
Abstract
Background
Pressure injury is a preventable public health problem. It may develop due to intense force or force combined with shear. Pressure injuries may be associated with pain and increased length of hospital stay. Adequate knowledge and a positive attitude of nurses are required to prevent pressure injuries. Evidence on pressure injury prevention in Ghana among nurses is limited.
Aims and Objectives
The study examined factors associated with nurses’ knowledge and perceived barriers toward pressure injury prevention in the Tamale metropolis, Ghana.
Methods
This was a multi-center descriptive cross-sectional study that recruited 216 nurses using systematic random sampling method. Data were collected using a self-administered questionnaire and analyzed using the R package and Statistical Package for Social Scientists (SPSS) version 27.0. After controlling for covariates, regression analysis determined the predictors of knowledge and attitude toward pressure injury prevention.
Results
More than two-thirds (79%) of nurses demonstrated good knowledge regarding pressure injury prevention. However, a significant majority (94%) exhibited poor attitudes. Notably, nurses employed in teaching hospitals [aRR = 2.09 (95%CI: 1.31, 3.44), p = .002] and those with 2–4 years of work experience [aRR = 1.96 (95%CI: 1.23, 3.22), p = .004] were significantly more likely to possess good knowledge about pressure injury prevention. Conversely, nurses without prior education on pressure injury prevention [aRR = 0.48(95%CI: 0.23, 0.98), p = .041) were less likely to prevent it. The most perceived barriers were inadequate equipment and logistics and insufficient time/increased workload.
Conclusion
While nurses exhibited a good knowledge about pressure injury prevention, their attitude toward its prevention was poor, indicating significant gaps that need addressing. Developing a comprehensive pressure injury management document and promoting attitudinal change through continuing professional capacity development may prove timely. The findings highlight the need for addressing organizational barriers that hinder effective nursing practice to improve the quality of care and positive patient outcomes.
Keywords
Background
Pressure injury (PI) or ulcer is damage to a localized area of the skin, or soft tissues, especially bony prominences, caused by intense force or force combined with shear (Kottner et al., 2020). It arises from a complex interplay of factors, including those associated with dietary status, mobility, activity level, and skin perfusion. PI development has also been linked to factors such as dementia, peripheral neuropathy, advanced age, cardiovascular illnesses, incontinence, immobility, and fractures (Chung et al., 2023; Elli et al., 2022). Pressure injury development may be associated with pain or discomfort, increased length of stay in healthcare centers, and possibly, increased morbidity (Nguyen et al., 2015; Nuru et al., 2015).
The declaration of the prevention of PI in Rio de Janeiro noted the importance of its prevention as a universal right, a public health problem, and an adverse event (Soldevilla Agreda, 2012). Pressure injury prevention is, therefore, crucial and a priority function of frontline health staff, especially nurses, because its development may signify poor-quality care (Miller et al., 2017). In this regard, it is an important function of professional nurses to mitigate its occurrence. This can be achieved through many strategies including but not limited to creating awareness, demonstrating comprehensive pressure injury prevention knowledge, fostering a positive attitude toward prevention, enhancing patients’ skin assessment, preserving skin integrity, and preventing skin injuries (Beeckman et al., 2011; Hekmatpou et al., 2018). It is also imperative for nurses to identify patients who are susceptible to developing pressure injuries through the above strategies and implement standardized protocols to prevent any associated complications. As a result, the Nursing and Midwifery Council (N&MC) in Ghana has developed and implemented practice guidelines to assess patients who are at risk to develop PI and protocols to treat pressure injuries, which are all contained in the nursing procedure manual for use by nurses in healthcare settings (Nursing and Midwifery Council, 2024).
Review of Literature
Several studies in low, middle, and high-income countries have evaluated nurses’ knowledge, attitude, and barriers toward pressure injury prevention (Ebi et al., 2019; Fulbrook et al., 2019; Lotfi et al., 2019; Sari et al., 2021; Sham et al., 2020; Tirgari et al., 2018). Descriptive cross-sectional studies in Ethiopia, Iran, and Nigeria have all reported overall poor knowledge scores of PI prevention among nurses (Ebi et al., 2019; Ingwu et al., 2019; Tirgari et al., 2018). Similarly, studies in Australia and China have reported poor knowledge scores that is 54%, 51%, and 57% respectively (Coventry et al., 2024; Liang et al., 2024; N. Song et al., 2024). Furthermore, a study conducted in Sweden among nurse assistants revealed a poorer knowledge score where only 3.4% of the nurses obtained satisfactorily good knowledge score (Bjurbo et al., 2024). In contrast, similar studies conducted in Australia, Saudi Arabia, and Malaysia have shown an overall good nurses’ knowledge score toward PI prevention (Barakat-Johnson et al., 2018; Kaddourah et al., 2016; Sham et al., 2020). Furthermore, a study in Namibia on knowledge, attitude, and practice of pressure injury prevention revealed that the majority (70%) had good knowledge (Abrahams et al., 2023).
On the other hand, nurses’ attitude plays an important role in reducing PI. Nurses must have a positive attitude toward assessment to identify patients who are at risk or have pressure injuries. Studies from Pakistan revealed that attitude scores were generally moderate to good that is 67% and 78% respectively (Muhammad et al., 2017; Ullah et al., 2024). Studies in Saudi Arabia (Kaddourah et al., 2016) and Ethiopia (Etafa et al., 2018) found similar results. However, positive attitude scores were reported in several other studies. For instance, in Namibia (Abrahams et al., 2023) and Australia (Coventry et al., 2024), nurses’ overall attitudes toward pressure injury prevention were positive 78% and 83% respectively. A similar finding was observed in Malaysia where 82% of the nurses portrayed positive attitudes (Bakar et al., 2023).
