
Abstract
Introduction
Nurse–physician collaboration is a fundamental part of the healthcare information flow, while poor or improper collaboration could result in poor healthcare outcomes and increased medical errors.
Objective
This study investigated the relationship between nurse–physician collaboration and the perceived quality of healthcare services offered in Jordanian public hospitals, and associated factors.
Methods
A descriptive correlational research design was used. A sample of 385 nurses employed in five Jordanian public hospitals was recruited. Nurse–Physician Collaboration Scale was used to assess collaboration, while the HEALTHQUAL scale was used to evaluate healthcare service quality. The IBM SPSS software (version 26) was used to analyze the data.
Results
There was a positive correlation between nurse–physician collaboration and the perceived quality of healthcare services provided to patients (r = 0.778, p < .01). There was variability in the perception of nurse–physician collaboration based on gender, RN-to-patient staffing ratios, age, and income level (p < .05). No association was found between nurses’ demographics and their perceptions of the quality of healthcare services provided to patients.
Conclusions
Healthcare organizations should implement effective practices to promote nurse–physician collaboration, which could subsequently improve the quality of tangible services provided to patients.
Introduction
Nurses and physicians play vital roles in the healthcare team, and their collaboration is essential for achieving optimal patient outcomes. Accurate information-passing between nurses and physicians is a critical factor in patient outcomes. Physicians and nurses can treat patients collaboratively, utilizing their skills, knowledge, and expertise. Collaborative care delivered by nurses and physicians is characterized by shared goals, acceptance, and respect for individual strengths and differences, fair, and effective decision making, a clear patient focus, and routine communication (Falana et al., 2016).
One of the essential aspects of providing healthcare services is teamwork, which is vital for ensuring high-quality and safe care. Teamwork is necessary in the current complex healthcare system, which is crucial for critical actions and procedures (Georgiou et al., 2017). Collaboration is the exchange of ideas among individuals around a single topic. Interprofessional collaboration aims to give each team member an equal opportunity to contribute their knowledge and skills in an atmosphere of respect and trust. This collaboration in the healthcare system strives to promote interaction between the various healthcare providers during patient care (Georgiou et al., 2017).
Effective nurse–physician collaboration is essential for delivering high-quality healthcare services to patients. It could also lead to better patient outcomes, including reduced hospital readmissions, lower mortality rates, fewer complications, and decreased rates of adverse events (Boev et al., 2022).
Review of Literature
Teamwork between nurses and physicians goes beyond simply sharing an office space. It suggests a shared objective and responsibility to deliver healthcare that addresses the patient's needs (Sharifiyana et al., 2016). Thus, the literature agrees that the nurse–physician collaboration concept assumes the following three constructs: information sharing, joint decision making, and cooperativeness (Elsous et al., 2017; Kim et al., 2022; Ushiro, 2009). Whether or not an agreement is reached during the interaction, collaboration entails the exchange of thoughts and ideas while considering everyone on the health staff's diverse points of view (Standaert et al., 2021).
Quality of care refers to the likelihood that anticipated health outcomes will materialize due to individual and population health treatments. Although there are many ways to define excellent healthcare, it is becoming widely understood that these elements should be present in high-quality services: providing evidence-based healthcare to those in need, guarding against injury to individuals receiving treatment, and individual-centered care (Ritchie et al., 2018). Healthcare service quality can be better defined in terms of process and outcome measures. The processes refer to what a healthcare provider generally does in clinical practice to maintain or improve health. This dimension could include empathy, tangibles external factors regarding physical facility and equipment, safety and patient protection, and cost efficiency in service delivery processes (Lee, 2017; Lee & Kim, 2017; Yunningsih, 2022). The outcome reflects the impact of the intervention provided by healthcare providers on the health status of patients. This dimension is reflected in the degree of care improvement (Lee, 2017; Lee & Kim, 2017). Positive patient outcomes in healthcare settings are best achieved through effective interprofessional teamwork. Because physicians and nurses have different perspectives on patient care, the distinctions between the two professions might be seen as an asset rather than a liability for patient care (Myers, 2017).
The need for this study originated from the lack of such studies that focused on the effect of nurse–physician collaboration on the quality of the provided healthcare services. Most of the related studies focused on one aspect of healthcare quality or patient outcome and, in some cases, one department or unit in the hospital. Moreover, limited research has been conducted on this topic in the Middle East and Jordan, which argues for the need to perform such studies. The results of this study could be used as a reference for hospital managers and decision makers to improve the quality of healthcare provided in Jordanian public hospitals through improving nurse–physician collaboration. The outcome of this study would open the way for more studies and research to fill in the gap in the literature.
