
Abstract
Background
The October 7th, 2023 war on the Gaza Strip triggered widespread psychological distress across Palestine. Nursing students in the West Bank, already under academic and clinical stressors, are particularly susceptible to post-traumatic stress symptoms (PTSS) and reduced quality of life (QOL).
Objective
To assess the prevalence and severity of PTSS and its association with QOL among West Bank nursing students after the Gaza war.
Methods
A cross-sectional study was conducted with 339 undergraduate nursing students from a West Bank university. Data were collected using the Impact of Event Scale-Revised and WHOQOL-BREF instruments. Analyses included descriptive statistics, t-tests, ANOVA, Pearson correlation, and Eta coefficients using SPSS v20.
Results
Students showed high levels of PTSS: intrusion (M = 1.92, SD = 0.87), avoidance (M = 1.73, SD = 0.89), and hyperarousal (M = 1.75, SD = 0.91), with a total PTSS score of M = 5.41. The overall QOL score was moderate (M = 3.25, SD = 0.57), with the environmental domain scoring lowest (M = 2.93, SD = 0.81). Exposure to checkpoint violence (reported by 49.2%) was associated with higher PTSS (M = 6.09 vs. 4.90; p < .001) and lower QOL (M = 3.13 vs. 3.34; p = .001). The PTSS and QOL were negatively correlated (r = –0.352, p < .001). Eta coefficients indicated small-to-moderate effect sizes for checkpoint exposure: PTSS (η = 0.235), QOL (η = 0.181).
Conclusion
West Bank nursing students experienced significant psychological distress and reduced QOL following the Gaza war, especially those exposed to checkpoint violence. These findings underscore the need for targeted mental health interventions and academic accommodations in conflict-affected educational settings.
Keywords
Introduction
The protracted political conflict in Palestine has fostered a landscape marked by chronic instability, insecurity, and psychosocial strain. The escalation of violence that began on October 7th, 2023, in the Gaza Strip had profound psychological repercussions across all Palestinian territories, including the West Bank. Although geographically removed from the direct conflict zone, West Bank communities experienced its ripple effects through heightened fear, continuous media coverage, academic disruption, and intensified military presence.
University students—especially those in high-stress academic disciplines like nursing—are particularly vulnerable to mental health deterioration due to the compounding effects of academic pressure, clinical demands, and exposure to trauma. Nursing education is inherently demanding, requiring students to manage rigorous theoretical instruction alongside emotionally taxing clinical experiences. In conflict settings, these pressures are exacerbated by political instability, socioeconomic hardship, and restrictions on mobility, increasing the risk for post-traumatic stress symptoms (PTSS) such as intrusive thoughts, hyperarousal, and avoidance behaviors.
Numerous studies have explored the psychological challenges among Palestinian students. For instance, examined the relationship between social anxiety and self-esteem among undergraduate nursing students, while Almhdawi et al. (2022) focused on sources of stress and coping behaviors during first clinical placements. Similarly, Hawash and Dwaikat (2020) assessed stress sources and coping strategies among physical therapy students during clinical practice, and Toqan et al. (2022) investigated the effectiveness of progressive muscle relaxation exercises in reducing anxiety among nursing students during their initial clinical training. These studies reflect a growing body of literature on student mental health in Palestine but often do not address trauma specifically or assess its connection to quality of life (QOL).
Quality of life, as conceptualized by the World Health Organization, encompasses physical, psychological, social, and environmental domains. In Palestine, persistent structural challenges—including limited access to healthcare and public services, restricted movement, and economic instability—can undermine QOL, particularly for students facing continuous stress. Trauma exposure has been shown to erode well-being, disrupt concentration, impair academic performance, and impede long-term professional development.
Checkpoint violence, a well-documented feature of daily life in the West Bank, contributes significantly to psychological distress among students. Regular encounters with Israeli military checkpoints can involve verbal harassment, psychological intimidation, and physical searches. These experiences disrupt academic routines and can lead to chronic stress reactions, particularly for students commuting to clinical training sites.
