
Abstract
Introduction
Evaluating the utilization of protocols used in managing asthma emergencies in the pediatric setting should be effective in preventing errors during emergency procedures. To ensure that pediatric asthma emergencies are managed properly, there is a need for healthcare personnel to adhere to guidelines for the management of pediatric asthma emergencies.
Aim
To evaluate the utilization of management protocol for pediatric asthma emergencies.
Methodology
Cross-sectional survey, using a semi-structured questionnaire to gather data from medical personnel to determine the effective use of asthma guidelines in the emergency management of pediatrics. Data were analyzed using SPSS version 27.0. Pearson's Chi-square test of association was used to determine the association between the dependent and independent variables, with a p-value < 0.05 regarded as statistically significant in association.
Findings
Adherence (mean score = 3.49, SD = 1.342) for nurses and a (mean score = 4.25, SD = 0.463) adherence for physicians to the protocol for the management of pediatric asthma emergencies at the health facility. There was a significant statistical association between adherence to the pediatric asthma emergency protocol and the management outcome of pediatric asthma emergency protocol (p-value 0.001).
Inadequate resources, such as resuscitation equipment (66.7%) and nebulizers (55.9%), were the barriers hindering the adherence and utilization of the management protocol for pediatric asthma.
Conclusion
Although there is high utilization and adherence to the management protocol for pediatric asthma emergencies, availability of essential equipment, training nurses and physicians to sustain the utilization and the positive outcome of the protocol guidelines are needed.
Introduction
Asthma is a chronic airway inflammatory disorder that involves several cells and cellular elements in association with hyper-responsiveness of the airway (Craig et al., 2023). Globally, Asthma is one of the dominant non-communicable respiratory conditions among children (Balaji et al., 2020). According to the World Health Organization(WHO), about 300 million people live with asthma globally, and this may increase to 400 million by the end of 2025 (World Health Organization, 2022).
The disease process of pediatric asthma involves a complex interaction of chemistry, physics, immunology, and pharmacology where mucus secretion, bronchial spasm, edema, and scar remodeling occur (Mangova et al., 2020). It is also estimated that pediatric asthma accounts for 10%–15% of the global disease burden among children (Asher et al., 2021). The prevalence of pediatric asthma increases by 1% every decade in Europe and 2% in Africa and the Middle East, while that of Asia is reduced by 1% every decade (Asher et al., 2021).
Childhood asthma is becoming more common in Africa (Mosler et al., 2020a). In Central Africa, 10% to 20% of children between the ages of 12 and 14 are thought to have asthma symptoms, and slightly over 20% in South Africa (Mosler et al., 2020b). In Ghana, there is a decreasing trend of asthma cases, but among the pediatric age group, the cases are on the ascendancy (Ghana Health Service DHIM2, 2024). In 2021, a total of 84,700 asthma cases were recorded, and this decreased to 80,841 cases in 2022 (Ghana Health Service DHIM 2, 2024). Among children between the ages of 5–19 years, 23,926 asthma cases were recorded in 2021, representing 28.2% of all asthma cases recorded in 2021. In 2022, a total of 25,413 asthma cases were recorded among children aged 5–19 years, and this represented 31.4% of all asthma cases in 2022 (Ghana Health Service DHIMS 2, 2024). This indicates that there is an increasing trend of asthma among children in Ghana. In the Upper East region of Ghana, 30.3% of all asthma cases recorded in 2021 were among children, and this increased to 33.4% in 2022 (Ghana Health Service DHIMS 2, 2024).
To ensure that pediatric asthma emergencies are managed properly, there is a need for medical personnel to adhere to guidelines and protocols for the management of pediatric asthma emergencies. There exist several protocols and guidelines on the management of asthma for both children and adults. The British Thoracic Society (BTS) in 1990 made a guideline for the management of asthma (Jafarnejad & Khoshnezhad Ebrahimi, 2020).
The management protocol and guidelines for pediatric asthma emergencies may vary from country to country. However, the utilization of these guidelines and protocols by healthcare workers determines the quality of care given in these emergencies (Mosler et al., 2020a). In Ghana, management of emergencies, including pediatric asthma, is based on standard protocols and guidelines (The standard treatment guidelines). The use and adherence to these protocols and guidelines are essential to the survival of children with asthma.