Purpose
With the aim of investigating the link between nurse–physician collaboration and the healthcare services offered in the Jordanian public hospitals, this study was guided by the following research questions:
How do nurses describe nurse–physician collaboration and quality of healthcare services? What is the relationship between nurse–physician collaboration and the perceived quality of healthcare services provided to patients? What is the variability in the perception of nurse–physician collaboration and the perceived quality of healthcare services provided to patients based on nurses’ demographics?
Methods
Research Design
A descriptive correlational research design was used.
Sample
The target population comprises all the working nurses in the Jordanian public hospitals during the research period. On the other hand, the accessible population includes nurses working in the largest five public hospitals in Jordan that are accessible to the researcher. A convenience sample technique was used to recruit nurses. The minimum sample size required is 385 to have a confidence level of 95%, a margin of error of 5%, and a population proportion of 0.5. Besides, the current study conducted a one-way analysis of variance (ANOVA) analysis with nine groups. The minimum required sample size to meet this purpose depends on the G*power program, a power =0.95, with an alpha set at 0.05, a medium effect size; the minimum needed sample size is 378. Therefore, the sample size 385 is reasonably adequate to meet the study purpose.
Inclusion and Exclusion Criteria
The inclusion criteria were (a) nurses employed in their departments for a minimum of 6 months so that they completed their probation period for employment and could share their perspectives regarding collaboration with physicians and (b) primary nurses who attend direct patient care. Those on leave during the study period, nurse educators, and nurse managers were excluded from the study.
Measures
Demographic Questionnaire
The Demographic Questionnaire was used to measure the sociodemographic variables, including gender, age, education, marital status, income, year of experience, hospital unit, and RN-to-patient staffing ratios. These demographics were mainly selected on the basis of references in the literature associating them with the nurse perceptions of collaboration (Al-Ajarmeh et al., 2022; Kang et al., 2020; Mansourimoaied et al., 2000; Migotto et al., 2019).
Nurse–Physician Collaboration Scale
The Nurse–Physician Collaboration Scale was developed by Ushiro (2009). This scale is commonly used instrument to assess collaboration between nurses and physicians from the nurses’ perspective (Kim et al., 2022; Zhang et al., 2016). It consists of three dimensions with 27 items. The first dimension is joint participation in the decision-making process. This dimension includes 12 items, with a Cronbach's α coefficient of 0.923. The second one is sharing patient information. It has nine items with a Cronbach's α coefficient of 0.905. The third one is cooperativeness. It has six items, with a Cronbach's α coefficient of 0.800. A Likert five-point scale was used to classify answers as follows: (1) strongly disagree, (2) disagree, (3) neutral, (4) agree, and (5) strongly agree. The mean scores of all items range from 1 to 5, with a higher mean score indicating greater nurse–physician collaboration. Cronbach's α coefficient for the overall scale was 0.932.
HEALTHQUAL Multi-Item Scale
The HEALTHQUAL multi-item scale (Lee, 2017; Lee & Kim, 2017) was used to assess healthcare service quality. It consists of five dimensions with 33 items: empathy (7 items) with Cronbach's α coefficient of 0.932, tangible (5 items) with Cronbach's α coefficient of 0.807, efficiency (7 items) with Cronbach's α coefficient of 0.823, safety (6 items) with Cronbach's α coefficient of 0.872, and improvements of care service (8 items) with Cronbach's α coefficient of 0.842. The HEALTHQUAL is rated on a Likert-type five-point scale, ranging from 1 = worst to 5 = outstanding, with a higher mean score indicating a better-perceived healthcare service quality. Cronbach's α coefficient for the overall scale was 0.969.
Data Collection
In order to collect the primary data for the research, the primary researcher distributed the questionnaire online. Data were collected from January to March 2022. The researcher met the nurse managers in the hospitals, and the aim of the study was explained to them. The online survey was created with Google Forms. The nurse managers emailed the survey to nurses in the Jordanian public hospitals. The distributed questionnaires were (1000) and (392) were retained with a response rate of (39.2%). After cleaning the data, 385 were included in the analysis.
Ethical Considerations
The approval of the study was granted by the Institutional Review Board (IRB) of The IRB Committee of Zarqa University. Before collecting data, permission was requested from the Jordan Ministry of Health to access the governmental hospitals. The tools’ developers provided permission to use their tools. Participants had the right to privacy, anonymity, and the freedom to withdraw from the study. Consent to participate in the study was obtained using a check box to tick to indicate that the nurse participant agreed to participate. A brief explanation of the study objectives and procedure and the consent form were embedded in the online survey.