This study specifically aimed to assess the prevalence and severity of PTSS and their association with QOL among West Bank nursing students following the October 7th, 2023, war on the Gaza Strip. Additionally, it examined the impact of exposure to violence at Israeli checkpoints on these outcomes.
Literature Review
Armed conflict, political instability, and systemic violence have shaped the lived realities of Palestinians for decades, creating a mental health crisis that particularly affects young adults and students. Within academic institutions, nursing students are a particularly vulnerable subgroup due to the dual stressors of clinical training and exposure to war-related trauma. This literature review explores prior research on the impact of war on QOL, the prevalence and manifestations of PTSS, and the specific effects on nursing students in conflict zones, with a focus on the Palestinian context.
Existing research consistently reveals that populations living in conflict areas experience high levels of PTSS and compromised QOL. War trauma has been linked to psychological symptoms such as flashbacks, nightmares, avoidance, and heightened arousal (Thabet & Abu Sultan, 2017). In Palestine, these symptoms are compounded by ongoing threats, such as house demolitions, military incursions, and restricted movement. Giacaman (2020) note that Palestinian youth face daily stressors that contribute to cumulative trauma and deteriorating mental health. The normalization of violence and instability has become an everyday reality that deeply influences personal and social development.
Students in higher education, particularly those enrolled in healthcare fields, experience additional layers of psychological burden. Academic stress, clinical demands, and personal safety concerns intersect in ways that impair both academic performance and psychological well-being (Pereira et al., 2018). Nursing students, in particular, are expected to perform under emotionally intense conditions during clinical rotations, even while managing their own trauma. According to Malarbi et al. (2017), individuals exposed to trauma show impairments in executive functions such as attention and working memory, which are critical for clinical competence. As such, the demands of nursing education may exacerbate trauma-related symptoms among students in war-torn regions.
In Palestine, war-related disruptions in education are well-documented. Palestine, Ministry of Education and Higher Education (2019) reported that frequent school closures, military raids on campuses, and limitations on movement due to checkpoints or curfews have made consistent attendance difficult for university students. These disruptions are not only logistical but psychological, as each missed class or clinical shift increases academic stress and feelings of hopelessness. Juzoor for Health and Social Development (2021) emphasized that mobility restrictions particularly affect students from rural areas, who often commute long distances and must navigate Israeli military checkpoints that are sites of potential violence and humiliation.
Checkpoint violence, a recurring feature in the West Bank, has become a focal point in understanding trauma among students. Bdier et al. (2024) found that frequent exposure to physical and verbal abuse at checkpoints significantly correlates with depressive symptoms and anxiety among young Palestinians. These experiences not only affect psychological health but also disrupt the sense of agency and safety necessary for successful learning. Moreover, students who are repeatedly subjected to such experiences may begin to exhibit avoidance behaviors or develop persistent hypervigilance, both of which are common in PTSD (Hamdan & Hallaq, 2021).
Quality of life in conflict zones is shaped by more than just physical safety. According to the World Health Organization (2020), QOL encompasses environmental, social, psychological, and physical domains. In the Palestinian context, access to healthcare, public services, and even leisure activities is limited by political and economic barriers. Alqaissi et al. (2025) reported that students in areas affected by conflict rated their environmental and psychological well-being the lowest among all QOL domains. Financial strain, lack of access to mental health care, and social isolation further decrease QOL and may contribute to a cycle of psychological decline.
Although research has examined PTSD and QOL in general populations within Palestine, few studies have specifically addressed the experiences of nursing students. This gap is notable given the critical role nurses play in the Palestinian healthcare system, especially during humanitarian crises. Understanding how trauma affects nursing students’ psychological health and QOL is essential for informing interventions that ensure both student success and healthcare system resilience.
Aim of the Study
This study specifically aimed to assess the prevalence and severity of PTSS and their association with QOL among West Bank nursing students following the October 7th, 2023, war on the Gaza Strip. Additionally, the study examined how exposure to violence at Israeli checkpoints influenced these outcomes.
