
Abstract
Introduction
Central line-associated bloodstream infections (CLABSI) are a significant source of hospital-acquired infections, particularly in intensive care units where central venous catheters are frequently used. These infections can lead to increased morbidity, mortality, and healthcare costs. While various clinical guidelines exist for prevention, the actual knowledge and adherence of nurses to these guidelines vary widely, with limited synthesis available at the systematic review level.
Aim
This study aimed to synthesize current evidence on the knowledge, behaviors, and adherence of intensive care unit nurses regarding CLABSI prevention practices.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Peer-reviewed empirical studies published between 2018 and 2024 were searched in PubMed, Scopus, and Google Scholar. Studies were included if they assessed ICU nurses’ knowledge and practices related to CLABSI prevention. After screening 3,585 articles, nine studies met the inclusion criteria and were appraised using the Risk of Bias in Systematic Reviews (ROBIS) tool.
Results
Nine full-text studies published between 2018 and 2024 were analyzed. The studies used cross-sectional surveys, cohort designs, and questionnaire validation methods. Most nurses demonstrated moderate knowledge levels, but adherence to prevention guidelines was low, with full compliance reported by only 5% of participants. Key themes included training gaps, institutional variability, and increased infection risk from improper catheter use. Several studies suggested that targeted education and the use of diagnostic tools such as procalcitonin may support improved outcomes.
Conclusion
This review highlights a persistent gap between knowledge and adherence to CLABSI prevention practices among ICU nurses. Strengthening education, institutional support, and diagnostic strategies is essential to reduce infection rates and improve patient safety.
Introduction
Central venous catheters (CVCs) are medical devices similar to intravenous lines but longer, inserted into veins near or inside the heart—most commonly the internal jugular, subclavian, or femoral veins. These catheters facilitate the administration of intravenous fluids, blood products, medications, hemodialysis, and hemodynamic monitoring. Despite their essential role in patient care, CVCs pose significant risks, including hospital-acquired infections (HAIs), particularly central line-associated bloodstream infections (CLABSIs), which are among the most severe nosocomial infections (Maqbool et al., 2023).
Research highlights the serious consequences of CLABSIs, including increased mortality rates, prolonged hospital stays, and high treatment costs (Badparva et al., 2023; Ziegler et al., 2015). One study estimated that CLABSIs contribute to over 4,000 deaths annually in the United States, with each infection extending hospital stays by approximately 21 days and incurring additional costs exceeding USD 30,000 per episode (Jun et al., 2016).
Nosocomial infections, also known as HAIs, occur when patients develop illnesses during extended hospital stays, typically within 48 h of admission or up to three days post-discharge. These infections pose serious health risks, potentially leading to severe complications or death. A nosocomial infection is classified based on the presence of pathogens in body fluids such as blood or cerebrospinal fluid, even if symptoms are not immediately apparent. Furthermore, hospital staff and visitors are also at risk of acquiring these infections.
Among the most common HAIs are ventilator-associated pneumonia (VAP), urinary catheter-related infections, surgical site infections, and CLABSIs (Edwardson & Cairns, 2019). Studies indicate that insufficient knowledge and poor adherence to best practices among nursing personnel caring for patients with CVCs contribute significantly to the incidence of CLABSIs (Alkubati et al., 2015; Chen et al., 2015; Labeau et al., 2009). Additionally, factors such as work overload and staff shortages have been associated with inadequate compliance with CLABSI prevention protocols (Alkubati et al., 2015; Chen et al., 2015).
Given these concerns, this study aims to assess the knowledge and practices of nurses in preventing CLABSIs. By identifying gaps and areas for improvement, the findings may contribute to enhancing patient safety and reducing the prevalence of CLABSIs in healthcare settings.
Review of Literature
CLABSIs remain a major concern in healthcare settings, particularly in intensive care units (ICUs), where prevalence is higher due to the frequent use of CVCs. Nurses, as frontline healthcare providers, play a vital role in preventing CLABSIs through adequate knowledge, positive attitudes, and adherence to infection prevention guidelines. This literature review explores the current status of ICU nurses’ knowledge and behaviors regarding CLABSI prevention, with a focus on the importance of education, training, and compliance with best practices.