Despite the availability of evidence-based protocols for managing pediatric asthma emergencies, there exists a notable gap in the consistent and effective utilization of these protocols in clinical settings (Castagnoli et al., 2023; Jafarnejad & Khoshnezhad Ebrahimi, 2020). This deficiency in adherence to established guidelines poses a considerable risk to the well-being of pediatric patients experiencing acute asthma exacerbations.
There is a paucity of research assessing the practical efficacy of established management protocols for pediatric asthma emergencies, despite their existence. By evaluating the results of the present protocols used at the Regional Hospital in the Upper East in addressing pediatric asthma emergencies, this study seeks to close, this gap.
Conceptual Framework
Donabedian's conceptual framework was adopted for this study. This involves evaluating the structure, process, and outcomes of care (Donabedian, 1988).
Structure: This is the first component of the Donabedian Model of Quality of Care. It entails assessing the regional hospital's resources and organizational aspects influencing pediatric asthma care, including examining the medical personnel, availability of equipment, adherence to protocols/guidelines, and the existence of the regional hospital's established protocols (Papadopoulos et al., 2023).
Process: This is the second component under the Donabedian Model. The stage involves a detailed assessment of the actual process during the delivery of care in pediatric asthma emergencies. The various activities the nurses and doctors put in place to provide care for the asthma patients are based on the guidelines.
Outcome: The quality of healthcare is evaluated by the outcome and indicates whether, during the process, care goals were achieved. In this study, the result is when the child regains their normal breathing pattern (Wuaku et al., 2022). Find the details in Figure 1.
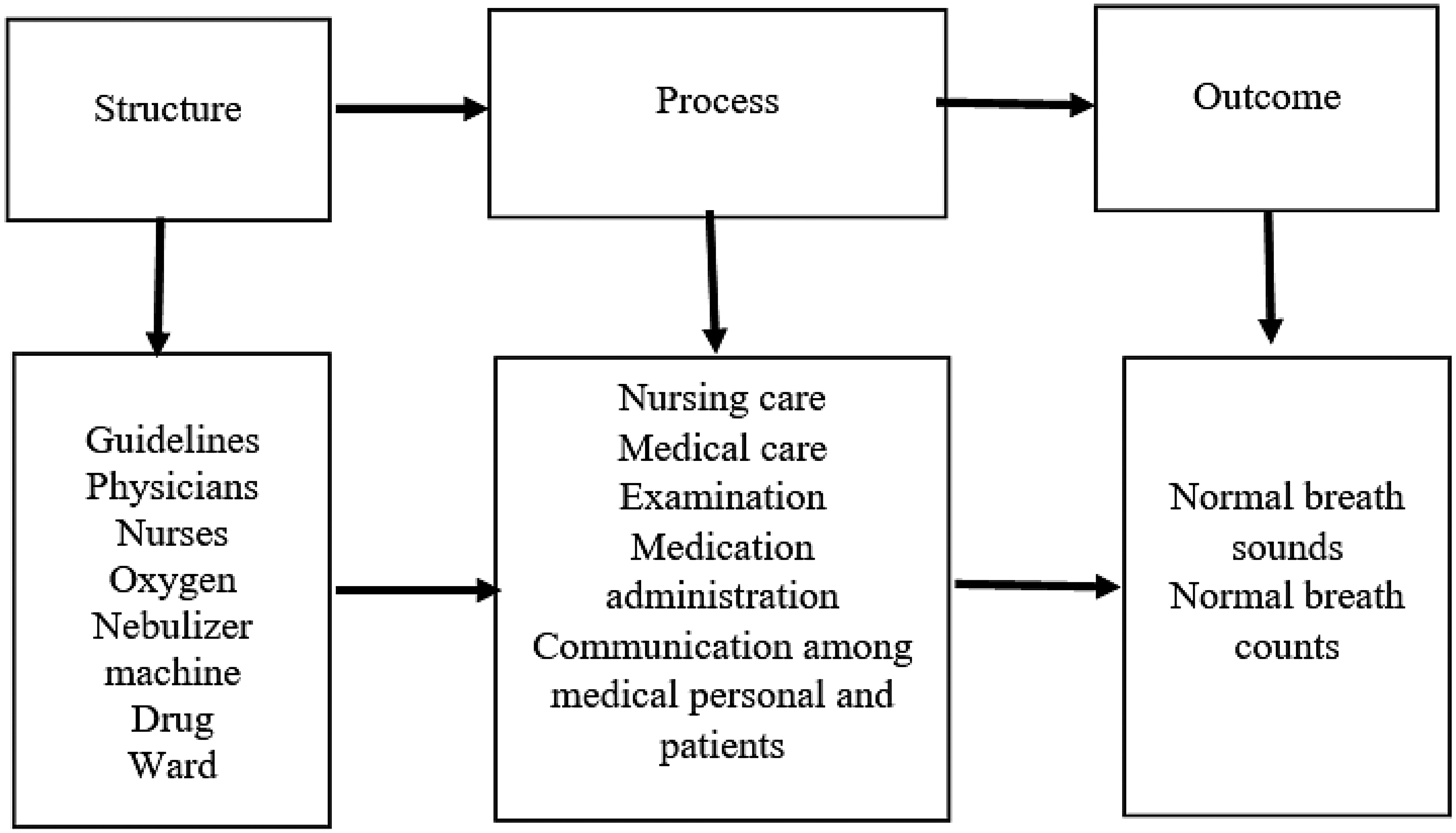
Evaluation of the Quality Use of the Asthma Protocol (Wuaku et al. 2022).
