intervention group were significantly better than in the control group, where patients received routine oral care.
The BOAS used in this study for evaluating oral hygiene places significant emphasis on ensuring adequate moisture in the oral mucosal surfaces, tongue, and gingiva, with three of its subscores specifically focused on assessing this aspect. Xerostomia, or dry mouth, can serve as a precursor to the proliferation of harmful microorganisms in the oral cavity, leading to conditions such as oral candidiasis, mouth ulcers and trauma, gingival inflammation, increased dental plaque accumulation, and subsequent dental caries (Ristevska et al., 2015; Salum et al., 2018).
Moreover, underlying conditions such as diabetes, viral infections, oxygen therapy, lack of oral feeding and chewing, physiological stress, and various medications—including antihypertensives, diuretics, and sedatives—can significantly reduce salivary secretion, resulting in severe dry mouth. ICU patients are particularly susceptible to these factors, making the maintenance of adequate oral moisture a critical component of oral care in this population (Adolfsson et al., 2022; Dodds et al., 2023; Sato et al., 2023).
A study by Sedighi et al. (2024) demonstrated that the use of artificial saliva spray for 4 days effectively reduced xerostomia and BOAS scores in COVID-19 patients undergoing noninvasive mechanical ventilation (Sedighi et al., 2024). Similarly, in the current study, the oral care program, which included mouth rinsing every 4 h and the use of artificial saliva in cases of severe dry mouth, resulted in a significant reduction in BOAS scores in mechanically ventilated patients.
Another important aspect of oral care is the reduction of dental and oral plaque, which are optimal sites for the growth of respiratory pathogens, particularly Pseudomonas aeruginosa. This bacterium is the most common and deadly cause of VAP. Therefore, the removal or reduction of dental plaque through brushing and the use of antimicrobial mouthwashes plays a pivotal role in the prevention of VAP (Gershonovitch et al., 2020). In the present study, all patients received 0.12% chlorhexidine mouthwash and a finger toothbrush every 12 h, which effectively reduced their plaque and debris subscores on the BOAS scale. In support of these findings, Haghighi et al. (2017) reported that the use of chlorhexidine mouthwash and toothbrushing significantly reduced the mucosal plaque score (MPS) in intubated patients (Haghighi et al., 2017).
Consistent with the current study, Salarzehi et al. (2020) demonstrated that comprehensive oral care in intubated patients in the ICU led to a significant reduction in BOAS scores and improved oral hygiene in these patients (Salarzehi et al., 2020). Similarly, Atashi et al. (2018) reported similar results when implementing a comprehensive oral care program—including the use of chlorhexidine mouthwash, toothbrushes, oral and pharyngeal suctioning, and moisturizing the oral mucosa and lips with aloe vera gel—in intubated patients (Atashi et al., 2018). These findings are consistent with the results of the current study and highlight the need for comprehensive oral care for intubated patients, especially those with underlying medical conditions.
A notable aspect of the current study that distinguishes it from previous research was the provision of video-based oral care training along with an oral care algorithm tailored to three different categories of ICU patients. In addition, oral care practices were supervised across different work shifts for one month, with nurses receiving guidance as needed to ensure optimal care implementation. This approach not only improved patient oral hygiene but also enhanced the quality and effectiveness of care facilitated by multimedia and face-to-face training.
Effective and continuous training, as well as ensuring proper understanding of the educational content, is essential to sustain a care program. In this study, the primary objective was not only to improve oral hygiene through comprehensive oral care but also to enhance the quality of care and equip ICU nurses with the skills to perform these practices thoroughly and accurately based on the latest scientific evidence. Consequently, a multimedia training approach was adopted.
In the current study, the performance of trained nurses in oral care was found to be superior to that of the control group. Similarly, Liaw et al. (2015) demonstrated that a web-based multimedia training program improved the clinical performance of nurses in acute care units (Liaw et al., 2015). Consistent with this, Chu et al. (2019) found that multimedia training was more effective in improving nurses’ knowledge and skills in pain assessment compared to traditional lecture-based methods (Chu et al., 2019). Furthermore, Jeong (2017) reported that pre-recorded video training significantly improved the clinical skills of nursing students (Jeong, 2017).