Studies consistently show that ICU nurses possess varying levels of knowledge about CLABSI prevention guidelines. For example, Almalki et al. (2023) reported that ICU nurses in Jeddah, Saudi Arabia, demonstrated moderate knowledge (71% correct responses), but significant gaps persisted, particularly concerning catheter care and infection prevention protocols. Similarly, Xiumen Chi (2020) found that despite the existence of national guidelines in China, ICU nurses lacked comprehensive knowledge about CLABSI prevention, highlighting the need for targeted educational interventions.
The importance of continuing education for healthcare workers is emphasized by Dube et al. (2020), who investigated the increased risk of CLABSI associated with concurrent CVC use. The study found that the risk nearly doubled when multiple central lines were used simultaneously, underscoring the need for better training in central venous access management. Chi et al. (2020) also noted that nurses’ knowledge deficits significantly contributed to infection rates, reinforcing the value of evidence-based training to standardize practice across institutions.
Compliance with CLABSI prevention guidelines is another critical factor influencing infection outcomes. Aloush and Alsaraireh (2018) found that although ICU nurses in Jordan showed some adherence to CLABSI prevention protocols, significant variability existed across hospitals and regions. This inconsistency suggests that adherence is influenced by institutional practices, resource availability, and ongoing training efforts. Additionally, Dang (2023) developed the CLABSI-KAP-Q questionnaire to assess nurses’ knowledge, attitudes, and practices. The study identified key areas for improvement and emphasized the importance of continuous education and routine audits to promote compliance with infection control best practices.
Beyond knowledge and compliance, nurses’ attitudes toward CLABSI prevention also play a critical role. Positive attitudes are generally associated with better adherence to guidelines. Almalki et al. (2023) observed that ICU nurses in Saudi Arabia demonstrated favorable attitudes toward CLABSI prevention, which correlated with higher knowledge levels. However, adherence to protocols remained suboptimal, suggesting that positive attitudes must be accompanied by proper implementation of evidence-based practices.
Some studies have also examined the role of diagnostic tools and biomarkers in CLABSI prevention. Madhura et al. (2021) investigated the utility of procalcitonin (PCT) as a biomarker for diagnosing CLABSIs in patients with chronic kidney disease (CKD) undergoing hemodialysis. PCT levels were significantly elevated in patients with CLABSIs, indicating its potential value in early detection. However, the study stressed that biomarker effectiveness must be supported by nursing knowledge and clinical judgment to optimize outcomes.
In conclusion, the literature suggests that while ICU nurses often possess a basic understanding of CLABSI prevention, considerable knowledge gaps and inconsistencies in practice remain. Strengthening education, standardizing guidelines, and enhancing institutional support are essential to improve compliance and reduce infection rates. Future research should prioritize developing effective training programs, refining assessment tools for knowledge and adherence, and addressing systemic barriers to protocol implementation. Bridging these gaps can significantly lower CLABSI incidence and improve patient outcomes in critical care settings.
Methodology
Research Question
The research question guiding this study is: What is the current level of knowledge and adherence among ICU nurses regarding evidence-based guidelines for preventing central line-associated bloodstream infections (CLABSIs)?
Research Design
This study employs a systematic review methodology to evaluate existing research on ICU nurses’ knowledge and adherence to CLABSI prevention guidelines. A systematic review is selected for its structured and comprehensive approach to synthesizing data from multiple studies, promoting rigor, transparency, and replicability.
Search Process
A literature search was conducted using three major electronic databases: PubMed, Scopus, and Google Scholar. The focus was on peer-reviewed studies published between 2017 and 2024 that examined ICU nurses’ knowledge, attitudes, or behaviors related to CLABSI prevention.
Search Strategy
The search strategy used a combination of keywords and Boolean operators to optimize study retrieval. The following terms were used:
“Central Line-Associated Bloodstream Infection” OR “CLABSI” “Nurses’ Knowledge” OR “Nurses’ Compliance” OR “Nurses’ Adherence” “ICU Nurses” OR “Critical Care Nurses” “Prevention Strategies” OR “Infection Control Guidelines”
Boolean operators such as AND and OR were applied to refine search results. Filters were also used to include only peer-reviewed articles involving human subjects. In Table 1, the inclusion and exclusion criteria are provided.
Inclusion and Exclusion Criteria.