Review of Literature
Asthma is one of the most frequent respiratory emergencies faced by the pediatric world and a potential life-threatening episode (Craig et al., 2023). Clinical guidelines for childhood asthma management frequently rely on data extracted from adult studies, although adult and pediatric asthma mechanisms and treatment responses differ significantly (Mathioudakis et al., 2021)—the poor adherence to the usage of guidelines in managing asthma emergencies in children worldwide. The effects result in the inappropriate use of antibiotics (Hoosen et al., 2020). The overall adherence to the pediatric asthma protocol was 58.1% in Durban, South Africa. There was a higher adherence among pediatricians (77.0%) than general practitioners (58.1%) (Homaira et al., 2020). In the implementation of asthma guidelines in South Korea, it was observed that 89.3% of physicians are aware of the guidelines, but only 11% of them complied with them (Jo et al., 2020).
While existing literature has investigated the adherence to protocols in pediatric asthmatic emergencies, there is a prominent gap in the adherence to management protocol in pediatric asthmatic emergencies in urban areas in low-income countries. Our study addresses this gap by conducting a descriptive study using SPSS version 27.0 to analyze the data, which revealed that medical personnel adhered to protocol management in pediatric asthmatic emergencies, but there was a need for sustainability through the provision of equipment and ongoing training of personnel.
Operational Definition of Terms
Asthma: When a child finds it difficult to breathe his/her normal breathe.
Utilization: The approach healthcare providers use the guidelines for managing pediatric asthma emergencies.
Pediatric: A child within the ages of one month to 12 years.
Medical Personnel
Management Protocol: The standardized recognized procedures to care for asthma emergencies in children.
Research Question
What is the level of adherence to the protocol management of pediatric asthmatic emergencies among nurses and doctors at the regional hospital?
Methods
Study Design and Study Setting
An analytical cross-sectional quantitative approach was employed as a research design. The data collection method was a census sampling using a self-administered Semi-Structured Questionnaire. The study was conducted at the health facility in the Upper East of the country.
The health facility is located within the Bolgatanga Municipal in the Upper East region. The health facility serves as a referral center for the 15 administrative districts and 101 sub-district health facilities, including the neighboring health facilities from north northeast region and the countries surrounding it. The hospital has 38 medical officers, six specialists (one pediatrician), 451 nurses, with 11 being clinical nurse specialists which four are pediatric specialists.
The pediatric unit and the emergency units of the hospital have five oxygen cylinders each, one oxygen concentrator each, one nebulizer each, four pediatric-size respiratory masks each, a box of pediatric emergency drugs each, and a printed copy of the standard treatment guidelines (7th edition, 2017) each. The hospital also has a wireless internet system. The pediatric unit and the emergency unit have two mobile tablets each and four desktop computers.
Study Population and Sampling
The study involved medical personnel directly involved in the management of pediatric asthma emergencies in the health facility at the various departments: the pediatric unit and the accident and emergency unit.