A lot of factors including demographic and professional greatly influence knowledge and attitude toward pressure injuries. Studies in China, Iran, Indonesia, and Saudi Arabia have revealed that higher educational levels of nurses have resulted in significant knowledge and positive attitudes toward pressure injury prevention (Alshahrani et al., 2023; Liang et al., 2024; Sari et al., 2021; N. Song et al., 2024). Also, demographic factors like age, and gender were associated with knowledge and attitude (Emami Zeydi et al., 2022) while work experience was also a significant factor (Emami Zeydi et al., 2022; Lotfi et al., 2019). In another study, nurses using international PI guidelines as a reference in the operating room, and intervening to prevent pressure injuries during surgery were positively associated with PI prevention (Kaya & Erol Ursavaş, 2023). Furthermore, hospital level, job title, previous training on PI, and the time of last training on PI were significantly associated with knowledge and attitude (Liang et al., 2024).
On the barriers to pressure injury prevention, factors such as increased workload and inadequate training on PI prevention (Ebi et al., 2019; Etafa et al., 2018), shortage of staff, and lack of pressure injury risk assessment scale (Batiha, 2018; Ingwu et al., 2019) and lack of time and unstable patients (Ingwu et al., 2019; Sham et al., 2020) were reported. In Canada, a qualitative study on the facilitators and barriers to pressure injury prevention revealed that knowledge gaps, limited staffing, and lack of funding to support PI prevention were barriers that affected its prevention and management (Cesca et al., 2024) while in China, nurses reported barriers such as lack of priority in PI prevention by the nurses, low priority to PI prevention due to the severity of the patient, competing demands, lack of universal PI prevention guidelines in Chinese language, and difficulty accessing guidelines among others (B. Song et al., 2024).
Despite improvements in global healthcare systems, patients, particularly in low-income countries (LMICs), continue to sustain pressure injuries, which may indicate a lack of quality care. As a low- and middle-income country, there is limited or no research on nurses’ knowledge, attitude, or perceived barriers to pressure injury prevention in Ghana. In the effort to enhance patient care, promote patient safety, and improve overall patient care outcomes, the lack of evidence on pressure injury prevention makes determining nurses’ knowledge, attitude, and identifying barriers toward PI prevention crucial. As a result, the current study examined factors that influence nurses’ knowledge and attitudes and identified the perceived barriers hindering pressure injury prevention in the Tamale metropolis, Ghana. The findings are intended to fill gaps in the literature while also improving nurses’ knowledge and attitudes toward PI prevention. Furthermore, the outcome of this study is likely to help inform policy improvements in professional nursing training in Ghana as well as improve overall patient care.
Methods and Methodology
Study Design
The current study was a multi-center descriptive cross-sectional design that employed a quantitative approach to data collection. The study assessed nurses’ knowledge, attitude, and perceived barriers toward pressure injury prevention in three government health facilities in the Tamale metropolis.
Study Setting
The Tamale Metropolitan Assembly is the administrative capital of the northern region of Ghana. The study was conducted at [Hospital A], [Hospital B], and [Hospital C]. These facilities are tertiary, secondary, and primary levels per the Ghana Health Service (GHS) pyramidal healthcare and referral system levels. The hospitals offer round-the-clock general and specialist care services to the public. Hospital A is an 812-bed capacity referral tertiary health facility. As part of its mandate as a teaching hospital, it serves as a center for training diverse healthcare professionals including postgraduate medical specialization, medical, nursing, and allied health professionals. The hospital sees an average of 340 patients daily and has a total nursing workforce of 1,367. Hospital B is a secondary referral facility with 399 professional and auxiliary nursing staff. Similarly, Hospital C has a 126-bed capacity with a nursing staff population of 410. Data were taken from the medical, surgical, orthopedics, urology, and intensive care units of the hospitals. In all, 544 nurses constituted the target population for this study.
Study Population
The study population was nursing staff drawn from the selected hospitals. The nursing staff were professional nurses (registered general nurses) (RGNs) and auxiliary nurses (registered nurse assistant clinical) (RNAC). The selection of these categories of nurses was based on their scope of practice, thus, they render direct clinical nursing care to patients. The RGNs in Ghana are nurses who have undergone either three years of diploma or four years of Bachelor's nursing training and have been licensed to practice as professional nurses by the Nursing and Midwifery Council (N&MC). The RNAC, licensed by N&MC receives two years of training as a nurse assistant. The target population of nurses in the selected wards from these facilities were [Hospital A = 363], [Hospital B = 79], and [Hospital C = 102], respectively. Find the participants’ sampling procedure below in Figure 1.

Participants’ selection procedure.
Participants Selection Procedure
Sample Size Determination
Three healthcare facilities were sampled purposely in this study. The sample size was determined using the Yamane formula for sample size calculation based on a known population (Yamane, 1973). The Yamane formula is suitable for studies where the population is finite and known. This prevents over or under-sampling. See the formula below.

The final sample size after calculation was 231 nurses. To reduce sample bias and ensure sample representativeness, proportionate sampling was used to determine the number of nurses in each facility. Therefore, the sample size for each health facility was Hospital A (154), Hospital B (34), and Hospital C (43). Power analysis (G*Power) version 3.1.9.7 was used to confirm the sample size using a moderate effect size of odds ratio = 1.8, alpha = 5%, and a priori power of 0.85, a sample of 208 was determined. We added a 10% non-response rate resulting in a total sample of 231.
Sampling Procedure
The nurses were subsequently sampled via a systematic random sampling method. This method was chosen because of its suitability in allowing all the nurses in the various wards/units in the selected facilities an equal opportunity to be part of the study for selection. In the wards, the nurses’ daily attendance books served as registers from which they were selected. The nurses write their names serially on the register starting from the first to the last each day with a date. A sampling interval was then calculated by dividing the total target population (544) for the three facilities over the total sample size (231) for the three facilities (544/231), which yielded 2 as the interval. Therefore, every second nurse on the attendance book was eligible for selection to take part in the study. This was done in each of the wards or units in the selected facilities. Balloting was done to select the first two nurses for the study to determine the start point.
