
Abstract
Introduction
Research shows low health confidence predicts poor involvement in self-care and is associated with increased use of costly healthcare services. To improve overall health and reduce health inequities, the relevance and urgency of identifying the relationship between social determinants of health and health confidence are great.
Objective
This study explored relationships between social determinants of health and health confidence in adults at an urgent care center in southern California.
Methods
The descriptive cross-sectional study collected data via survey from 240 English- and Spanish-speaking adults (18–93 years) receiving care for any medical condition between 15 and 17 August 2022. Patients in need of immediate medical attention were excluded. The survey encompassed The PRAPARE screening instrument, sociodemographic questions, and a single health confidence question. Bivariate analysis identified significant differences in health confidence for a logistic regression model.
Results
Forty-seven percent (n = 107) of participants reported low confidence in managing their health and well-being. Low health confidence was observed in those with unmet needs (χ2 = 4.16, p = .042), and varying levels of stress (χ2 = 13.76, p = .008). Low health confidence was common in low-income (t = 2.23, p = .028) and greater social risk groups (χ2 = 19.7, p < .001). Participants in contact with friends or family 1 to 5 times per week (vs. >5 times) were more likely to report low health confidence; those with high levels of stress were more likely to report low health confidence (vs. no stress).
Conclusion
This study highlights the insidious prevalence of social determinants of health and the impact of social isolation and stress on health confidence, providing the basis for implementing standardized social determinants of health screening.
Introduction
Social determinants of health (SDOH) are the conditions in which people live, work, and grow, influencing their health, well-being, and quality of life (Office of Disease Prevention and Health Promotion [ODPHP], n.d.). A safe environment, economic stability, opportunities for personal growth, employment, an active social environment, and a healthy lifestyle impact health status and account for 30%–55% of health outcomes (World Health Organization [WHO], 2023). The WHO and Healthy People 2030 recognize that SDOH is closely associated with health and well-being and have made addressing modifiable SDOH a priority (ODPHP, n.d.; WHO, 2023). Yerramilli et al. (2024) note investing in health equity and social determinants shows significant health and financial returns.
The Affordable Care Act recognizes patient involvement in healthcare is vital to healthcare reform (Hibbard & Greene, 2013). Health confidence refers to patients’ capacity to manage an illness (Wasson et al., 2018), and includes several overlapping concepts—patient engagement, activation, empowerment, and self-efficacy (Bleacher et al., 2020). Consequently, health confidence is an actionable proxy measure for patient health management with studies estimating 50% of patients have low health confidence (Health Confidence Academy, 2023). The result of low levels of health confidence and poor self-care increases the cost of services (Benson et al., 2019; Hibbard & Greene, 2013; Wasson, 2013). In contrast, high health confidence results in better management and control over chronic diseases by adhering to prescribed treatment regimens, performing regular self-monitoring at home, and attending follow-up appointments (Hibbard & Greene, 2013), resulting in improved health and decreased healthcare costs. Nevertheless, further clarity is needed in understanding the relationships among SDOH, health confidence, and health management of chronic disease risk.
Review of Literature
Despite the consensus that SDOH affects patient and population health, data has been scarce due to limited standardized methods to screen for social needs (Weir et al., 2020). In the United States, most social needs research has taken place in community health centers with a historical precedent for addressing SDOH as a core tenant of primary care (Gottlieb et al., 2018). Notably, although SDOH are strong predictors of morbidity and mortality, it is challenging for healthcare systems to integrate nonmedical factors into their data and develop interventions for care. Nonetheless, in Veteran Administration Hospitals, research has found increased emergency department (ED) use among those with social risks (Davis et al., 2020). In 2018, only 24% of U.S. hospitals and 16% of U.S. medical practices reported screening for all social needs (food insecurity, housing instability, utility and transportation needs, and interpersonal violence; National Association of Community Health Centers [NACHC], 2019a). Physician practices serving disadvantaged patients were more likely to screen for all five social needs (NACHC, 2019a). Among commercially insured populations, patients with social needs were more likely to ration or delay care, engage in unhealthy behaviors, and experience diminished physical and behavioral health (Pera et al., 2021; Sherman & Stiehl, 2018). Low-wage earners were three times more likely to visit the ED (Pera et al., 2021), used preventative services 50% less, and had four times more avoidable hospital admissions than high-wage earners (Sherman et al., 2017). Such trends suggest adverse SDOH also affects those with employer-sponsored insurance and supports the need for social needs screening in different populations and settings. Although barriers to social needs screening exist (lack of resources, time, and incentives), early identification can connect patients with services (NACHC, 2019a). Nurses at the forefront of healthcare delivery are in contact with diverse patients, performing a critical role in addressing healthcare inequities, and are well positioned to initiate social need screening, which can improve patient outcomes and decrease healthcare costs.