The total population of medical personnel in the various units is 84, eight physicians and 76 nurses. The census technique was used since all the participants were used. A self-administered, semi-structured questionnaire was used to collect the relevant data from participants. The participants were engaged in this study after they had consented to participate in the study. The questionnaires were self-administered to nurses and physicians using Google Forms. The pediatric unit and the emergency units of the health facility have WhatsApp groups; hence, the link to the questionnaire was shared on the WhatsApp platform of the units involved. This made it easy to reach all the nurses and physicians in those units.
Inclusion and Exclusion Criteria
The inclusion criterion included registered nurses working at the pediatric unit and the emergency unit. And also physicians working at the pediatric unit and the emergency unit. Nurses and physicians who were on leave or refused to participate in the study were excluded from the study.
Ethical Issues
The research adhered to ethical guidelines by obtaining ethical clearance from the Institutional Review Board of Health Research Centre in the Region (NHRCIRB623) and the Research Development Unit at Regional Hospital. An introductory letter from college of the principal investigator was submitted to the above institutions listed. Participant information pamphlets were given to all participants to read and decide if they would like to participate in the study before the commencement of data collection. Ensuring that informed consent from all participants was sought before. Confidentiality and anonymity of participant information were maintained during data collection, analysis, and reporting. Institutional Review Board approval was obtained before the commencement of the study.
We ensured that participation in the study was voluntary and no intimidation was applied. The participants were informed they could withdraw from the study without persuasion. Participants were all assured of confidentiality and anonymity that the data collected would be kept private. Access to the data is restricted to the research team alone.
Data Collection Instruments and Tools
The questionnaires were self-administered to the nurses and physicians using Google Forms. A structured questionnaire was used to collect the relevant data from participants. The questionnaire addressed the demographic information of the participants, medical personnel's adherence to management protocol for pediatric asthma emergencies, management protocol outcomes for pediatric asthma emergencies, and the barriers to the usage of a management protocol for pediatric asthma emergencies. Questions in the data collection tool were adapted from pediatric authors like Garagorri-Gutierrez and Leiros-Rodriguez (2022) and Pudasainee-Kapri (2021).
The questionnaires for the study were reviewed by research supervisors and other expert researchers. Based on the feedback from the supervisors (PhD holders) and other expert researchers (pediatric nurse specialists), modifications were made to improve the structure and wording of the questionnaire.
For reliability, Cronbach's alpha was used to assess internal consistency, yielding a score of 0.846. Also, the questionnaire was administered via Google Forms, and this ensured standardized data collection, which minimized interviewer bias. Even though test–retest reliability was not evaluated, the researcher's adherence to the predefined inclusion and exclusion criteria, as well as the homogeneity of the sample, enhanced measurement stability. In addition, the statistical tool for data analysis was SPSS version 27.0 software, which is also a recommended scientific package for analyzing data in health research.
This ensured the validity of the study. The data collection Google Form-based questionnaires were piloted in one of the district health facilities in the region to identify gaps, standardize, and ensure quality assurance in the data. Also, for clarification of the tool for freedom from any bias. Vague questions identified were corrected for participants in this study to have a clearer understanding of the tool.
Letters were sent to the Director of the health facility as well as the departmental heads. The letters provided detailed information about the study, which was then communicated to the medical personnel. Permission was given to the team to conduct the study. Data collection was done by the first author, a registered student nurse at the time this project was conducted. The two other authors are PhD holders in nursing education, and the third author is an esteemed statistician. All of them guided the data process as well as supervised the study.
Data Collection Technique and Procedure
Introductory letters were sent to the Director of the health facility and the departmental heads to pave the way for data collection. The nurses and physicians were informed about the nature, objective, and procedure of the study. The data were collected using an online structured questionnaire designed through Google Forms. The questionnaire link was shared electronically with the selected nurses and physicians at the health facility. An introductory text was attached to the Google Forms, which provided the nurses and physicians with the details. The objective of the study, voluntary participation, and confidentiality of responses were all assured.
Participants who gave informed consent were able to proceed with the completion of the form. Participants were given 14 days to complete and submit the questionnaire; reminders were sent four times to encourage them to complete the questionnaire. Participants used an average of 30 to 45 min to complete the questionnaire. The completed responses were stored in the Google Form platform, which reduced manual entry errors and maintained the integrity of the responses. The responses were copied into an Excel sheet for onward analysis.