Inclusion and Exclusion Criteria
All cadres of nurses specifically auxiliary (nurse assistant clinical) and registered general nurses (professional nurses) who consented to participate in the study were included. These nurses were carefully chosen due to their core responsibility of rendering clinical nursing care to patients, which includes prevention and management of PI. All student nurses, nurses on national service/rotation, midwives, and public health nurses were excluded.
Study Instrument
The researchers used a structured questionnaire to collect the data based on the study objectives. The questionnaire was structured into four (4) parts. Part one: demographic characteristics and professional information such as age, sex, marital status, religious affiliation, educational level, professional qualification, unit of work, education on PI prevention, source of PI prevention education, and number of years of working experience. Part two consisted of the Pressure Injury Knowledge Test Tool (PUKT). The PUKT questions were developed and validated by (Beeckman et al., 2011). The researchers adapted the PUKT questions from (Beeckman et al., 2011) and (Ebi et al., 2019). The knowledge questions are 25 classified into five subgroups; Etiology and Development (5 items), Nutrition (5 items), Risk Assessment (5 items), Classification and Observation (5 items), and Prevention (5 items). Part three contained 6 attitude questions, and part four consisted of barriers toward pressure injury prevention. Like the knowledge questions, the researchers used validated attitude and barrier questions in line with previous studies (Ebi et al., 2019; Etafa et al., 2018; Ingwu et al., 2019). On the aspect of the attitude, a four-point Likert scale with appropriate descriptions as: 1= “Strongly disagree”, 2= “Disagree”, 3= “Agree”, and 4= “Strongly agree” was used to elicit responses from the nurses. Meanwhile, yes or no questions were asked about knowledge and barriers.
Data Collection Procedure
Data collection commenced after obtaining permission from the study facilities. The data was collected from May to August 2020. Three research assistants (RAs) helped in data collection. Data collection was done during morning and afternoon shifts. Questionnaires were administered directly to the nurses at the wards/units in which they work. Using the nurses’ attendance book to identify eligible nurses, data collectors approached and administered the questionnaires to the nurses at their convenience. After handing over the questionnaires to the nurses, the RAs excused them and only returned for the completed questionnaires based on a schedule with the nurses. This approach promoted privacy and prevented coercion. Using a simple random sampling strategy, all the nurses had equal chances of being selected. Every second nurse on the attendance book was deemed qualified for selection. This approach prevented biases relating to participant selection. Each day after data collection, all questionnaires were cross-checked for completeness before leaving the site. The researchers ensured that all questions were answered and where clarity was needed, it was provided succinctly. All questionnaires were collected upon completion.
Validity and Reliability
All the researchers peer-reviewed the questionnaire to ensure its validity. Moreover, the content of the questions in the questionnaire was reviewed by two nurses with a Doctor of Philosophy degree with a specialization in adult health nursing and four (4) nurse specialists in surgical and critical care nursing. Pretesting and piloting were done among ten nurses from the selected facilities; however, they were not included in the final sampling frame. The piloting and pretesting were done to identify ambiguity and provide clarity to the questions. Cronbach's alpha coefficient was performed to ensure internal scale reliability and it yielded the following scores; knowledge (0.82), attitude (0.61), and barriers (0.85). Although 0.70 is a generally accepted Cronbach alpha (Nunnally & Bernstein, 1978), values of 0.60 have also been accepted in other studies (Black et al., 2010). Therefore, our 0.61 was considered acceptable and was included in the study.
Data Analysis
Statistical Analyses were done using the R package and Statistical Package for Social Scientists (SPSS) version 27.0. Descriptive statistics (frequency and percentage) were performed for categorical data and presented using tables.
The level of knowledge was assessed based on the responses regarding etiology, nutrition, risk assessment, classification, and prevention of pressure injuries questions. A score of 1 was assigned for a correct response while 0 was assigned for an incorrect response. With attitude, a score of 1 was assigned for strongly disagree, 2 for disagree, 3 for agree, and 4 for strongly agree. The barriers section was scored as Yes or No. The final knowledge scores were categorized into two; thus, good (if a nurse answers correctly 75% or more of the knowledge questions on PI prevention) and poor (if a nurse answers correctly less than 75% of the knowledge questions on PI prevention). Similarly, the final attitude scores were grouped as good and poor if the nurse scored 75% or more and less than 75% respectively. These categorizations are consistent with previous similar studies (Berihu et al., 2020; Fulbrook et al., 2019; Sham et al., 2020). Bivariate analysis was done to ascertain factors that were associated with the knowledge and attitude of nurses, using the chi-square test. Multivariable logistics and complementary log-log regression modeling methods were used to predict the knowledge level of nurses. In modeling dichotomous outcome variables, when either the presence of the event or the absence of the event is rare, complementary log–log regression modeling becomes handy. In this study, 79% of the nurses had good knowledge toward PI prevention, hence, a complementary log-log regression model was compared with a logistic regression model. Confidence intervals were computed at a 95% confidence level and a p-value less than or equal to 0.05 was considered statistically significant.
Results
Out of a total of 231 nurses who were given questionnaires, 216 answered and submitted their questionnaires. Females formed the most (56.5%) while 63.9% were aged 25 to 31 years. Most, 47.2% had diploma qualifications and about two-thirds, 70.8% were registered general nurses. The majority (79.2%) of the nurses had received education on pressure injury prevention and 66.2% read literature on pressure injury prevention. Table 1 illustrates the socio-demographic characteristics of respondents.
Socio-Demographic Characteristics of Respondents.