Methods
Study Design
This study employed a quantitative, descriptive cross-sectional design to assess the prevalence and severity of PTSS and their association with QOL among Palestinian nursing students following the October 7th, 2023 war on the Gaza Strip.
Study Population and Sample Size
The target population consisted of approximately 1,650 undergraduate nursing students enrolled at a university in the West Bank. A total of 339 students participated, representing about 20.5% of the population. This sample size was deemed sufficient for descriptive and inferential analysis based on standard sample size estimation for cross-sectional studies with a 95% confidence level and margin of error of 5%.
Sampling Method and Justification
Participants were recruited using convenience sampling, selected based on accessibility and willingness to participate during the data collection period. This method was chosen due to logistical constraints such as restricted mobility, heightened security conditions, and academic disruptions. However, convenience sampling may introduce selection bias and limit the generalizability of findings beyond the sample. These limitations are acknowledged in the interpretation of results.
Data Collection Procedures and Timeframe
Data were collected over a one-month period from December 1 to December 31, 2023, using self-administered questionnaires delivered through two modes:
In-person distribution: Paper questionnaires were handed out during scheduled lectures and clinical training sessions by the research team. Online distribution: A secure survey link was sent via the university's official e-learning platform (e.g., Moodle) and institutional student email system. Access was restricted to currently enrolled students with university credentials, ensuring that only eligible participants completed the online survey.
Eligibility Criteria
Participants were eligible if they were:
Currently enrolled undergraduate nursing students at the university. Aged 18 or older. Willing to provide informed consent.
Contrary to an earlier version of this manuscript, students with known psychiatric disorders were not excluded. This decision was made to preserve the ecological validity of the findings and capture the full range of psychological burden during a national crisis. Excluding such students could underestimate the true prevalence and severity of trauma symptoms.
Instruments
Impact of Event Scale-Revised
This 22-item instrument measures PTSS across three subscales: intrusion, avoidance, and hyperarousal. Items are rated on a 5-point Likert scale from 0 (not at all) to 4 (extremely). Higher scores reflect greater symptom severity. In this study, the Impact of Event Scale-Revised demonstrated excellent internal consistency (Cronbach's alpha = 0.941).
WHOQOL-BREF
The 26-item WHOQOL-BREF assesses QOL across four domains: physical health, psychological well-being, social relationships, and environmental conditions. Items are scored on a 5-point Likert scale. Following WHO guidelines, domain scores were calculated and transformed into a 0–100 scale. While WHO does not recommend a composite total score, for this study, an average across the four domain scores was computed to provide a general indicator of overall well-being.
A 60% threshold (score ≥ 60/100) was used to differentiate between “poor” and “good” QOL, consistent with prior studies in similar conflict-affected settings (e.g., Abuejheisheh et al., 2024; Alshaikh et al., 2023).
Demographic and Exposure Questionnaire
A structured tool was developed to collect demographic data (e.g., age, gender, academic year, marital status, residence) and information related to checkpoint exposure.
Checkpoint violence exposure was measured using a multi-item checklist. Students were asked:
Whether they passed through Israeli checkpoints en route to campus or clinical placements (Yes/No). Whether they had experienced verbal (e.g., insults), psychological (e.g., intimidation, humiliation), or physical violence (e.g., pushing, hitting). Whether they had witnessed violence against others.
Participants could select more than one type of exposure. However, frequency or severity of incidents was not assessed, which is acknowledged as a limitation.
Statistical Analysis
Data were analyzed using SPSS version 20. Descriptive statistics (means, standard deviations, frequencies, percentages) summarized participant characteristics and scale responses.
Normality of distribution for PTSS and QOL scores was assessed using the Kolmogorov–Smirnov test:
PTSS total score: K–S = 0.055, p = .081
QOL total score: K–S = 0.063, p = .074
Since p > .05, both variables were considered normally distributed, supporting the use of parametric tests.
Independent sample t-tests and one-way ANOVA were used to compare PTSS and QOL scores across demographic groups.