Data Analysis
The information gathered was imputed and analyzed using the Statistical Package for Social Sciences (SPSS) version 27.0 software. Before entry into the software, the questionnaires underwent a thorough cross-check to ensure completeness. Data cleaning procedures were implemented to address any missing values. The analysis of the data was conducted using both inferential and descriptive statistical methods, aligning with the study's objective. A Pearson chi-square test of association was conducted between the dependent and independent variables, and a p-value <0.05 was considered a statistically significant association.
Data Quality Management
These data were collected, entered into Excel spreadsheets, and stored on a password-protected computer, and a backup copy was kept securely on a separate and password-protected hard drive. These data were only accessible to the first author and the other authors who are supervisors. These data were treated as strictly confidential. All who chose to be included in the study completed informed consent. Participants were assigned unique alphanumeric identifiers to ensure strict confidentiality.
Results
Sociodemographic Characteristics (Nurses)
Table 1 shows the sociodemographic characteristics of respondents (nurses). Among the nurses, 26 (34.2%) were aged 30–34 years and one (1.3%) of the respondents was 40 years and above. With regards to the cadre of the respondents, most of the respondents, 46 (60.5%), were Registered General Nurses, and only two (2.6%) were Pediatric Nurse Specialists. Most of the respondents, 49 (64.5%), have 1–5 years’ experience of work, and one (1.3%) has 16–20 years’ experience of work. Details are shown in Table 1.
Sociodemographic Characteristics (Nurses), N = 76.

Adherence to Pediatric Asthma Emergency Protocol (Nurses)
Table 2 illustrates a five-point Likert scale, which is also an interval scale with a significant mean. From 1 to 1.80 denotes strongly disagree (SD), from 1.81 to 2.6 means disagree (D), and from 2.61 to 3.40 means neutral (N). From 3.41 to 4.20 means agree (A) and from 4.21 to 5.0 means strongly agree (SA). The statement “I am familiar with the protocol relevant to my role in pediatric asthma emergency management,” the mean is 3.43. This means that most of the respondents are familiar with the pediatric asthma emergency protocol. The statement “I consistently follow the established pediatric asthma emergency management protocol during pediatric asthma emergencies” has a mean of 3.49, and this indicates that there is high adherence to using the established pediatric asthma emergency management protocol during pediatric asthma emergencies.
Adherence to Pediatric Asthma Emergency Protocol (Nurses).

Association Between Sociodemographic Factors and Adherence to the Approved Clinical Protocol for Pediatric Asthma Emergency
Table 3 indicates that having sufficient training in management of pediatric asthma emergencies was statistically significant (p-value 0.002) with adherence to the approved clinical protocol for managing pediatric asthma emergencies. The other factors were not statistically significant. Find the details in Table 3.
Association Between Sociodemographic Factors and Adherence to the Approved Clinical Protocol for Pediatric Asthma Emergency.

Test of Association Between Adherence to Pediatric Asthma Emergency Protocol and Management Outcome of Pediatric Asthma Emergency Protocol (Nurses)
Table 4 shows the Pearson chi-square test of statistical association between adherence to the pediatric asthma emergency protocol and the management outcome of pediatric asthma emergency protocol. There is a significant statistical association between adherence to the pediatric asthma emergency protocol and the management outcome of pediatric asthma emergency protocol (p-value 0.001).
Test of Association Between Adherence to the Pediatric Asthma Emergency Protocol and Management Outcome of Pediatric Asthma Emergency Protocol (Nurses).

Sociodemographic Characteristics of Respondents (Physicians)
The sociodemographic characteristics of respondents (physicians) are shown in Table 5. Over one-third of the respondents, three (37.5%) and three (37.5%) are aged 30–34 years and 35–39 years, respectively. Only one (12.5%) is a pediatric specialist. Over three-quarters of the respondents, six (75.0%) have 1–5 years of work experience. Details of the rest of the sociodemographic characteristics are
Sociodemographic Characteristics (Physicians), N = 8.

Adherence to the management protocol for pediatric asthma emergencies (physicians)
Adherence to the Approved Clinical Protocol for Pediatric Asthma Emergencies (Physicians)
The adherence to pediatric asthma emergency protocol among physicians is shown in Table 6. Illustrates a five-point Likert scale, which is also an interval scale with a significant mean. From 1 to 1.80 denotes strongly disagree (SD), from 1.81 to 2.6 means disagree (D), from 2.61 to 3.40 means neutral (N), from 3.41 to 4.20 means agree (A), and from 4.21 to 5.0 means strongly agree (SA). The statement “I consistently follow the established pediatric asthma emergency management protocol during pediatric asthma emergencies” has a mean score of 4.25, which indicates that most of the respondents consistently follow the pediatric asthma emergency protocol during pediatric asthma emergencies. This means that there is very high adherence to the protocol for managing pediatric asthma emergencies.