Source: Field data.
Knowledge of Nurses on Pressure Injury Prevention
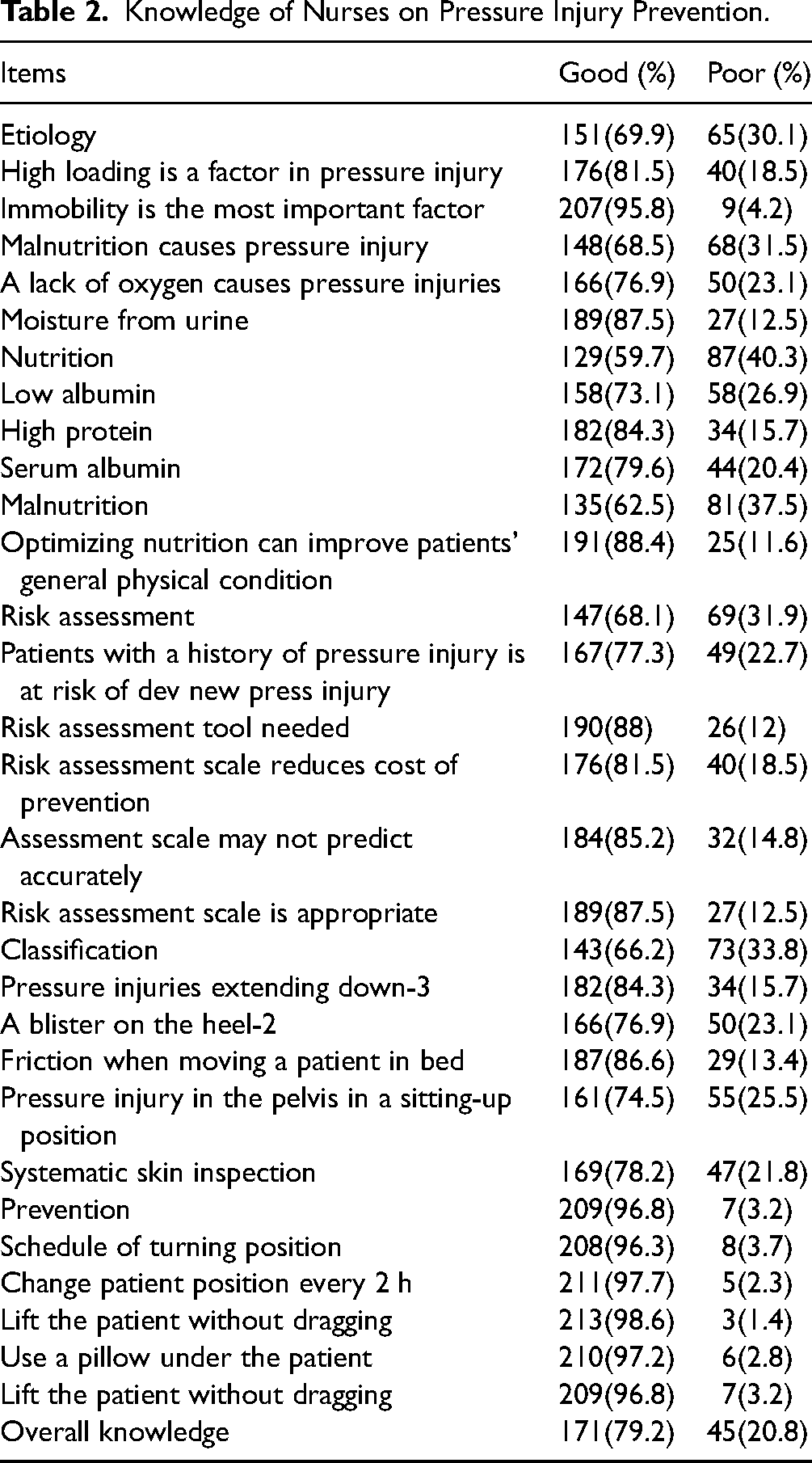
Table 2 presents findings on nurses’ knowledge of pressure injury prevention. The nurses demonstrated high knowledge scores in the prevention sub-scale 209(96.8%) followed by the etiology sub-scale 151(69.9%) while the lowest knowledge score was observed in nutrition (59.7%).
Knowledge of Nurses on Pressure Injury Prevention.
Summary of Nurses’ Overall Knowledge Score
From the analysis, the majority (79%) of the nurses scored more than 75% correct responses on knowledge questions and have been classified as having good knowledge compared to 21% who scored at most 75% of the correct responses. Additionally, the registered nurses’ category was more knowledgeable in preventing pressure injuries (81.7%) compared to 73% for the registered nurse assistant clinical.
Factors Associated With Nurses’ Knowledge of Pressure Injury Prevention
In the bivariate analysis, nurses who worked at their current ward for one to two years [cOR = 2.616 (95%CI: 1.05, 6.496), p = .034], nurses who had overall work experience of 2 to 4 years [cOR = 2.596 (95%CI: 1.117, 6.03), p = .024], nurses who worked in a teaching hospital [cOR = 3.281 (95%CI: 1.504, 7.16), p = .002], and nurses who have received education on PI prevention [cOR = 2.702 (CI: 1.30, 5.603), p = .006] were more likely to prevent pressure injuries while nurse who never had any source of education on pressure injury prevention [cOR = .286 (CI: .119, .684), p = .004], were less likely to prevent pressure injuries. The logistic regression model (LRM) and complementary log–log regression model (CLLRM) were compared in fitting the data. LRM (p-value = .174) and CLLRM (p-value = .056) were correctly fitted with Hosmer and Lemeshow tests. Nagelkerke and Cox and Snell pseudo-R-squared values for CLLRM were 0.19 and 0.12, respectively. LRM also respectively reported 0.17 and 0.11. The CLLRM model also reported lower AIC, AICc, and BIC values of 208.5, 210.4 and 251.9 than LRM (211.7, 213.6 and 255.0), respectively. The metrics reported by the complementary log-log regression model outperformed the Logistic regression model hence its results were explained.