In 2013, the NACHC, Association of Asian Pacific Community Health Organizations, Oregon Primary Care Association, and Institute for Alternative Futures developed, implemented, and promoted a national standardized patient SDOH risk assessment protocol—The PRAPARE screening instrument (Fraze et al., 2019; NACHC, 2019b, 2019c). Since 2016, PRAPARE has become the dominant social risk assessment for social needs across community health centers nationally (NACHC, 2019b). Research is needed to examine the acceptability of social needs screening in different settings, with different patient populations (Gottlieb et al., 2018), as social needs screening is not routinely done at healthcare encounters (NACHC, 2019a).
Purpose. To provide further clarity, the current study examined the relationships among SDOH, chronic disease risk factors, and the health confidence of adults seeking care at a southern California healthcare center. The social–ecological model (McLeroy et al., 1988) provided the framework for examining how SDOH impacts health confidence. The model emphasizes the interplay between individual, interpersonal, institutional, community, and policy levels and how these factors create barriers to accessing care (McLeroy et al., 1988). Understanding these interconnected factors by using standardized social needs screening is essential for addressing health disparities, promoting health equity, and reducing healthcare costs (Centers for Disease Control and Prevention [CDC], 2024). To improve overall health and reduce health inequities in a postglobal pandemic and unprecedented inflation rates, the relevancy and urgency to identify SDOH affecting health confidence are of the utmost importance.
Methods
Study Design and Setting
This descriptive cross-sectional study examined relationships between SDOH and health confidence in adult patients of any age receiving care at an urgent care center in southern California. This center is affiliated with a large integrated healthcare delivery system serving 12.5 million members in eight states and the District of Columbia. The urgent care setting was chosen to efficiently recruit a large number of diverse participants within the three-day data collection time frame. Moreover, urgent care centers serve a diverse population, providing access to individuals across a wide range of ages and presenting with various medical conditions, ensuring a representative sample for the study. The sample size was calculated based on a priori power analysis using G*Power 3.1.9.7 (Faul et al., 2007). The minimum required sample size to achieve 80% power for detecting a medium effect size at a significance criterion of α = .05 and 12 predictors was 127.
Participants
A purposive sample of participants was recruited and enrolled from an urgent care center in Southern California between 15 and 17 August 2022. The inclusion criteria were English- and Spanish-speaking patients aged 18 and older with any chief complaint. Patients in need of immediate medical attention were excluded from participating, as were those who spoke a language other than English or Spanish due to the limited availability of bilingual/bicultural research associates and resources for translation services. After the three-day recruitment period, 240 adults were enrolled in the study. Approximately 5% of patients declined participation.
Procedures
The research team screened all patient check-ins for eligibility. Eligible patients were recruited in person by the research team, receiving a brief explanation of the study in a private section of the waiting room. An informational poster in English and Spanish was also placed at the urgent care center entrance, directing interested patients to speak with the research team. Those interested in participating were consented to the study, and provided with the self-administered PRAPARE questionnaire, supplemental survey, and community resource list in their preferred language. Assistance in completing the questionnaires was provided as needed. Surveys were collected and validated for completion by the research team and stored in a secured location. Participation consisted of a one-time 20–30-min study visit, with participants receiving a $5 gift card for their time and effort. At the end of the data collection period, all data was downloaded into data management software and securely stored. A consulting statistician had controlled access to the deidentified dataset.
Ethical Considerations
The University of San Diego Institutional Review Board (IRB) reviewed and approved all study procedures to protect human subjects (IRB-2023-5). The study was performed in accordance with the requirements of the Code of Federal Regulations on the Protection of Human Subjects (45 CFR 46 and 21 CFR 50 and 56), including its relevant Subparts. Participants were informed about the study details, including that participation was voluntary and they could withdraw at any time without adverse consequences. A copy of the information sheet was given to participants prior to the initiation of the survey. Confidentiality of the collected data was maintained.