Study Selection
The search initially retrieved 3,585 studies from three databases: Google Scholar (2,846), Scopus (121), and PubMed (618). After removing duplicates, 2,895 unique articles remained for further screening. These studies were then assessed based on predefined inclusion and exclusion criteria, resulting in 1,519 articles selected for full-text review. Following a detailed evaluation of relevance and methodological quality, nine studies met the eligibility criteria and were included in the final systematic review, as illustrated in Figure 1.

PRISMA Flowchart.
Screening Process
The screening process adhered to the Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines to ensure that only high-quality studies were included.
Identification Title and Abstract Screening: The titles and abstracts were examined for relevance to the research question. Studies that did not focus on ICU nurses’ knowledge, attitudes, or adherence to CLABSI prevention were excluded. Full-Text Screening: Full-text articles were reviewed to assess their relevance, ensuring they provided specific data on nurses’ knowledge and behavior. Articles that did not meet this criterion were excluded.
Data Analysis
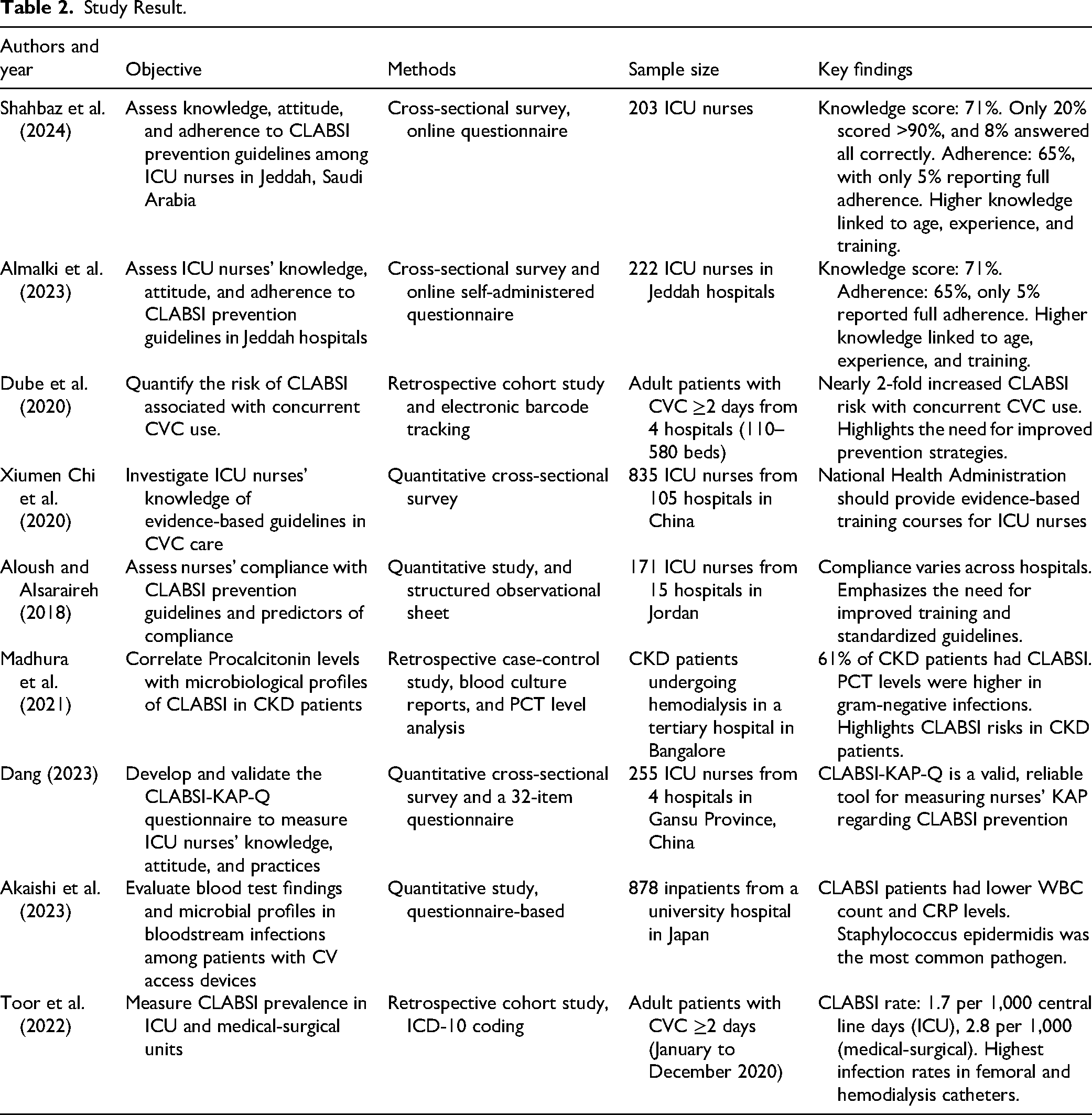
Key variables assessed included nurses’ knowledge, adherence to CLABSI prevention protocols, and factors influencing compliance. Details of the nine included studies are provided in Table 2.