However, after controlling for covariates, multivariable complementary log-log regression analysis revealed that nurses who worked in a tertiary facility (Hospital A) [aRR = 2.09 (95%CI: 1.31, 3.44), p = .002] were 2 times more likely to prevent PI compared to those who worked in the primary (Hospital C) and secondary level facilities. Additionally, nurses who had 2–4 years of work experience [aRR = 1.96 (95%CI: 1.23, 3.22), p = .004] were more likely to prevent pressure injuries compared to those who had less than two years of work experience. Those who never had education on pressure injury [aRR = 0.48(95%CI: 0.23, 0.98), p = .041] were less likely to prevent pressure injuries compared to those who had education on pressure injury at their workplace. The bivariate and multivariate analyses are shown in Table 3.
Predictors Analysis of the Factors Associated With Nurses’ Knowledge of Pressure Injury Prevention.
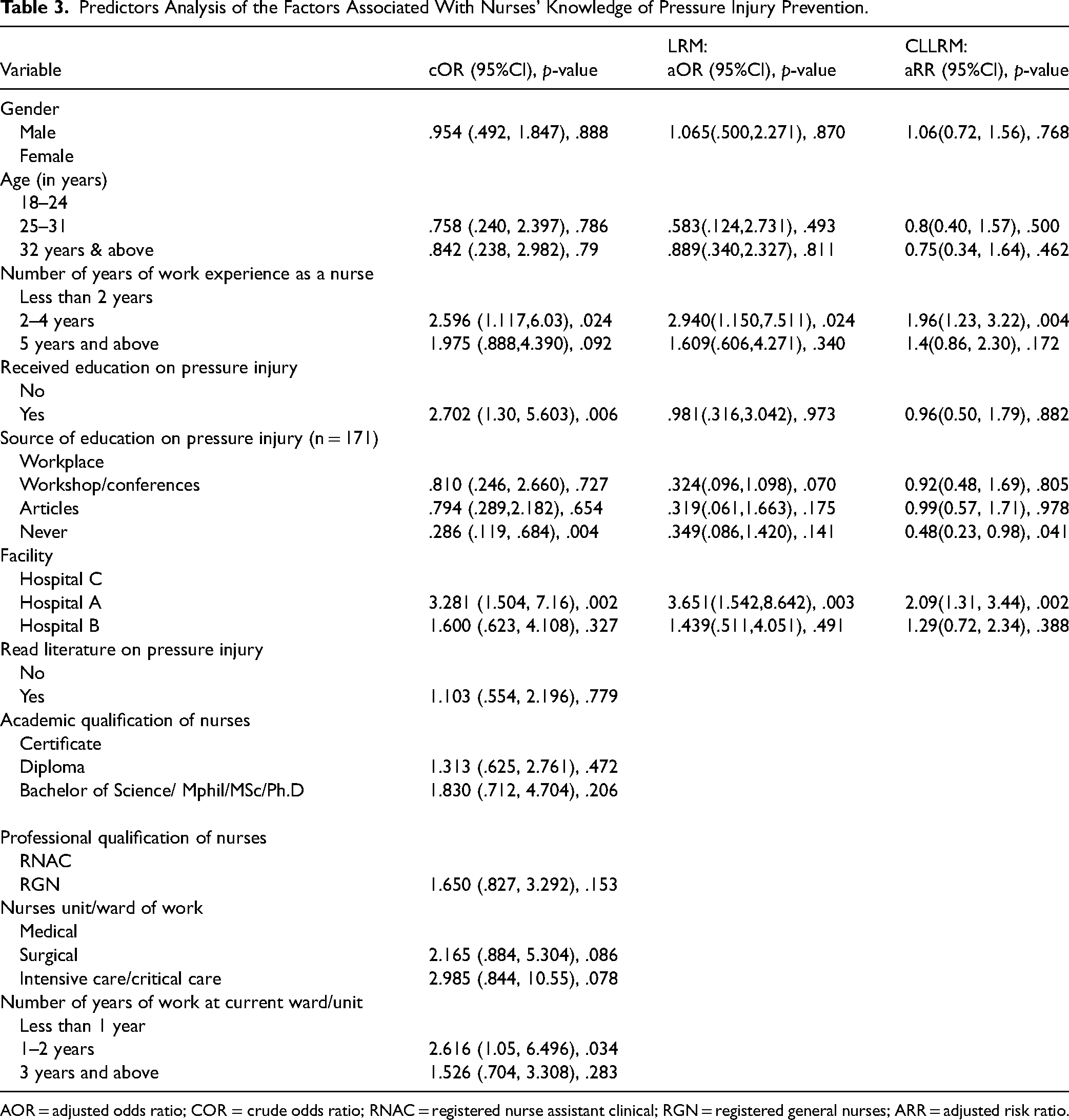
AOR = adjusted odds ratio; COR = crude odds ratio; RNAC = registered nurse assistant clinical; RGN = registered general nurses; ARR = adjusted risk ratio.
Attitudes of Nurses Toward Pressure Injury Prevention
Summary of Nurses’ Attitude Toward Pressure Injury Prevention
About 94% of the nurses showed poor attitude while only 6% demonstrated a good attitude toward PI prevention.