Pearson correlation tested the association between PTSS and QOL.
Eta coefficients assessed the strength of association between checkpoint violence exposure and both outcomes.
A p < .05 was considered statistically significant.
Consideration of Confounding Variables
While this study did not exclude participants based on psychiatric history, we acknowledge the potential influence of uncontrolled confounders, including:
Prior trauma not related to recent events. Baseline academic stress or burnout. Socioeconomic status. Preexisting physical or mental health conditions. Although these were not statistically controlled due to the study's cross-sectional nature, demographic, and exposure data were collected to allow for stratified analysis. Future studies should consider regression modeling or longitudinal designs to better isolate causal effects.
Ethical Considerations
Ethical approval was granted by the Institutional Review Board of Palestine Polytechnic University at number (REC, PPU, 121). Participants received a full explanation of the study's purpose, and informed consent was obtained prior to data collection. Confidentiality was ensured, and all data were anonymzed.
Results
Sample’s Characteristics
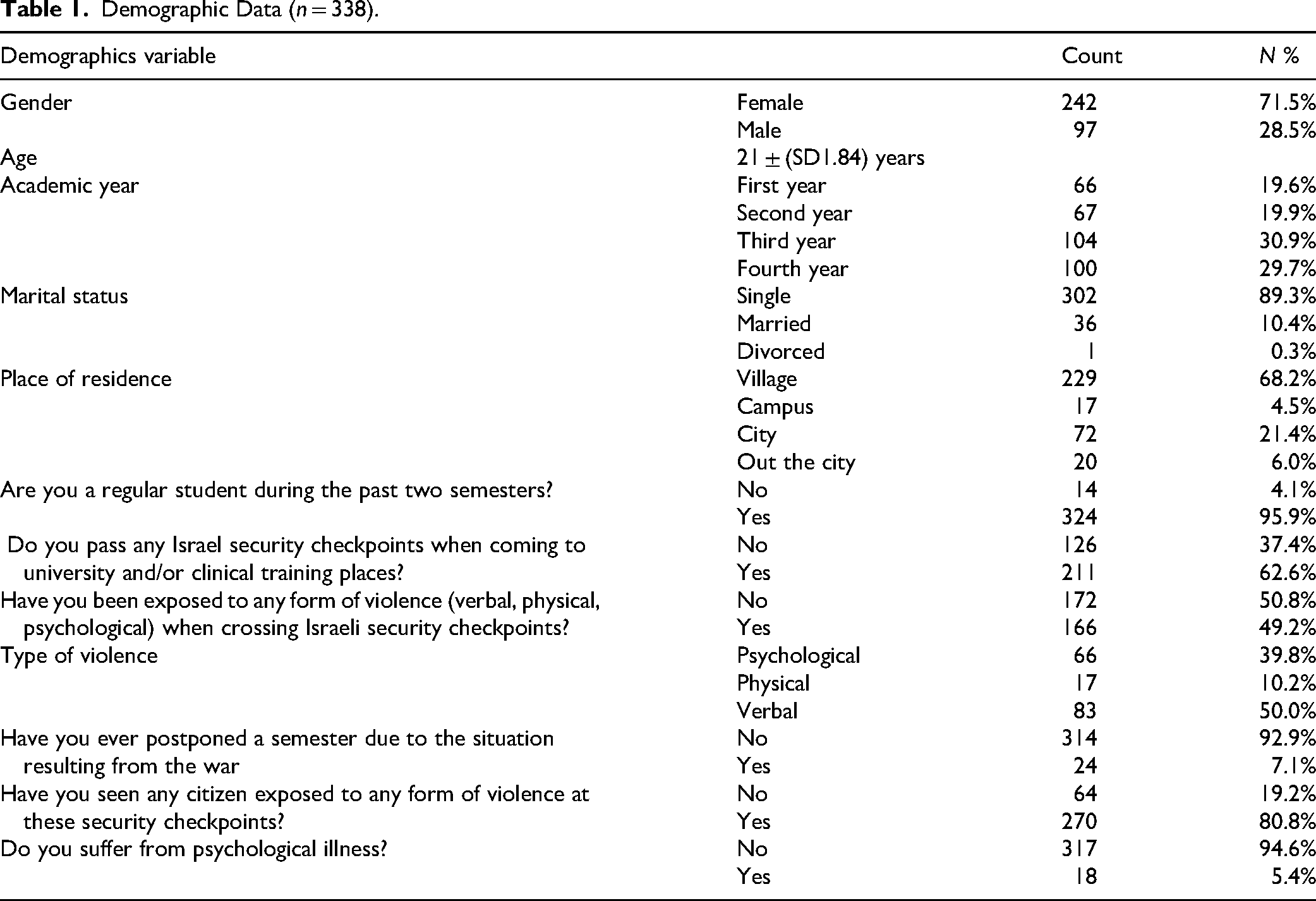
The final sample included 339 students (71.5% female, mean age = 21 ± 1.84 years). The majority (68.2%) resided in villages, and 62.6% regularly passed through Israeli checkpoints. Of those, 49.2% reported exposure to checkpoint violence, including verbal (50%), psychological (39.8%), and physical (10.2%) abuse as in Table 1.