Adherence to the Management Protocol for Pediatric Asthma Emergencies (Physician), N = 8.

Management protocol outcomes for pediatric asthma emergencies (physicians).
Table 7 shows the management protocol outcomes for pediatric asthma emergencies among physicians. The table illustrates a five-point Likert scale, which is also an interval scale with a significant mean. From 1 to 1.80 denotes very dissatisfied (VD), from 1.81 to 2.6 means dissatisfied (D), and from 2.61 to 3.40 means neutral (N). From 3.41 to 4.20 means satisfied (S) and 4.21 to 5.0 means very satisfied (VS). The statement “In your experience, what is the general outcome of pediatric asthma emergencies managed at the regional hospital?” has a mean score of 4.63 and which means the respondents are very satisfied with the general outcome of pediatric asthma emergencies managed at the regional hospital. This indicates a very good outcome with the use of the pediatric asthma emergency protocol at the regional hospital.
Management Outcomes for the Protocol for Pediatric Asthma Emergencies (Physicians).

Discussion
Adherence to the Management Protocol for Managing Pediatric Asthma Emergencies
The study found that the Standard Treatment Guideline (39.5%) among nurses and 62.5% among physicians is the most used protocol for the management of pediatric asthma emergencies at the regional hospital. In Ghana, the Standard Treatment Guideline is a major document produced by the Ministry of Health for the management of most diseases in Ghana, including asthma. However, the Global Initiative for Asthma (GINA) guidelines are the most used protocol for the management of asthma, including pediatric asthma emergencies worldwide (Chikaodinaka Ayuk et al., 2017). In the current study, the physician used the Standard Treatment Guidelines more than the nurses in the management of pediatric asthma emergencies. This may be because in Ghana, most of the health personnel, especially the physicians in this current study, use Standard Treatment Guidelines to manage asthmatic emergency cases in children, because that is the only option available for them. The Standard Treatment Guidelines are primarily prescription based, so they are more likely to be utilized by physicians rather than nurses, as the study findings suggest. Additionally, there is no specific nursing management protocol for handling pediatric asthma emergencies, meaning that nurses may rely on general asthma management practices. According to the conceptual framework adapted from Wuaku et al. (2022), these guidelines are part of the structure that influences the process, which in this context refers to the use of the protocol. When the protocol does not adequately address nursing interventions and management, as found in this study, its utilization may be compromised. However, this study was unable to determine whether the protocol used by the nurses met their specific nursing management needs. In-service training for the medical personnel, in this study, revealed that only 53.9% of nurses and 100% of physicians have received sufficient training on the management of pediatric asthma emergencies.
In-service training sessions in some countries are typically organized by health professional labor unions, such as the Registered Nurses and Midwives Association and the Medical Association, as well as by health regulatory bodies like the Nurses and Midwives Council and the Ministry of Health and its agencies. Non-Governmental Organizations also play a role in facilitating these trainings. These sessions are essential for earning Continuing Professional Development (CPD) points, which are necessary for renewing professional licenses. However, most of these trainings are held in the southern part of the country and often come at a cost. In the setting where the study was conducted, in-service training is usually sponsored by employers or NGOs, but there are often quotas that limit the number of participants from each health facility. As a result, only a limited number of medical personnel can attend these sessions. In this study, it is evident that, because the number of nurses exceeds the number of physicians, a smaller proportion of nurses had the opportunity to benefit from in-service training compared to physicians.
The study found a high adherence (mean score = 3.49, SD = 1.342) to the protocol for the management of pediatric asthma emergencies among nurses at the regional hospital. The study also found a very high adherence (mean score = 4.25, SD = 0.463) to the protocol for the management of pediatric asthma emergencies among physicians at the regional hospital. These findings with the findings of Homaira et al. (2020), where it was reported that overall adherence to the pediatric asthma protocol was 58.1%, with higher adherence among pediatricians (77.0%) than general practitioners (58.1%). However, the findings of this current study contradict the findings of a study conducted at King Edward VIII Hospital in Durban, South Africa, by Hoosen et al. (2020), where very low adherence to the GINA protocol was reported. Similarly, the adherence level of this study was higher than that of Jo et al. (2020) in a study in South Korea, where 11% of adherence to the national asthma guideline was recorded among physicians. The level of adherence found in the current study was also higher than the findings of Oshikoya et al. (2020), with adherence of 29.4% in all of Nigeria.