Measures
The PRAPARE screening instrument is a national standardized patient risk assessment tool designed to engage patients in evaluating and addressing SDOH (NACHC, 2019b). It consists of four core domains—personal characteristics (race, ethnicity, farmworker status, language preference, veteran status), family and home (housing status and stability, neighborhood), money and resources (education, employment, insurance, income, material security), and social and emotional health (transportation, social isolation, stress). The instrument was developed and validated using the eight Gold Standard stages of measure development (Fraze et al., 2019). It is written in fourth-grade literacy level and takes <10 min to administer (NACHC, 2019b). One item is, What is your housing situation today? I have housing. I do not have housing (staying with others, in a hotel, in a shelter, living outside on the street, on a beach, in a car, or in a park). I choose not to answer this question. Stress is when someone feels tense, nervous, anxious, or can’t sleep at night because their mind is troubled. How stressed are you? Not at all. A little bit. Somewhat. Quite a bit. Very much. I choose not to answer this question.
The PRAPARE risk tally scoring methodology created by the original developers was utilized (NACHC, 2019a). A total score was obtained by adding the number of positive responses across all questions (NACHC, 2019a). Each response is assigned a value based on its risk level. For instance, stable housing is scored 0 (no risk), temporary housing is scored 1 (moderate risk), and homelessness is scored 2 (high risk). Similar scoring is applied across other domains. Scores range from 0 to 22, with increasing values representing a greater number of social risks (NACHC, 2019c).
The supplemental survey was developed by the researcher to collect participants’ age, gender, chronic disease history (diabetes, hypertension, cancer, stroke, arthritis, obesity), chronic disease risk factors (tobacco and alcohol use, physical activity), and health confidence score (Figure 1).

Social–Ecological Model for Understanding Differential Impact of COVID-19. Adapted from “An Ecological Perspective on Health Promotion Programs” by K. R. McLeroy, D. Bibeau, A. Steckler, & K. Glanz, 1988. Health Education Quarterly, 15(4), pp. 351–377. https://doi.org/10.1177/109019818801500401.
Health confidence (included in the supplemental survey) was measured with a single patient-reported risk assessment question in the What Matters Index—“How confident are you that you can control and manage (deal with) most of your health problems?” (Wasson et al., 2018). The question is easy to understand, does not require computation or complex interpretation, is actionable to address patient needs, and requires self-reflection. Direct questioning of health confidence may lead to social desirability bias, thus, patient self-reporting in this indirect way can minimize bias (Wasson & Coleman, 2014). The measure can be scored as a 10-point scale (“not very confident” to “very confident”) or a three-response variable (“very confident,” “somewhat confident,” and “not confident”). This version is easy for patients to quickly interpret and can be used for problem-solving and motivational interventions (Wasson & Coleman, 2014). This study utilized the three-response category for data collection and subsequently dichotomized the variable to simplify data analysis and interpretation, grouping “somewhat confident” and “not very confident” into one variable “low health confidence.”
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 28. All study variables were examined for normality, missing values, and outliers; test assumptions were evaluated and addressed as needed. Descriptive statistics (frequency, percent, mean, standard deviation, range) were used to characterize the sample, and chi-square (or Fisher's exact) tests and t-tests to detect differences in groups. Variables important in the literature and significant at p < .05 in the bivariate analysis were considered for entry into a binomial logistic regression to identify factors that contribute to health confidence.
Results
Sociodemographic and clinical characteristics (N = 240) are presented in Table 1. All participants had health insurance. Almost two-thirds were women (59.5%, n = 136). The mean age was 49 years (SD = 17.79, range = 18–93). About two-thirds self-identified as Hispanic or Latino (60.7%, n = 145). Only 5% were veterans and 1.3% reported seasonal or migrant farm work as their or their family's primary source of income. Most lived with one or more family members; 13.1% (n = 30) lived alone. About half spent time with family and friends at least 1–5 times a week (50.9%, n = 110); 34.3% spent time with family and friends almost daily. Although 96.4% (n = 217) had housing and 87.8% (n = 201) reported a stable housing situation, 23.2% (n = 51) reported a number of unmet needs, such as food, clothing, utilities, childcare, medicines or healthcare, phone, and other. Only 20.4% reported having no stress, with 19.5% (n = 44) reporting having quite a bit of it and 12.4% (n = 28) very much stress. The commonest chronic condition was hypertension (20.6%, n = 47). Consistent with the literature (Benson et al., 2019; Hibbard & Greene, 2013; Wasson, 2013), 47.1% (n = 107) reported low levels of health confidence in managing their own health and well-being.