Demographic Data (n = 338).
The analysis in Table 2 The findings revealed high levels of PTSS among participants, with elevated mean scores across all subscales—intrusion (M = 1.92), avoidance (M = 1.73), and hyperarousal (M = 1.75). The total PTSS score (M = 5.41) indicates a significant psychological impact, suggesting widespread trauma-related distress that warrants further attention and intervention strategies.
Means and Standard Deviations of Post-Traumatic Stress Symptoms.

From Table 3, the mean scores for avoidance, intrusion, and hyperarousal subscales were all high, indicating elevated post-traumatic stress levels among students. The total PTSD mean score was 5.41, reflecting significant psychological distress with consistent responses across all subscales.
Means and Standard Deviations of Each Subscale of Post-Traumatic Stress Symptoms.

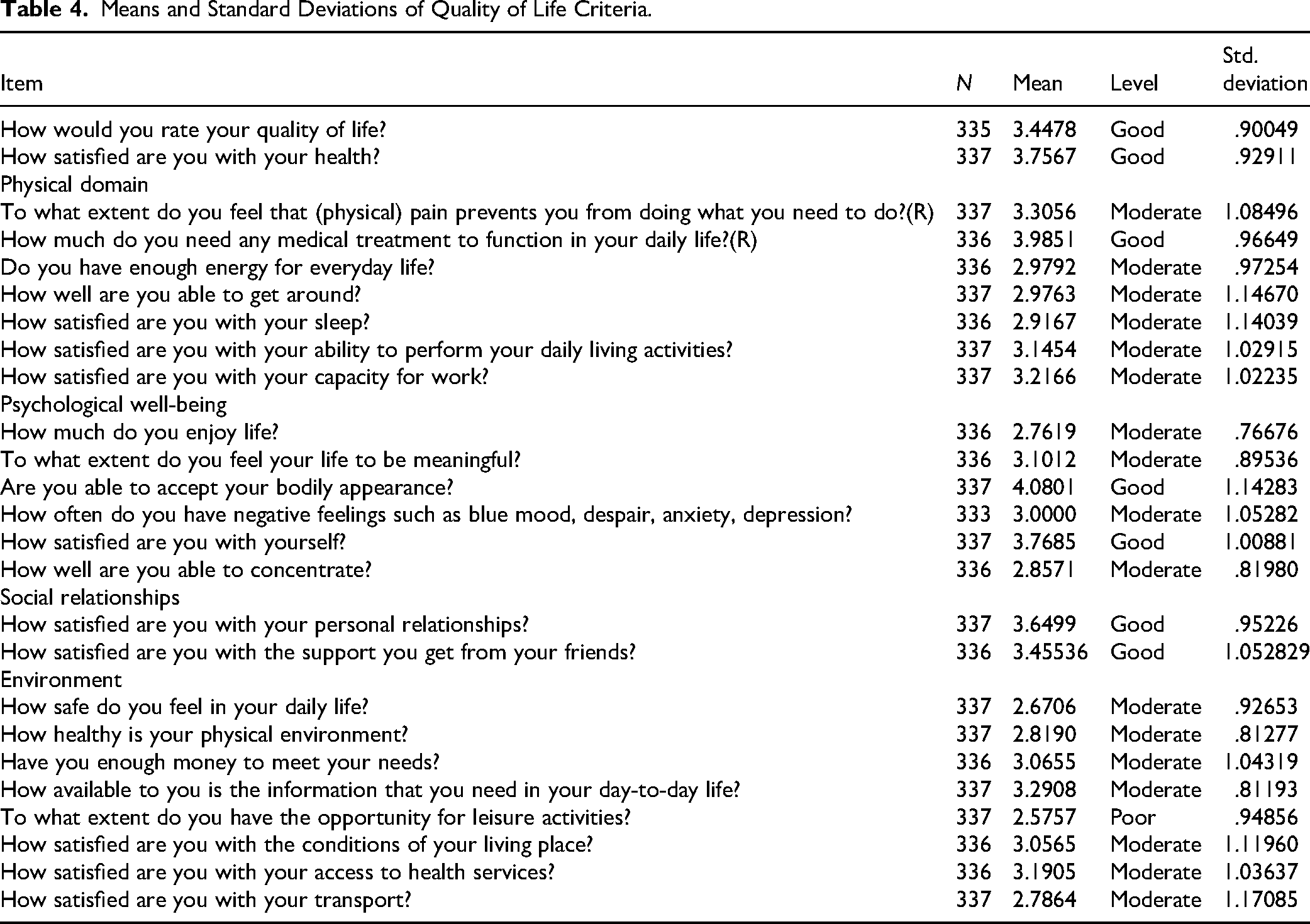
From Table 4, the analysis showed that the level of QOL is Moderate within (M = 3.24, SD = .566). The most of students are able to accept their bodily appearance within (M = 4.08, SD = 1.14), but the level of the ability to perform their daily living activities is moderate within (M = 3.14, SD = 1.02), where the level of having opportunity for leisure activities is poor within (M = 2.5, SD = .566).
Means and Standard Deviations of Quality of Life Criteria.
The findings indicate that Palestinian nursing students report poor overall QOL, particularly in physical, psychological, and environmental domains. While self-satisfaction and social relationships were rated as good, the low scores in essential areas highlight the adverse impact of ongoing conflict and trauma on students’ daily well-being and functioning as in Table 5.
Score (From100) of Each Domain of Quality of Life.

To analyze the relationship between exposure to violence at checkpoints and level of PTSD and QOL for Palestinian nursing students, Eta coefficient has calculated, also independent sample T-test has used to check the differences of the QOL and the level of PTSD according to exposure to violence at checkpoints. This is clear in the below tables.
From Table 6, the results showed that there is a weak relationship between exposure to violence at checkpoints and level of PTSD and QOL for Palestinian nursing students, within Eta coefficient equal: .235 and .181, respectively.
Eta Coefficient Values.

From Table 7, the analysis indicated that there is a significant difference at α = .05, of the QOL and the level of PTSD according to exposure to violence at checkpoints. With p-values: .001 to .000, respectively. It obvious that the level of the QOL is lower for students who exposure to violence, where their level of PTSD Symptoms is higher than the others.
Independent Sample T-Test Results of the Differences of the Quality of Life and the Level of PTSD According to Exposure to Violence at Checkpoints.