Study Result.
Data Extraction
The data extraction involved documenting the following information from each included study:
Study characteristics (authors, year of publication, and research design). Sample size and participant details (ICU nurses). Methodology employed (e.g., cross-sectional survey and retrospective cohort). Key findings related to nurses’ knowledge levels, adherence to CLABSI prevention guidelines, and the impact of training programs.
Additionally, any study limitations (e.g., self-reported data and small sample size) were noted to assess potential biases.
Data Synthesis
A structured spreadsheet was used to document key information from the selected studies. This approach allowed for systematic comparison and thematic analysis, highlighting trends, commonalities, and disparities in the findings.
Quality Appraisal
To assess the quality of the included studies, the Risk of Bias in Systematic Reviews (ROBIS) tool was used. The appraisal focused on study relevance, risk of bias in study identification, and data collection/analysis. The studies were rated for quality based on the following:
Study Relevance: All studies were relevant, but there was variation in methodology. Risk of Bias in Study Identification Bias in Data Collection and Analysis: Several studies relied on self-reported data, contributing to potential reporting bias.
An overall moderate risk of bias was determined for the systematic review due to the methodological limitations of the included studies as in Table 3.
Summary of Quality Appraisal.

Ethical Considerations
As a systematic review that analyzed published studies, no ethical approval was required. All included studies were evaluated for ethical compliance. The review adhered to PRISMA guidelines to ensure transparency and integrity. Conflicts of interest in the selected studies were disclosed to maintain objectivity, and all data used were properly cited.
This methodology ensures a comprehensive, systematic approach to synthesizing existing research on ICU nurses’ knowledge and adherence to CLABSI prevention guidelines, providing a reliable understanding of the current status in hospital settings.
Results
Knowledge and Adherence Gaps
Across the reviewed studies, significant gaps in ICU nurses’ knowledge and adherence to CLABSI prevention protocols were consistently identified. Almalki et al. (2023) reported that while ICU nurses achieved a moderate overall knowledge score of 71%, only 20% scored above 90%, and just 8% answered all questions correctly. This underscores a key issue: despite possessing some foundational knowledge, many ICU nurses do not demonstrate high levels of proficiency in CLABSI prevention practices. These findings suggest that substantial improvement is needed, as partial knowledge alone is insufficient to ensure safe and consistent clinical practice. This conclusion is supported by previous studies, which have shown that knowledge alone does not necessarily lead to adherence to clinical protocols (Aloush & Alsaraireh, 2018; Dube et al., 2020). The results point to the need for targeted educational interventions to address knowledge deficits and improve the overall quality of care.
Similarly, adherence to CLABSI prevention guidelines was found to be suboptimal across multiple studies. Almalki et al. (2023) and Aloush and Alsaraireh (2018) both found that only about 5% of nurses fully adhered to CLABSI prevention protocols, despite being aware of them. This highlights a critical gap between awareness and implementation, which may be attributed to factors such as time constraints, heavy workloads, or inadequate reinforcement of protocols in clinical settings. These findings are consistent with those of Xiumen Chi et al. (2020), who also reported that practical barriers often hinder adherence, even among nurses with adequate knowledge.
Training and Education
A recurring theme across the studies was the critical importance of continuous and standardized training for ICU nurses. Xiumen Chi et al. (2020) and Dang (2023) emphasized that evidence-based training programs are essential for providing nurses with current knowledge and practical skills necessary for effective CLABSI prevention. Enhancing these programs is vital to addressing the knowledge deficits and poor adherence identified in the literature. Dube et al. (2020) and others demonstrated that targeted CLABSI-focused training can significantly improve adherence to prevention protocols. These findings underscore the need to integrate structured educational interventions into routine professional development, as they are key to improving both knowledge and compliance among ICU nurses.