Social Determinants of Health, and Clinical Characteristics of Study Population by Health Confidence.
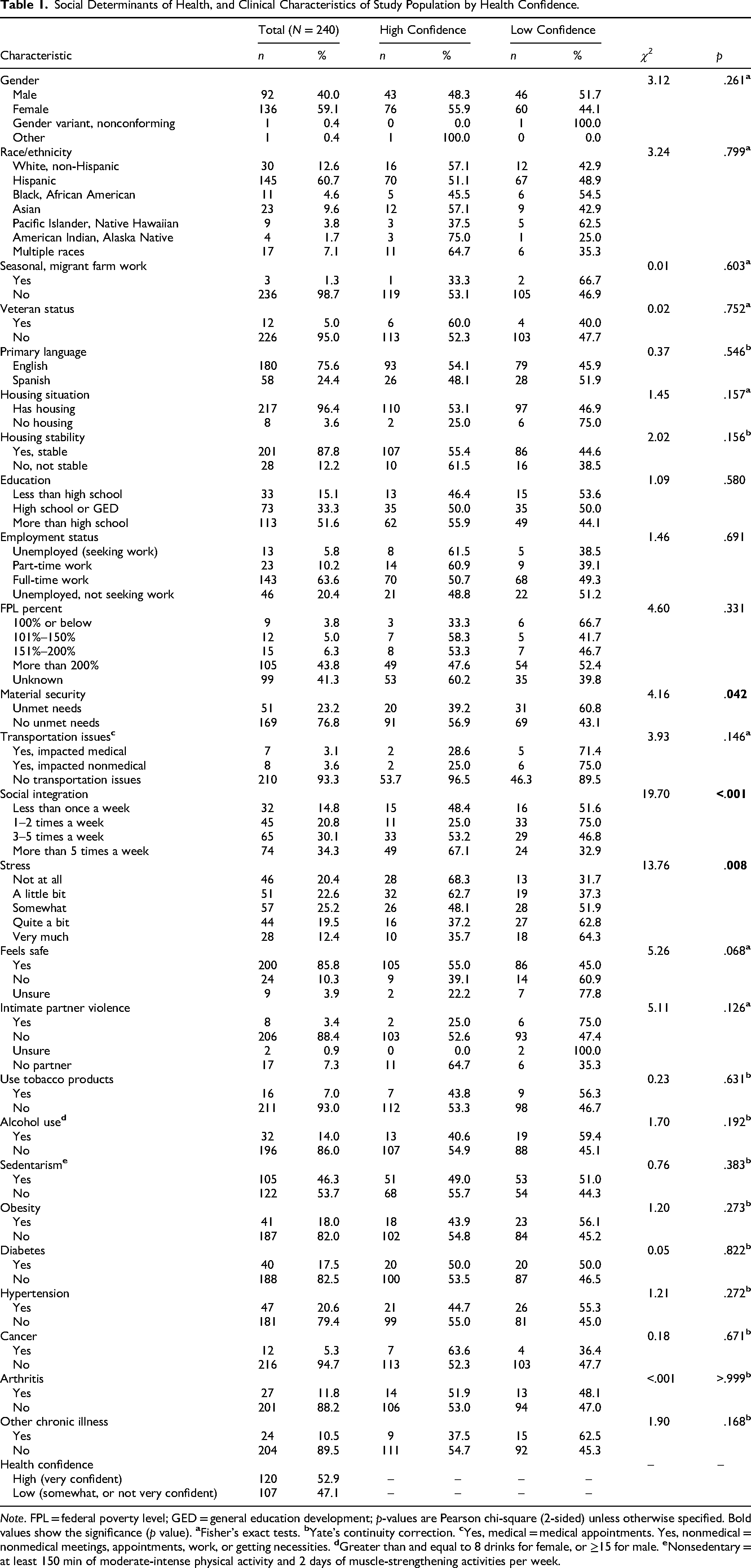
Note. FPL = federal poverty level; GED = general education development; p-values are Pearson chi-square (2-sided) unless otherwise specified. Bold values show the significance (p value).