Statistical Analysis
After data collection, the researcher used the IBM SPSS software (version 26) to analyze the data. For the descriptive data, arithmetic means and standard deviation were reported. Pearson correlation coefficient analysis was used to assess the relationship between nurse–physician collaboration and the perceived quality of healthcare services provided to patients. Independent t-tests and one-way ANOVA were used to assess differences in the scores of main study variables based on categorical demographics.
Results
Sample Characteristics
Most participants were male (62.9%), single (55.1%), and had a bachelor's (43.1%) or a postgraduate (29.1%) degree. Participants were employed in oncology units (18.4%), pediatric units (16.1%), postcritical care units (15.3%), women and infant health units (12.2%), intensive care units (11.4%), surgical units (9.4%), and other units (17.2%). For the RN-to-patient staffing ratios, the highest category was (1:5) with a percentage of (30.1%), and the lowest ratio was (1:6) with a percentage of (14.8%).
The mean value for the age of the respondents was 37.5 years, while the maximum age recorded was 55 years. For the income level, the mean value was 537.5 JD, and the minimum income level was 360 JD (1 JD = 1.41 USD). Finally, the minimum number of years of experience recorded was 1, and the maximum was 23, with a mean value of 12.08, Table 1.
Distribution of the Study Sample (n = 385).

Nurses’ Perceptions of Nurse–Physician Collaboration and Quality of Healthcare Services
The mean score of the nurse–physician collaboration was 3.57 for the cooperativeness subscale, 3.78 for sharing patient information, and 3.79 for joint participation in the decision-making process. The mean score of the perceived quality of healthcare services provided to patients from nurse perceptions was 3.57 for the efficiency subscale, 3.58 for the improvements of care service subscale, 3.59 for the tangible subscale, 3.69 for the empathy subscale, and 3.72 for the safety subscale.
Variability in the Perception of Nurse–Physician Collaboration and Perceived Quality of Healthcare Services Provided to Patients Based on Nurses’ Demographics
Based on Table 2, there were no statistically significant differences in relation to the study's variables regarding the perceived quality of healthcare services based on the following variables (gender, education level, marital status, hospital unit, and RN-to-patient staffing ratios). Also, there is no correlation between perceived quality of healthcare services and the variables (age, income level, and years of experience).
Factors Affecting Quality of Services and Nurse–Physician Collaboration (n = 385).

* Correlation is significant at the 0.05 level (2-tailed).
** Correlation is significant at the 0.01 level (2-tailed).
Nurse–physician collaboration was significantly higher among female participants and participants who reported a nurse–patient ratio of 1:3 or fewer. There was also a significant correlation between nurse–physician collaboration and age and income level.
Relationship Between Nurse–Physician Collaboration and Perceived Quality of Healthcare Services
Table 3 shows a significant positive relationship between nurse–physician collaboration and the perceived quality of healthcare services provided to patients. The correlation coefficient was 0.778 at the level of significance α ≤ 0.01. The values of the correlation coefficient ranged between 0.473 and 0.778.
Pearson Correlation Coefficients Between Collaboration Between Nursing and Healthcare Providers and the Quality of Services.