The contradiction between the findings of the current study and those of Hoosen et al. (2020), Jo et al. (2020), and Oshikoya et al. (2020) may be due to the difference in pediatric asthma policy frameworks in the countries where the studies were conducted. A study conducted in Nigeria attributed the poor adherence of physicians to the protocol for the management of asthma in children to poor knowledge on pediatric asthma management, as inadequate training of health professionals on the use of pediatric asthma emergency protocols (Oshikoya et al., 2020). However, the findings of the current study indicated that more than half of the nurses and all the physicians had sufficient in-service training on the management protocol for pediatric asthma emergencies. This may have accounted for the high adherence found in the current study.
In the current study, all the physicians had sufficient training in managing pediatric asthma emergencies, while only slightly more than half of the nurses received similar training. This discrepancy likely contributes to the higher adherence to the protocol among physicians compared to nurses. It also raises questions about the suitability of the protocol (Standard Treatment Guidelines) for nursing management of pediatric asthma at the regional hospital. While the study did not specifically evaluate the protocol's suitability for nurses, the lower adherence among nurses might be due to the protocol being less applicable to their role, combined with insufficient in-service training for nurses at the health facility.
Evaluation of Management Outcomes of the Management Protocol for Pediatric Asthma Emergencies
The study found that there is a satisfactory management protocol outcome for pediatric asthma emergencies (mean score = 3.72, SD = 1.091) among nurses and a very satisfactory management protocol outcome for pediatric asthma emergencies (mean score = 4.63, SD = 0.518) among physicians. This indicates that, overall, there is a positive management protocol outcome for pediatric asthma emergencies at the regional hospital. The study also found a significant statistical association between adherence to the pediatric asthma emergency protocol and the management outcome of pediatric asthma emergency protocol (p-value 0.001).
The findings aligned with the findings of Baldacci et al. (2019), where it was reported that children with asthma exacerbations who were managed with the guidelines had better outcomes than the control group. Also, Baldacci et al. (2019) further reported that adherence to the asthma protocol had a significant association with the positive outcome of pediatric asthma emergencies. This also agreed with the findings of the current study.
Similarly, the findings of the current study aligned with the findings of a study conducted on “Pathways to Improve Pediatric Asthma Care,” where Kaiser et al. (2020) reported that, implementation of guidelines for managing asthma in children was associated with the quality of care and positive outcome for children admitted with asthma. Also, the current study reported a higher positive management protocol outcome among physicians than among nurses. This was confirmed by the higher level of adherence reported among physicians than among nurses.
Protocols and guidelines for the management of cases such as pediatric asthma emergencies are standardized tools that have expert inputs and have gone through testing to prove their effectiveness. It is therefore not surprising that the use of the management protocol for pediatric asthma emergencies yields positive outcomes, as confirmed by the current study and that of Baldacci et al. (2019) and Kaiser et al. (2020).
The findings of this study align with the conceptual framework adapted from Wuaku et al. (2022), which connects the processes of nursing care, medical care, examination, and medication administration to outcomes like normal breath sounds and normal respiratory rates. This suggests that higher adherence to the protocol leads to more positive outcomes. In the current study, physicians demonstrated greater adherence to the protocol than nurses, which correlated with more satisfactory outcomes among physicians. However, the study assessed the outcomes based on the perspectives of the physicians and nurses, which may have introduced bias due to the self-appraisal nature of the questionnaire. Including the perspectives of the parents of the children who received care according to the protocol could have provided a more objective evaluation of the outcomes for both nurses and physicians.
Strengths and Limitations
A census sampling method was used for this study, which allowed data to be collected from the nurses and physicians involved in the management of pediatric emergencies at the regional hospital, ensuring the true reflection of adherence to the pediatric asthma emergencies at the regional hospital, leading to a high accuracy of results. Also, the data collection tool was well developed and pre-tested to gain clarity for the study. Additionally, inferential statistics ensured the rigor of the results.