SDOH and Health Confidence
The distribution of SDOH by health confidence is presented in Table 1. Chi-square (or Fisher's exact) test showed health confidence was different in terms of material security (χ2 = 4.16, p = .042), social integration (χ2 = 19.70, p < .001), and stress (χ2 = 13.76, p = .008). Higher prevalence of low health confidence was observed for patients with unmet needs (60.8%, n = 31), patients who spend time with family 1–2 times per week (75%, n = 33), and patients with quite a bit (62.8%, n = 27) or very much stress (64.3%, n = 18); no other significant differences were found.
Independent samples t-test results are presented in Table 2. Results showed patients low in health confidence had lower incomes (M diff. of $22,628, p = .028) and higher social risk scores (PRAPARE score; M diff. of 1.23 points; 95% CI [0.52, 1.94], p < .001) than those with higher incomes and lower social risks scores.
Social Determinants of Health, Sociodemographic, and Clinical Characteristics of Study Population by Health Confidence.

Note. PRAPARE = Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences; USD = U.S. dollars. Bold values show the significance (p value).
Correlates of Low Health Confidence
The results of the binomial logistic regression are presented in Table 3. Adjusting for income, material security, and SDOH risks—significant in the bivariate analysis—evidenced the significant influence of participants’ social integration and stress level on health confidence. Participants seeing or talking to close ones 1–2 times per week (Adj. OR = 4.48, 95% CI [1.42, 14.22], p = .010) and 3–5 times per week (Adj. OR = 2.79, 95% CI [1.01, 7.77], p = .049) were more likely to report a low level of health confidence than those seeing or talking to close ones more than 5 times per week. Participants with quite a bit of stress (Adj. OR = 4.29, 95% CI [1.05, 17.51], p = .042) were more likely to report a low level of health confidence than those with no stress. Notably, the PRAPARE score—sum of all risk factors in the personal characteristics, family and home, money and resources, and social and emotional domains—did not uniquely contribute to health confidence. The presence of social integration and stress as unique factors may have masked the impact of the overall score on health confidence in the multivariate analysis.
Summary of Logistic Regression Analysis Predicting Low Health Confidence (N = 240).

Note. CI = confidence interval for odds ratio (OR); PRAPARE = Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences; USD = U.S. Dollars.
Discussion
To better understand the relationship between social needs and health confidence, this descriptive cross-sectional study targeted adults receiving care at an urgent care center in southern California. The Social Ecological Model—which postulates that health-related behaviors are not only determined by biological factors but also by multiple interrelated factors occurring at various levels—provided the theoretical underpinning for the study (Harvard Medical School. Medical Student COVID-19 Action Network, 2021; McLeroy et al., 1988). Social determinants at the individual, interpersonal, and community levels influence patients’ health confidence and should guide strategies to address their social needs (Poux, 2017).
Despite most participants reporting high levels of social integration, stable housing, and employment, and no transportation issues, almost half reported low confidence in managing their health and well-being. This finding aligns with research indicating that 25%–50% of the patient population has low levels of health confidence (Benson et al., 2019; Bleacher et al., 2020; Hibbard & Greene, 2013; Wasson, 2013). Low health confidence was observed for participants with unmet needs, low income, social isolation, and stress; stress was present for about 80% of participants. When controlling for income and material security (significant in the bivariate analysis), social isolation and stress uniquely contributed to low health confidence in this population. Unfortunately, the specific social isolation and stress factors impacting health confidence or the relationship between social isolation/integration and stress were not assessed; yet results support the need for SDOH screening. In addition, the prevalent impact of unmet material needs (and income) on health confidence is consistent with published literature (Bleacher et al., 2020), and provides an opportunity to intervene. In this study, select social risks were present along with culturally protective factors, exemplifying the dynamic network of interrelated factors occurring at the individual, interpersonal, and community levels (Harvard Medical School. Medical Student COVID-19 Action Network, 2021; McLeroy et al., 1988).