Based on the results of the present study and a review of related literature, it can be concluded that teaching oral care to ICU nurses using multimedia methods has a significant positive impact on the oral hygiene of ICU patients. In addition, it promotes better visual learning of proper oral care practices, increases satisfaction, and results in greater utilization of educational content compared to traditional teaching methods.
It is suggested that future studies use the proposed algorithm and similar examples in a wider range of patients. Also, specialized oral care algorithms should be designed for patients with specific conditions, such as oral malignancy, who require a particular oral care program. In addition, it is recommended that the knowledge, attitude, and practice (KAP) of ICU nurses regarding oral care be studied in the future. Several studies indicate that nurses often possess inadequate knowledge and demonstrate poor practice in providing oral care (Asadi & Jahanimoghadam, 2024; Iyer et al., 2023; Jun, 2022). This deficiency appears to stem from multiple, interconnected factors that warrant further investigation (Li et al., 2024). Studies in this regard appear to be limited.
Strengths and Limitations
In this study, a comprehensive evidence-based oral care algorithm was recommended for critical care patients with different levels of consciousness and ventilatory status. Also, a training video was recorded and provided to nurses to improve their clinical skills in this regard. In addition, the outcome assessor and the statistician were blinded to limit possible bias as much as possible.
One of the limitations of this study was that it was conducted in one hospital. Hence, the generalizability of the results may be affected. On the other hand, due to the high turnover and mortality rates of patients in the studied ICUs, the intervention period was shortened to prevent severe sample attrition. Perhaps a longer intervention period could yield more accurate and reliable results and clarify possible shortcomings of the algorithm. These limitations may affect the results of the study. It is suggested that these limitations be addressed in future studies.
Implications for Practice
The proposed oral care algorithm serves as a standardized, evidence-based guideline for ICU patients, provided it aligns with their specific needs. To reinforce adherence, the algorithm could be displayed at ICU bedsides, ensuring nurses have immediate reference during patient care. Additionally, integrating oral care training more prominently into nursing education programs would further promote its consistent and effective implementation.
Conclusion
The multimedia training of the evidence-based, comprehensive oral care algorithm for ICU nurses has led to a significant improvement in the oral hygiene of patients across various levels of care. Therefore, if consistent with the patients’ conditions, it is recommended that the clinical guidelines proposed in this study be utilized alongside nurse training programs to improve the oral hygiene of ICU patients. However, further research may be warranted.
Supplemental Material
sj-docx-1-son-10.1177_23779608251391498 - Supplemental material for The Effect of an Evidence-Based Oral Care Algorithm on Oral Health of Critical Care Patients: A Randomized Controlled Trial
Supplemental material, sj-docx-1-son-10.1177_23779608251391498 for The Effect of an Evidence-Based Oral Care Algorithm on Oral Health of Critical Care Patients: A Randomized Controlled Trial by Amirhossein Nasirmoghadas, Kosar Pourhasan, Yekta Rahimi, Mehrnoosh Azizi Zarazmi, Mohammad Arabdoost and Ladan Sedighi in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to thank the Clinical Research Development Unit (CRDU) of Loghman Hakim Educational Hospital, affiliated with Shahid Beheshti University of Medical Sciences, Tehran, Iran, for their support, cooperation, and assistance throughout the study.
ORCID iDs
Ethical Approval
Ethical permissions for this study were prospectively issued by the Research Ethics Committee of the Faculty of Nursing at Shahid Beheshti University of Medical Sciences in June 2024 (approval ID: IR.SBMU.PHARMACY.REC.1403.064). The investigation conforms to the principles outlined in the “Declaration of Helsinki.” Written informed consent was obtained from participants. They could withdraw from the study at any time without any consequences.
Consent for Publication
No individual data or information is provided, thus negating the need for consent for publication.
Author Contributions
NA, PK, and SL were involved in study conception and design, and drafting of the article; RY in data analysis and interpretation; NA, PK, SL, and RY in critical revision of the article; and PK, AzM, and ArM in data collection.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets and protocol used and analyzed during the current study are available from the corresponding author on reasonable request.
Trial Registration
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.