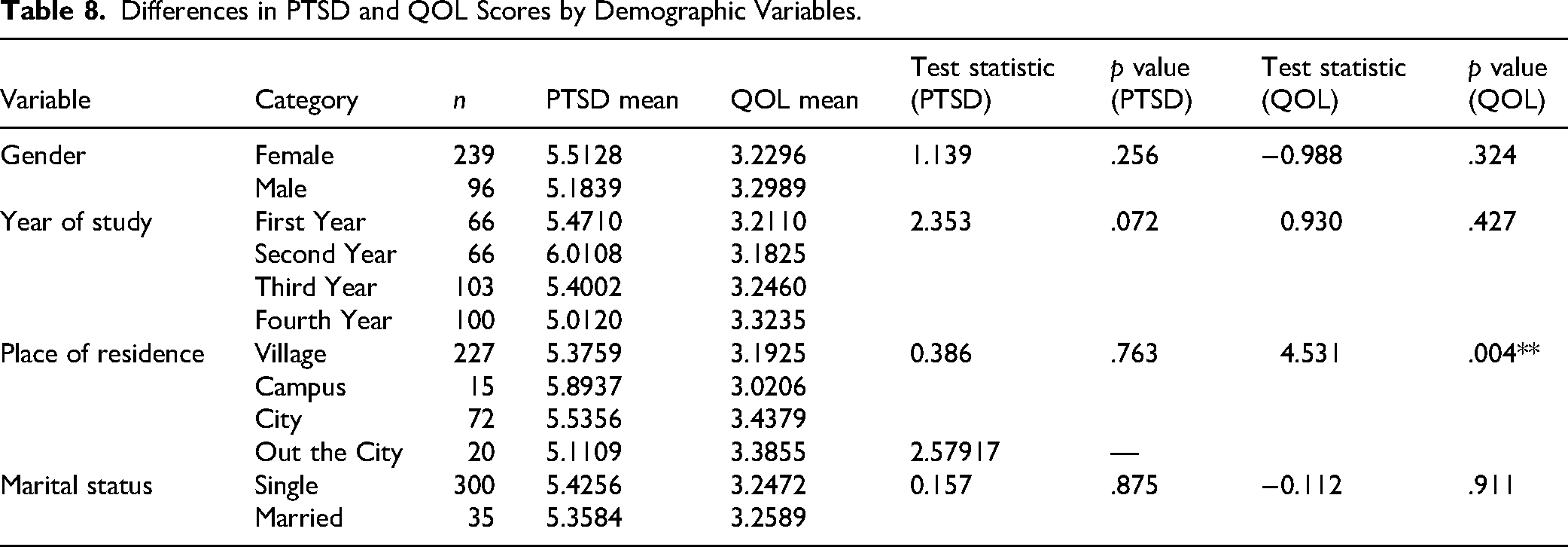
From Table 8, the analysis revealed no significant differences in PTSD or QOL scores based on gender, year of study, or marital status. However, place of residence significantly affected QOL, with students living in cities reporting better outcomes. This suggests geographic factors influence well-being more than demographic characteristics in this conflict-affected population.
Differences in PTSD and QOL Scores by Demographic Variables.
Discussion
This study explored the prevalence and impact of PTSS and QOL among Palestinian nursing students following the October 7th, 2023 Gaza war. The findings confirm a high psychological burden and compromised QOL among participants, with checkpoint violence emerging as a critical stressor. These results are consistent with prior studies from conflict-affected regions, emphasizing that even indirect exposure to war-related violence leads to lasting trauma and functional impairment (Farajalla et al., 2025; Thabet & Abu Sultan, 2017; Veronese et al., 2024).
Notably, nearly half the student's experienced violence at checkpoints, with those exposed demonstrating significantly higher PTSS and lower QOL scores. This aligns with Bdier et al. (2024), who emphasized the psychological effects of chronic exposure to occupational violence, especially in transit zones. Moreover, a significant negative correlation between PTSS and QOL was observed—echoing findings by Giacco et al. (2013)—where trauma directly impairs personal, social, and environmental well-being.
While most QOL domains were rated as moderate to poor, students reported relatively strong social support, suggesting resilience mechanisms through peer and family connections. In line with Giacaman (2020) and Toqan et al. (2023), such social capital can serve as a buffer against chronic stress. However, institutional and structural interventions remain essential to address the root causes of mental distress.