Infection Risks and Prevention Strategies
The studies also highlighted the increased risk of CLABSI associated with specific clinical practices, such as concurrent use of CVCs and the placement of femoral catheters. Both Dube et al. (2020) and Toor et al. (2022) emphasized that these practices significantly contribute to higher CLABSI rates. Notably, Toor (2022) found that CLABSI incidence was significantly higher in medical-surgical units compared to ICUs, suggesting that different healthcare settings may require tailored prevention strategies. These findings reinforce the need to focus CLABSI prevention protocols on high-risk scenarios—particularly through careful management of central lines and minimizing the use of femoral catheters unless absolutely necessary.
Biomarkers and Diagnostic Tools
An interesting finding from the studies was the role of biomarkers, particularly Procalcitonin (PCT), in diagnosing and managing CLABSI. Madhura et al. (2021) and Akaishi et al. (2023) reported that elevated PCT levels were associated with gram-negative infections in CLABSI patients, particularly in high-risk groups such as those undergoing hemodialysis. PCT has the potential to serve as an early diagnostic tool for CLABSI, allowing for quicker intervention and potentially improving patient outcomes. This could be especially valuable in settings where CLABSI risks are high and timely diagnosis is critical. The use of biomarkers alongside clinical observation might serve as an additional layer of defense in preventing and managing infections.
Prevalence and Microbial Profiles
Akaishi et al. (2023) and Dube et al. (2020) identified Staphylococcus epidermis as the most commonly detected pathogen in CLABSI cases. This bacterium is frequently associated with infections in patients with central venous access devices, aligning with the focus of this review. Additionally, both studies found that CLABSI patients often exhibited lower white blood cell (WBC) counts and C-reactive protein (CRP) levels, which underscores the need for improved diagnostic methods to detect infections, particularly in the early stages. These microbial profiles further emphasize the need for enhanced prevention strategies, including prompt identification and microbial testing, to better manage infection risks.
Tool Validation for Knowledge, Attitude, and Practices (KAP)
The validation of the CLABSI-KAP-Q questionnaire by Dang (2023) provided a reliable tool for assessing ICU nurses’ knowledge, attitudes, and practices regarding CLABSI prevention. This tool, through its systematic approach to data collection, allows healthcare organizations to assess knowledge gaps and identify areas for targeted interventions. It is an essential resource for designing educational programs aimed at improving nurses’ adherence to evidence-based guidelines and can be used to monitor progress over time.
Summary of Results
The body of research on preventing CLABSIs has been systematically categorized and synthesized based on studies retrieved from three major databases: Google Scholar, Scopus, and PubMed. The key findings are as follows: ICU Nurses’ Knowledge of Guidelines: Four studies reported that ICU nurses exhibited a moderate level of understanding of evidence-based guidelines for CLABSI prevention. However, significant gaps in knowledge remain regarding the detailed implementation of best practices. Effectiveness of the CLABSI Bundle: Five studies confirmed the effectiveness of the CLABSI bundle in significantly reducing infection rates across a variety of healthcare settings. These findings underscore the importance of standardized, evidence-based protocols in mitigating the incidence of CLABSIs. Incidence of CLABSIs: Three studies focused on the prevalence and incidence of CLABSIs, offering valuable insights into its occurrence and trends, particularly within intensive care unit (ICU) populations. Measuring Knowledge, Attitudes, and Practices: One study specifically explored methodologies for assessing ICU nurses’ knowledge, attitudes, and practices related to CLABSI prevention. This approach provides valuable tools for evaluating adherence to prevention guidelines and identifying areas in need of improvement. Risk Factors for CLABSI: Two studies examined patient-specific risk factors associated with CLABSI, particularly in ICU and pediatric oncology patients. These studies identify critical factors that heighten the susceptibility to infection and call for more personalized prevention strategies. Blood Culture Results in CLABSI: Two studies investigated blood culture profiles in CLABSI patients, providing insights into microbial patterns. These findings emphasize the importance of early identification and microbial testing in the clinical management of CLABSIs. Protocols in Hemodialysis Patients: Three studies explored preventive protocols in hemodialysis patients, focusing on central venous catheter management. These studies suggest that targeted strategies in this patient population are essential for reducing the risk of CLABSIs. Preventing Nosocomial Infections: One study addressed broader nosocomial infection prevention strategies, including measures aimed at reducing CLABSIs in hospital settings, highlighting the systemic nature of infection control efforts. Use of Two CVCs: Two studies evaluated the use of two CVCs and their appropriate duration, offering recommendations for minimizing CLABSI risk associated with this practice.