Attitude of Nurses on Pressure Injury Prevention
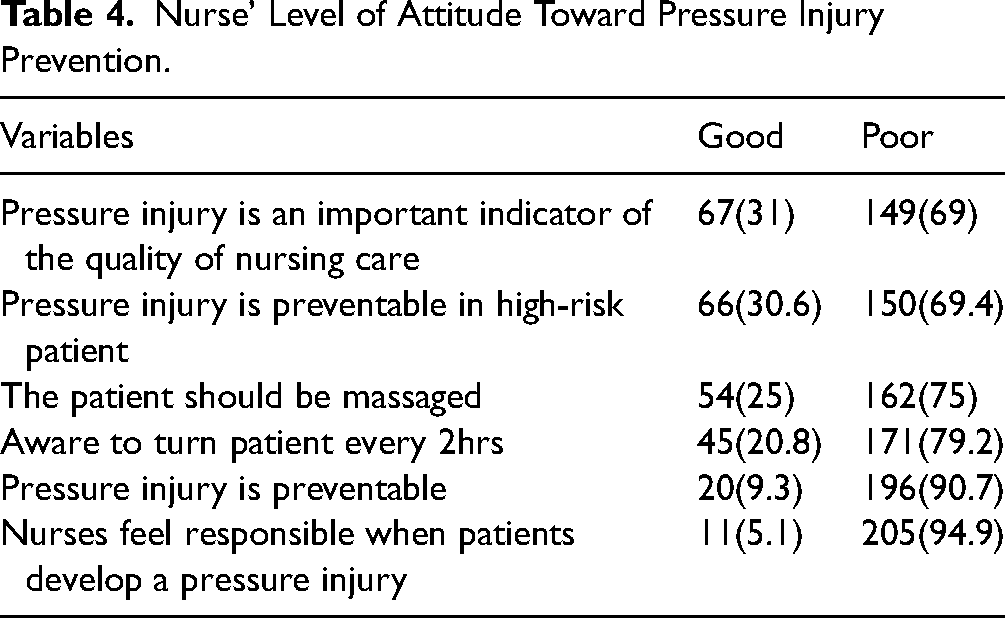
In Table 4, less than 50% had a good attitude toward PI regarding individual items. Pressure injury is an important indicator of quality of nursing care (31%), and PI is preventable in high-risk patients (30.6%) were the highest scored items under good knowledge. In contrast, 94.9% indicated nurses are not responsible for PI while 90.7% responded that pressure injuries are not preventable.
Nurse’ Level of Attitude Toward Pressure Injury Prevention.
Factors Associated With Nurses’ Attitude Toward the Prevention of Pressure Injury
In the bivariate analysis, the place of work was associated with nurses’ attitudes toward pressure injury prevention. Nurses at Hospital B [cOR = 4.2(1.048, 16.83), p = .032] were more likely to have a positive attitude toward preventing pressure injuries than those at Hospital C. See Table 5.
Factors Associated With Nurses’ Attitude Toward Pressure Injury Prevention.

COR = crude odds ratio; RNAC = registered nurse assistant clinical; RGN = registered general nurses.
Perceived Barriers to the Prevention of Pressure Injury
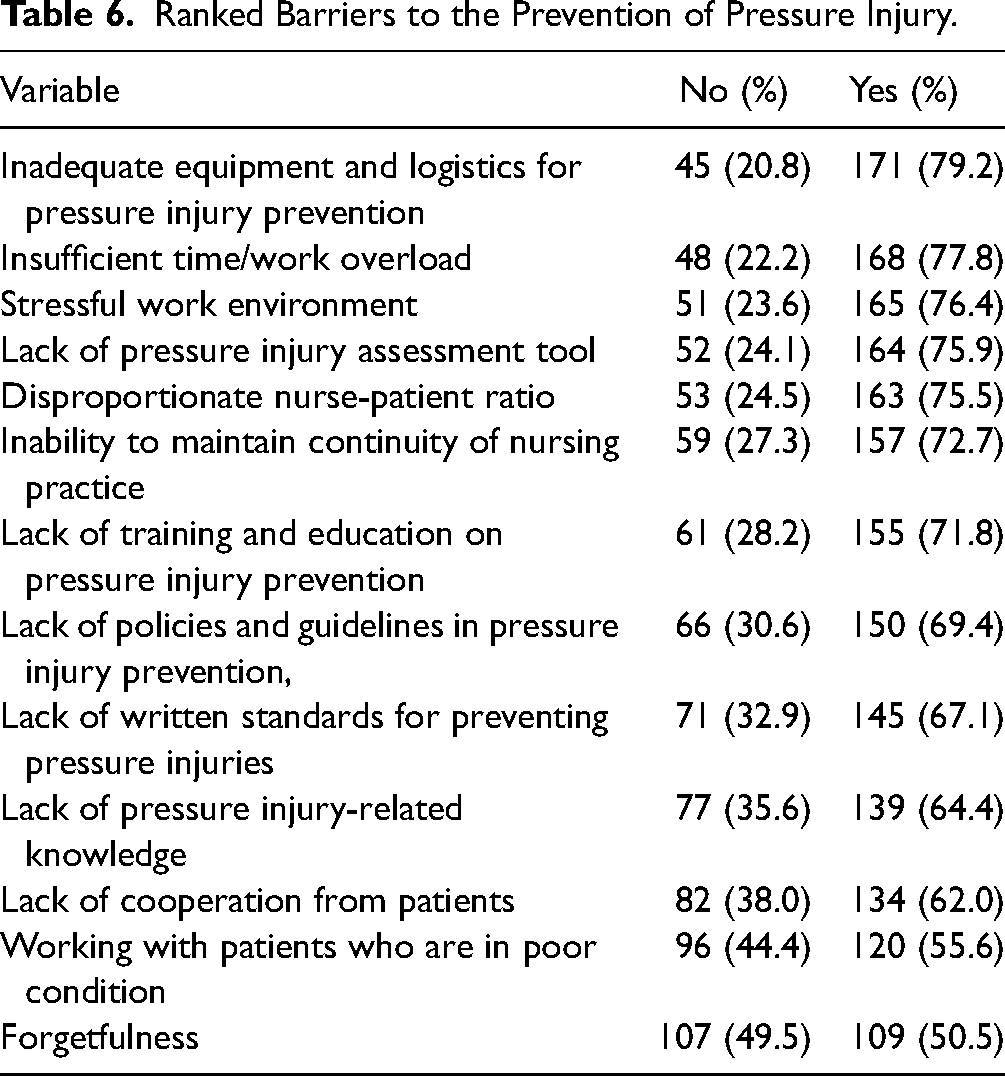
Table 6 presents the barriers to the prevention of pressure injuries indicated by the nurses. The five most dominant barriers in this study were inadequate equipment and logistics for pressure injury prevention (79.2%), insufficient time or increased work overload (77.8%), stressful work environment (76.4%), lack of pressure injury assessment tool (75.9%), and disproportionate nurse-patient ratio (75.5%).