The findings also resonate with regional studies on emergency and nursing personnel. For example, Mohammadi et al. (2021) highlighted the importance of ethical education in strengthening moral resilience among paramedics, which may be beneficial for nursing students facing ethically challenging war-related situations. Likewise, Hadian et al. (2022) identified numerous system-level barriers that hinder prehospital emergency responses in crisis settings—many of which are paralleled in the constraints faced by Palestinian students navigating trauma and limited access to care.
Additionally, Al Khalaileh et al. (2020) pointed out the multiple layers of psychological and logistical challenges faced by nurses during disaster response. Similar stressors were evident in our sample, where students were simultaneously coping with clinical training, academic responsibilities, and traumatic exposure. Supporting nursing students’ mental health is not only a matter of educational success but of future healthcare system readiness during crises.
Time-related stressors also play a key role in shaping nursing students’ psychological outcomes, particularly during times of crisis. According to Qtait and Alarab (2018), nursing students often encounter multiple time management obstacles, including overlapping academic and clinical responsibilities, unclear scheduling, and limited institutional support—all of which intensify under conflict conditions. Furthermore, systemic inefficiencies at the leadership level can compound these stressors. Qtait (2023) emphasized in a systematic review that nurse managers’ time management practices directly influence team functioning, workload distribution, and clinical learning environments. In protracted conflict settings, both individual and organizational time management capacities are critical in mitigating stress, maintaining continuity, and supporting students’ mental well-being.
On a broader scale, disrupted access to healthcare and academic continuity—also observed in medical tourism contexts during conflict (Khan et al., 2023; Irfan et al., 2025)—underscores the compounded vulnerabilities of healthcare trainees in war-torn settings. These students, as future professionals, represent a linchpin in the resilience of national health systems and must be equipped with both psychological and ethical preparedness for crisis response.
Study Limitations
This study has several limitations that should be acknowledged. First, the use of convenience sampling limits the generalizability of findings, as participants may not represent all nursing students across the West Bank or Palestine. Second, the cross-sectional design precludes causal inference and only captures psychological states at a single time point. Third, exposure to checkpoint violence was assessed via self-report and did not include frequency or severity, which may limit precision in interpreting trauma intensity. Finally, although several demographic and violence exposure variables were analyzed, the study did not control for other potential confounders such as socioeconomic status, academic performance, or past psychiatric history.
Conclusion and Recommendations for Future Research
Palestinian nursing students demonstrated high levels of trauma-related stress and compromised QOL in the aftermath of the Gaza war. These findings highlight the urgent need for trauma-informed mental health services, academic accommodations, and protective policies in higher education institutions in conflict zones.
Future research should adopt longitudinal or mixed-methods designs to capture the evolving nature of trauma and coping over time. Comparative studies between different healthcare disciplines could uncover occupation-specific stressors. Interventional studies evaluating the effectiveness of resilience-building, bioethics training, or trauma-reduction programs (e.g., psychological first aid, peer support models) are also needed. Lastly, future studies should explore the role of community-based and digital mental health solutions in mitigating psychological burden among students with limited access to in-person care.
Implications for Practice
This study highlights the critical need for trauma-informed support for nursing students in conflict zones. High levels of PTSS and poor QOL, especially among those exposed to checkpoint violence, indicate a significant psychological burden. Practical implications include integrating mental health services, academic accommodations, and resilience-building programs into nursing education. Faculty should be trained to recognize trauma, and institutions must advocate for safer student mobility. These interventions are essential to support students’ well-being, ensure academic success, and strengthen the future healthcare workforce in politically unstable settings like the West Bank.
Footnotes
Acknowledgments
The authors would like to thank who participated in this study for their time and valuable insights.
Ethical Considerations
Ethical approval was granted by the Institutional Review Board of Palestine Polytechnic University at number (REC, PPU, 121). Participants received a full explanation of the study's purpose, and informed consent was obtained prior to data collection. Confidentiality was ensured, and all data were anonymzed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this study available on paper.