Discussion
The reviewed studies consistently emphasize the challenges that ICU nurses face in preventing CLABSIs, despite the availability of well-established national and international guidelines. CLABSIs remain a significant concern in healthcare settings, especially in intensive care units (ICUs), where patients are more vulnerable due to the prolonged use of CVCs. The findings from the studies reviewed provide valuable insights into gaps in knowledge, adherence, and the need for systematic changes in training, institutional protocols, and diagnostic practices to address CLABSIs more effectively.
A key finding across the studies is the gap between knowledge and adherence to CLABSI prevention protocols. While ICU nurses demonstrated a moderate understanding of CLABSI prevention (e.g., 71% correct responses in Almalki et al., 2023), full adherence to evidence-based guidelines remained suboptimal. The study by Almalki et al. (2023) found that only 5% of nurses fully adhered to the guidelines, which points to a disconnect between theoretical knowledge and practical application. This trend was also noted by Aloush and Alsaraireh (2018), who observed variability in compliance across different hospitals. These findings suggest that knowledge alone does not ensure adherence to guidelines, highlighting the necessity of addressing underlying factors such as workload, institutional culture, and lack of reinforcement in clinical practice. This is consistent with literature that stresses the need for consistent, standardized education and training tailored to the needs of ICU nurses (Chi et al., 2020; Dang, 2023).
In practice, the gap in knowledge is particularly concerning because adherence to simple but crucial prevention protocols—such as hand hygiene, aseptic techniques, and proper catheter insertion and maintenance—has been shown to reduce infection rates significantly. The studies reviewed emphasize that these practices when followed correctly, are effective in reducing CLABSI incidences. As Chi et al. (2020) highlighted, even minor lapses in these practices can lead to significant infections. By bridging the knowledge gap, especially through targeted educational interventions, healthcare institutions can enhance the effectiveness of CLABSI prevention efforts.
A common theme across studies is the need for improved and standardized educational programs for ICU nurses. Studies by Xiumen Chi et al. (2020) and Dang (2023) emphasized the importance of evidence-based, structured training that can effectively address both the knowledge and practice gaps observed in ICU nurses. Dang (2023) further contributed by introducing the CLABSI-KAP-Q questionnaire, which provides a robust tool for assessing ICU nurses’ knowledge, attitudes, and practices regarding CLABSI prevention. Such tools are valuable in identifying specific areas where nurses require further education and can help shape more focused and effective educational interventions. Regular audits and feedback can complement these efforts by providing nurses with real-time performance assessments and fostering a culture of continuous improvement.
The findings also suggest that institutional support is critical in ensuring that educational programs are not only available but integrated into the routine professional development of ICU nurses. Regularly scheduled training sessions, combined with clear guidelines and institutional reinforcement, can ensure that nurses are well-equipped to implement evidence-based practices consistently. In this context, leadership plays a pivotal role in fostering a culture that prioritizes infection control and the continuous professional growth of nursing staff.
Several studies highlighted the role of patient-specific factors and CVC management in the prevention of CLABSI. Dube et al. (2020) and Toor et al. (2022) pointed out that practices such as concurrent CVC use and femoral catheter placement were linked to higher CLABSI risks. The findings underscore the importance of tailored interventions that focus on patient-specific risks, such as the type of CVC used or the presence of underlying conditions like chronic kidney disease (CKD). These insights suggest that infection control strategies should be dynamic and flexible, adapting to different clinical contexts and taking into account the unique risks posed by various catheter types or patient conditions.
The studies also emphasize the importance of institutional policies that govern catheter management practices. Standardizing procedures for catheter replacement and insertion, as well as the use of specific infection control checklists, such as the CLIP forms mentioned by Toor et al. (2022), is essential in reducing the likelihood of CLABSI. However, these practices must be universally applied across healthcare settings, as variability in compliance has been observed in some studies (Aloush & Alsaraireh, 2018). This suggests that healthcare organizations must establish clear, comprehensive guidelines for CVC management, monitor adherence, and create mechanisms for continuous improvement to minimize infection risks.