Ranked Barriers to the Prevention of Pressure Injury.
Discussions
Issues of pressure injury border on quality of care by health professionals which affects the quality of life of patients. Greater awareness and positive attitudes toward pressure injury prevention are essential in ensuring the quality of care for patients. It is also an act of ensuring professional integrity and competence and measuring quality improvements in patient care. Therefore, the current study examined nurses’ knowledge, attitudes, and perceived barriers toward pressure injury prevention.
The current findings showed that nurses’ knowledge score on pressure injury prevention was 79%, which signifies that nurses were knowledgeable in preventing pressure injuries. Similar studies in Malaysia, Ethiopia, and Namibia corroborate our findings (Abrahams et al., 2023; Berihu et al., 2020; Sham et al., 2020). Contrary, a plethora of previous studies have reported low nurses’ knowledge using similar questionnaires and knowledge cutoff points (Bjurbo et al., 2024; Coventry et al., 2024; Gedamu et al., 2021; Ingwu et al., 2019; Sawant & Shinde, 2017). The overall knowledge score is not surprising as the majority of nurses revealed that they received education on PI prevention in the current study. Education could have improved their understanding of how pressure injuries are developed and prevented. Inadequate knowledge may lead to poor quality of care, which eventually catalyzes poor quality of patient's life, prolonged hospital stay, and promoting pain or discomfort in the patient (Nguyen et al., 2015; Nuru et al., 2015).
Consistent with similar studies globally, the current study examined knowledge on five (5) sub-scales; etiology and development of pressure injuries, Nutrition, Risk assessment, Classification, and prevention (Ebi et al., 2019; Kim & Lee, 2019; Parisod et al., 2022). Nurses were more knowledgeable in the prevention sub-scale. This finding agrees with a study in Australia that used the Pieper-Zulkowski Pressure Ulcer Knowledge Test (PZPUKT) questionnaire to assess nurses’ knowledge of PI prevention (Fulbrook et al., 2019). In the prevention sub-scale, three responses emerged with the highest scores; lifting patients without dragging, changing patients’ position by turning every 2 h, and placing pillows under patients’ legs. These findings corroborate previous findings (Aydın et al., 2019; Nuru et al., 2015; Saleh et al., 2019). Contrary to our findings, nurses in Sweden, Nigeria, and Ethiopia neither repositioned patients, lifted patients without dragging nor knew the importance of placing pillows under patients heals respectively to prevent PI (Ingwu et al., 2019; Nuru et al., 2015; Schoeps et al., 2017). It is instructive to also state that the majority of nurses were able to correctly identify the causes or risk factors of PI development. They mentioned immobility of patients, malnutrition, lack of oxygen, and moisture from feces and urine which corroborates similar previous findings (Berihu et al., 2020; Ingwu et al., 2019). One of the nurses’ major responsibilities in maintaining skin integrity is identifying and preventing the factors that break the skin. When nurses possess the knowledge to identify risk factors, they can develop and institute strategic measures ranging from daily skin assessment to educating patients on how to identify and prevent PI effectively from occurring. Despite demonstrating overall good knowledge of PI prevention, our findings still highlight the need for further reinforcement in PI education among nursing staff (Parisod et al., 2022) especially, in the areas of risk assessment, observation, and classification (Carvalho et al., 2019; Parisod et al., 2022). In accordance with previous empirical evidence (Parisod et al., 2022), our findings affirm the need for further measures to enhance the knowledge of nurse assistants due to their poor knowledge of PI prevention compared to the registered nurses.
Nurses who worked in a teaching hospital were more likely to demonstrate good knowledge compared to those who worked in secondary and primary-level facilities. The study by (Liang et al., 2024) affirmed our findings where they found that nurses in secondary-level facilities and below were less likely to demonstrate good knowledge compared to those in tertiary facilities. The teaching hospitals in Ghana are classified under tertiary referral facilities as per the Ghana Health Service pyramidal healthcare and referral system levels. They have the autonomy to recommend and recruit highly qualified nurses through thorough recruitment processes. These hospitals create a conducive learning environment that promotes expert mentorship, monitoring and supervision, interprofessional collaboration, research opportunities, and feedback. Importantly, these hospitals have advanced medical technology, and well-stocked medical libraries, and encourage evidence-based clinical practice. Staff are exposed to frequent continuing professional development opportunities through workshops and seminars that keep them abreast with best clinical practice. The nurses who work in these facilities often possess higher educational qualifications such as a bachelor's, master's degree, or specialized nursing training which may have improved their knowledge
Despite the nurses’ good knowledge in this study, their attitude was poor. Contrary to our finding, the majority of studies revealed that nurses demonstrated a more positive attitude than a good knowledge of pressure injury prevention (Bjurbo et al., 2024; Liang et al., 2024; Sari et al., 2021; N. Song et al., 2024). This discrepancy in our study may stem from factors such as increased workload, poor staffing, and lack of resources as corroborated by previous studies (Barakat-Johnson et al., 2018; Coventry et al., 2024; Etafa et al., 2018) and may have hindered the nurses’ attitudes despite good knowledge. Also, a perceived lack of support such as training and making available resources to work with and institutional motivation or rewards for pressure injury management may dampen the spirits of nurses, leading to a poor attitude toward PI prevention (B. Song et al., 2024). The above factors need to be addressed by healthcare institutions as facilitators toward improving nurses’ attitudes. Nonetheless, a positive nurse's attitude is critical in the implementation of care strategies, especially in the areas of skincare, to identify, prevent, and treat pressure injuries (Abrahams et al., 2023; Bjurbo et al., 2024; Coventry et al., 2024; Liang et al., 2024). Chances that a positive attitude may influence a person's behavior toward a particular situation such as pressure injury prevention are high (Beeckman et al., 2011; Fishbein & Ajzen, 1975), however, a poor attitude score is a cause for concern.