Any screening and intervention efforts should consider the timing, approach, and acceptability of screening in the target population (Dobrow et al., 2018). Nurses at the forefront of healthcare delivery can screen patients for SDOH and health confidence in different settings (urgent care, primary care, at the hospital bed) in a nonjudgmental way when patients are not in acute distress. When at-risk patients are identified, healthcare organizations should adjust the care team composition and establish protocols to facilitate referrals to resources such as social workers, outpatient counseling, chronic disease educators, and community support resources (Weir et al., 2020). Nurses can help educate patients regarding the relationship between social isolation and stress and their effect on health confidence.
Strengths and Limitations
The results should be interpreted within the context of the study's limitations. The study sample was homogeneous with respect to ethnicity, geographic location, and socioeconomic status; not randomly selected. The setting was an urgent care center affiliated with a large integrated healthcare delivery system, and it may not be generalizable to the noninsured population. Most SDOH studies have been conducted in primary care or emergency room settings, rather than an urgent care setting treating acute episodic conditions. To our knowledge, there is no previous research on health confidence in the urgent care setting. Visiting urgent care for an acute episodic event may affect patients’ perception of health confidence, with results biased toward low health confidence, as compared to patients attending preventative care visits.
Despite limitations, the study is novel in exploring social needs and health confidence. Our research data suggest the insidious prevalence of SDOH and its impact on health confidence, providing the basis for implementing standardized SDOH screening. Further research on social needs and health confidence requires patient engagement and participation with sufficient representation from underserved populations. Changes in care team composition as well as healthcare provider understanding of the benefits of SDOH screening are needed to address inequitable access and significantly varied patient experiences (Benson et al., 2019; Hartman et al., 2021; Health Confidence Academy, 2023; Hibbard & Greene, 2013; Wasson, 2013). Healthcare organizations are increasingly recognizing the need for multidisciplinary care teams—primary care physicians, behavior health specialists, pharmacists, community and social workers, care coordinators, case managers, community-based organizations, and data analysts—to successfully address patients’ social determinants (Heath, 2024).
Implications for Practice
The findings emphasize the importance of implementing SDOH screening to improve health confidence. Screening should occur at multiple points of care, be nonjudgmental, and take place when patients are not in acute distress. Clear referral protocols are essential to connect at-risk patients with social workers, counselors, chronic disease educators, and community resources. Additionally, larger descriptive studies should explore how social integration and stress management affect health confidence and whether increased provider awareness and early referrals enhance patient outcomes. Qualitative research is also needed to capture patient perspectives on SDOH screening and health confidence.
Conclusion
This study highlights the relationship among SDOH, demographics, chronic disease risk factors, and health confidence in adults seeking care. In this study, patients with unmet social needs reported lower health confidence, influenced by limited social integration and higher stress levels. Healthcare professionals play a critical role in screening for SDOH in various healthcare settings. The results of this study highlight the need for ongoing education on SDOH screening, optimal adjustments to care team composition, effective referral protocols, and the influence social factors have on health confidence. Policies should focus on the timing and periodicity of screenings, referral process, and funding for SDOH training. Staffing strategies must prioritize equipping nurses with the skills to address unmet social needs effectively, ultimately enhancing health confidence and reducing health inequities and the use of costly healthcare services.
Supplemental Material
sj-docx-1-son-10.1177_23779608251344038 - Supplemental material for Social Determinants of Health and Health Confidence: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608251344038 for Social Determinants of Health and Health Confidence: A Cross-Sectional Study by Laura Truman, Patricia Calero, Caroline Etland, Razel B. Milo and Cynthia D. Connelly in SAGE Open Nursing
Supplemental Material
sj-pdf-2-son-10.1177_23779608251344038 - Supplemental material for Social Determinants of Health and Health Confidence: A Cross-Sectional Study
Supplemental material, sj-pdf-2-son-10.1177_23779608251344038 for Social Determinants of Health and Health Confidence: A Cross-Sectional Study by Laura Truman, Patricia Calero, Caroline Etland, Razel B. Milo and Cynthia D. Connelly in SAGE Open Nursing
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.