This study was done in the northern part of the country, where there are inadequate human resources and other needed resources to manage emergency pediatric asthmatic patients. This may not provide a good basis for generalization.
Implications for Practice:
Despite the high level of adherence to pediatric asthma emergency management protocols in the regional hospital setting, sustaining these positive outcomes necessitates a multidimensional approach that addresses structural, educational, and organizational factors. A key priority is the systematic evaluation of equipment gaps and their influence on the real-time application of standardized protocols. Essential equipment—including nebulizers, oxygen delivery systems, spacers, and pulse oximeters—must be readily available and functional to ensure consistency and timeliness of care delivery during acute asthma episodes.
Periodic, structured training programs for physicians and nurses are equally critical in reinforcing protocol familiarity, clinical competence, and confidence in high-stakes scenarios. Regular assessments of these interventions can inform refinement of training content and methodology, contributing to protocol sustainability and improved clinical outcomes over time. Hospitals must therefore institutionalize continuing professional development, embedding it within broader quality improvement frameworks.
This practice-oriented insight also highlights the importance of conducting multi-site comparative studies to identify variations in resource availability, protocol fidelity, and resulting patient outcomes across regional hospitals. Such investigations offer opportunities to uncover best practices, model effective systems, and tailor interventions to meet the specific contextual needs of diverse healthcare environments. Additionally, an assessment of the cost-effectiveness of interventions—such as maintaining critical supplies and delivering routine staff training—can support evidence-informed budgeting decisions that prioritize sustainable improvements in pediatric emergency care.
From a health systems perspective, hospital leadership plays a pivotal role in ensuring that essential resources are consistently procured, maintained, and equitably distributed. Budgetary planning must align with clinical demands, accounting for the ongoing availability of medications, oxygen, and diagnostic tools. Moreover, fostering a culture of interdisciplinary collaboration will enhance team-based care, leveraging the strengths of physicians, nurses, and allied professionals to deliver optimal outcomes for children with acute asthma exacerbations.
Finally, while clinicians must remain vigilant in adhering to established protocols, they should also serve as advocates for the tools and support systems required to deliver high-quality emergency care. The intersection of resource adequacy, continuous education, and collaborative practice forms the bedrock for resilient and responsive pediatric asthma management, positioning health institutions to achieve sustainable, system-wide improvements in patient care.
Areas of Training
Training initiatives should begin with comprehensive familiarization sessions that reinforce the pediatric asthma emergency management protocol. These sessions must be updated regularly to reflect any changes in best practices or clinical guidelines. In parallel, clinical staff should participate in hands-on training aimed at sharpening emergency response skills—particularly in rapid assessment, triage, and the implementation of immediate interventions during acute asthma exacerbations.
Practical instruction in equipment use and maintenance is essential to ensure proficiency in operating, troubleshooting, and maintaining vital medical devices. This not only promotes safety but also mitigates delays in emergency situations. Equally important is the cultivation of clinical decision-making abilities through case-based learning, which empowers providers to initiate and escalate care in alignment with protocol expectations. Finally, training must underscore the importance of accurate documentation, diligent patient monitoring, and timely escalation of care to ensure comprehensive management and accountability.
Areas of Modification
To optimize asthma emergency management in resource-constrained environments, targeted protocol adaptations are necessary. Elements of the existing protocol should be tailored to reflect local resource availability, while preserving the integrity of standard care practices. In settings with limited physician presence, training and credentialing experienced nurses to initiate select components of asthma care can significantly improve response times and outcomes.
Furthermore, adopting simplified asthma severity assessment tools can streamline decision-making processes and reduce delays in treatment initiation. Routine audits of protocol adherence and clinical outcomes, combined with constructive feedback mechanisms, can foster a culture of continuous improvement. Embedding training modules into daily workflows ensures that learning remains active and accessible, reinforcing institutional memory and practice consistency across healthcare teams
Conclusion
Even though there is high utilization and adherence to the management protocol for pediatric asthma emergencies in the regional hospital, efforts should be made to ensure the availability of essential equipment as well as regular training for nurses and physicians to sustain the high level of utilization and positive outcomes of the protocol guidelines.
Footnotes
Acknowledgments
The authors wish to acknowledge the nurses and doctors who voluntarily participated in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors certify that they have no competing financial interests or personal relationships that could be perceived as influencing the work reported in this study.