A promising advancement in CLABSI management discussed in the studies is the use of biomarkers, particularly Procalcitonin (PCT), for early diagnosis. The study by Madhura et al. (2021) demonstrated that elevated PCT levels were associated with gram-negative infections in CLABSI patients, particularly in those with CKD. Biomarkers such as PCT have the potential to enhance early detection and differentiation of infections, enabling timely intervention before the infection spreads or becomes more severe. This is particularly critical in high-risk populations, such as CKD patients, where delayed diagnosis and treatment can have severe consequences.
Integrating biomarkers like PCT into routine clinical practice could revolutionize the approach to CLABSI diagnosis. By facilitating quicker identification of infections, biomarkers can not only improve the effectiveness of treatment but also reduce the duration of hospital stays, patient suffering, and healthcare costs. However, further research is needed to validate the efficacy of biomarkers in large-scale clinical trials and determine how they can be most effectively incorporated into existing infection control protocols.
The importance of institutional support and leadership cannot be overstated. Studies such as those by Almalki et al. (2023) and Dang (2023) highlighted that higher levels of knowledge and better adherence to CLABSI prevention guidelines were associated with factors such as nurses’ age, experience, and participation in prior educational interventions. This suggests that hospital leadership plays a critical role in improving nurses’ adherence to CLABSI prevention protocols. By fostering a supportive environment through continuous professional development, ensuring that resources are available for regular training, and establishing clear policies on infection control, hospital leadership can make a significant impact on reducing CLABSI rates.
The findings from the studies reviewed contribute to the growing body of knowledge on CLABSI prevention by highlighting key barriers and solutions related to knowledge gaps, adherence issues, and infection control strategies. The development of reliable tools like the CLABSI-KAP-Q questionnaire presents an opportunity for healthcare institutions to systematically assess and address deficiencies in nurses’ knowledge, attitudes, and practices.
Practically, these findings underscore the importance of integrating evidence-based practices, such as hand hygiene, proper catheter management, and the use of biomarkers, into routine clinical care. Hospitals should prioritize the development and implementation of institutional policies that align with national guidelines while accounting for specific patient and healthcare setting characteristics. Moreover, leadership must support these initiatives by ensuring that ICU staff receives regular training and feedback, which can be reinforced through audits and performance reviews.
Future research should focus on identifying specific barriers to adherence within different hospital contexts, as well as exploring the long-term effectiveness of training programs, diagnostic tools, and biomarkers in reducing CLABSI rates. Investigating the impact of leadership support and institutional culture on adherence to infection control practices is also an important area for future studies. Such research will contribute to the creation of more targeted, evidence-based interventions aimed at reducing CLABSI incidence and improving patient outcomes.
Conclusion
ICU nurses face considerable challenges in adhering to CLABSI prevention guidelines, but there is significant potential for improvement through targeted educational programs, institutional support, and the integration of evidence-based practices. The reviewed studies highlight the critical need for addressing knowledge gaps, improving guideline compliance, and utilizing innovative diagnostic tools to reduce CLABSI incidence and enhance patient safety. By addressing these challenges through a comprehensive approach—combining education, leadership, policy development, and early detection—healthcare systems can achieve more sustainable and impactful reductions in CLABSI rates. Future research should continue to explore effective strategies to overcome barriers to adherence and ensure that CLABSI prevention efforts are both effective and sustainable.
Nursing Implications
The findings of this study suggest that regular training programs should be developed and implemented to enhance ICU nurses’ knowledge and skills in preventing CLABSIs. Continuous education and skill reinforcement are essential for ensuring adherence to best practices and improving patient outcomes.
Nursing policymakers and hospital administrators must identify and mitigate barriers that hinder the implementation of evidence-based guidelines, such as high workloads, shortages of necessary equipment, and the lack of CLABSI prevention workshops. Addressing these challenges is crucial to enhancing nursing practice, strengthening infection control measures, and ultimately reducing CLABSI rates in healthcare settings.
Footnotes
Acknowledgements
The authors acknowledge the midwives who participated in the study.
Ethical Considerations
Ethics approval was obtained from the University Ethics Review Committee (ppu.nur-48/01/24).
Consent to Participate
Informed consent was obtained from each participant with an assurance of anonymity and confidentiality.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this study would be available upon reasonable request from the principal investigator.