In this study, most nurses identified organizational or institutional factors as the most perceived barriers to preventing PI, such as inadequate equipment and logistics for pressure injury prevention, insufficient time/work overload, and stressful work environment. The current finding is congruent with previous findings (Batiha, 2018; Hamdan et al., 2018; Sham et al., 2020). Insufficient time, increased workload, and stressful environment may be due to low or inadequate staffing (Coventry et al., 2024; Ebi et al., 2019). Increased workload may leave nurses with fewer opportunities to perform effective nursing care, which inhibits proper patient assessment to identify at-risk patients (Barakat-Johnson et al., 2018). A shortage of nursing staff may also prevent key nursing interventions such as lifting patients without dragging and repositioning (Coventry et al., 2024; Kim & Lee, 2019). If the problem of staff shortage continues and leaves the burden of nursing care on a few it will not be surprising to realize that most nurses will become less interested in preventing PI and turn their attention to patients who are not critically ill. Notwithstanding the above, the nurses also mentioned the lack of pressure injury assessment tools at health facilities as a barrier. Perhaps, the N&MC of Ghana needs to look beyond providing checklists for treating PI in health facilities but should also develop a comprehensive guide that will include risk assessment, staging of PI, and classification, to aid in effective clinical practice.
Limitation and Strength
To the authors’ best knowledge, this is one of the few studies conducted in Ghana and the first in the northern part of the country regarding knowledge, attitude, and perceived barriers of nurses toward pressure injury prevention. However, the study presented some limitations that need to be mentioned. Firstly, the responses provided by the nurses are self-reported, which may come with some biases, and secondly, the responses provided by the nurses may not reflect how they provide care for patients. Notwithstanding the above, the authors believe the results of the study provide the basis for providing quality nursing care to patients and the results can be generalized since this was a multi-center facility study.
Conclusion and Recommendations
The findings from this study reveal some crucial insights into the challenges and opportunities for improving pressure injury prevention in Ghana among nurses. Despite the high knowledge level among nurses, the poor attitude level calls for a critical need for interventions focused on behavioral change and attitude improvements. Furthermore, barriers such as inadequate equipment and logistics for pressure injury prevention, insufficient time/work overload, and stressful work environment accentuate systemic challenges that impede optimal nursing care. The barriers highlight the need for holistic strategies that encompass resource allocation, workload management, and the need for a supportive and less stressful working environment.
Based on the findings, the following recommendations are timely; firstly, policy reforms and the design of training programs tailored toward encouraging attitudinal change and improving knowledge and skills are crucial, especially for lower cadres of nurses (B. Song et al., 2024). Also, continuing professional development and support systems that translate knowledge into practice is opportune (Dalvand et al., 2018). Furthermore, the Nursing and Midwifery Council of Ghana together with managers of healthcare facilities should develop and implement a comprehensive pressure injury prevention document for use in healthcare settings and for the training of nurses (Liang et al., 2024). Lastly, health facilities should enforce PI prevention by ensuring nurses identify at-risk patients leading to prevention during the delivery of care daily.
Implications for Practice
The findings indicate that nurses demonstrated good knowledge but demonstrated a poor attitude toward preventing pressure injuries. Continuing professional development through organizing regular training sessions, workshops, and motivational programs to drive proactive care and foster a positive attitude is timely. The findings will inform policy direction on the training of nurses in Ghana. Training programs should be comprehensive, and should intentionally include aspects of attitude change, managing stress and, efficient work practices. Lastly, collaborative efforts of healthcare policymakers, including facility heads, ward managers, and administrators are timely to develop and implement policies that address issues of pressure injury prevention comprehensively, leading to improved quality of care and ultimately improved patient outcomes.
Footnotes
Acknowledgment
The authors express their profound gratitude to the nurses for taking time out of their usual busy schedules to take part in this study. Further gratitude goes to the management of the hospitals for permitting us to conduct the study in their facilities.
Author Contributions
Conceptualization: SMS and II; Data curation: SMS, AA, and DA; Formal analysis: SMS, AA, and DA; Funding acquisition: All authors; Investigations: SMS, AW, GD, II, FAK, SM, IO; Methodology: SMS, AA, AK, FKN, PA, RKA; Project administration: SMS, AA, AK, FKN, GD, PA, RKA; Resources: all authors; Software: SMS, AA, DA, and RKA; Supervision: AK, FKN, PA, and RKA; Validation: AK, FKN, PA, and RKA; Visualization: SMS, AA, DA, and II; Writing-original draft: SMS and II; Writing review and editing: all authors.
Data Availability
The data used for analysis is available on secure and reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical approval was obtained from the University of Health and Allied Sciences Research Ethics Committee (UHAS-REC) with protocol identification number UHAS-REC A.1 [19] 19-20.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Voluntary written informed consent was obtained from all the respondents before the commencement of the study.