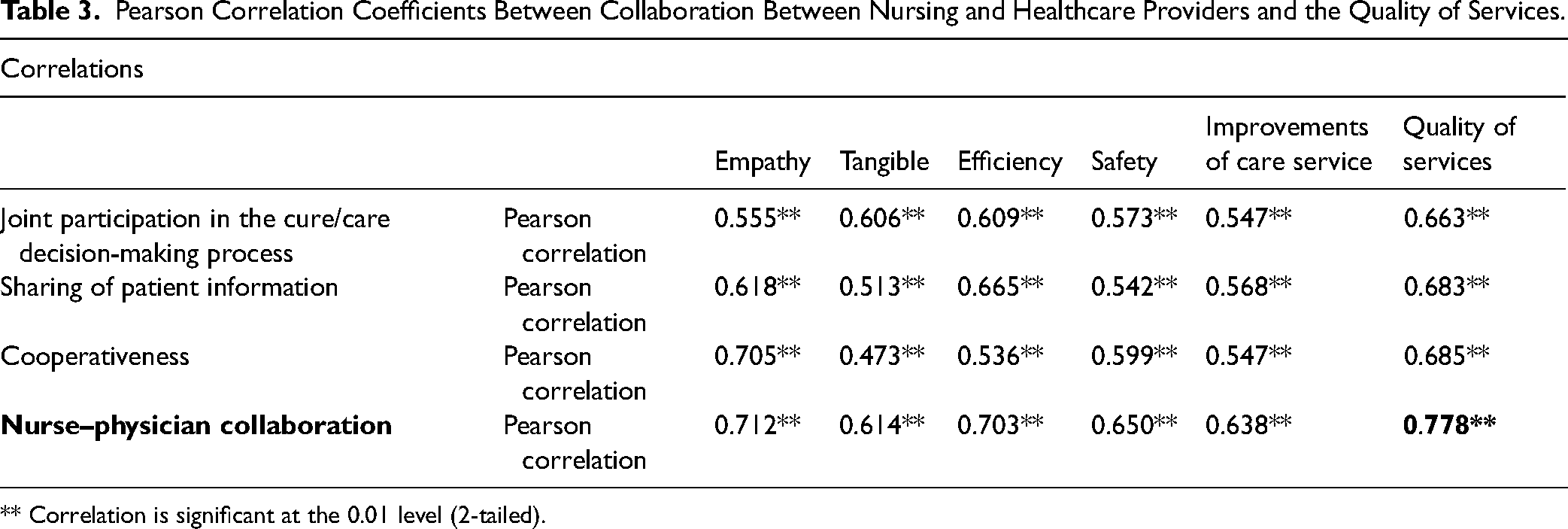
** Correlation is significant at the 0.01 level (2-tailed).
Discussion
This study explores nurse–physician collaboration and the perceived quality of healthcare services from the perspective of nurses. Overall, nurse–physician collaboration scores indicated relatively high levels of collaboration. This collaboration can promote a positive work environment where all healthcare providers feel valued and respected for their contributions (Kim et al., 2022).
The highest-ranked subpart of nurse–physician collaboration was joint participation in the decision-making process, indicating that nurses value their participation with physicians in making decisions related to patient care. Nurses’ joint participation in decision making may include regular meetings with physicians to discuss patient care plans, shared access to patient records, and clear communication channels (Chew et al., 2019). In general, nurses agree they should have an essential role in shared decision making and see their involvement as valuable (Arends et al., 2022). Nurse participants perceived cooperativeness as the lowest among the subdomains of nurse–physician collaboration. Previous research indicates a relatively low level of cooperation between nurses and physicians (Elham & El-Hanafy, 2018; Kim et al., 2022). This finding could be due to the historical–cultural dominance of physicians in the Jordanian healthcare system. Physicians have been in a position of greater power and authority than nurses. This can lead to a hierarchical rather than cooperative relationship where nurses have no choice but to be subordinate to physicians (Almukhaini et al., 2022). Poor cooperation between nurses and physicians is a global problem facing the complex healthcare system. The increasing numbers of female physicians and male nurses in the healthcare team, however, could reduce the dominant–subservient, male–female relationships between nurses and physicians. Previous research has shown that some physicians may have inadequate knowledge of nursing roles and responsibilities, which negatively affects their willingness to cooperate (Elsous et al., 2017). Therefore, more studies are needed to examine various ways to improve cooperation between nurses and physicians, which is essential for delivering safe, high-quality patient care.
In this study, nurses perceive the quality of healthcare services provided to patients positively. Nurses are often on the front lines of patient care, and they can provide valuable insights into what changes are needed to improve the quality of care (Streeton et al., 2016). The highest-ranked subpart of quality of healthcare services was safety. This aspect is crucial for delivering safe, high-quality care, and improving health outcomes. The nurse practice environment predominantly affects patient safety (Abraham et al., 2022). Ensuring patient safety involves a wide range of practices, including establishing well-structured safety protocols and guidelines to minimize the risks associated with patient care. This may include measures such as regular safety assessments, staff training on best practices for patient safety, and using evidence-based practices to reduce the risk of medical errors (Iglesias et al., 2013). The lowest three subscales of quality of healthcare services were empathy, tangible, and efficiency, and their mean scores were very close together. Empathy is essential to ensure patients feel heard and build trust and rapport between nurses and patients (Amudha et al., 2018). Tangible services refer to the physical aspects of patient care, such as the cleanliness and the availability of medical equipment. These aspects are essential for creating a positive patient experience and ensuring patients feel comfortable during their stay (Zubayer & Hoque, 2019). Finally, efficiency is a crucial aspect of healthcare delivery, as it allows healthcare organizations to optimize the use of resources while maintaining the quality of care provided to patients (Al-Hamdan et al., 2021). Overall, the results provide insights into areas for improvement regarding the quality of healthcare services provided to patients, which is essential to enhance the patient experience and improve patient outcomes.
The results showed a strong positive correlation between nurse–physician collaboration and the perceived quality of healthcare services provided to patients. This suggests that high-quality care can be provided to patients when nurses and physicians work collaboratively through teamwork. The positive correlation between nurse–physician collaboration and empathy suggests that nurse–physician collaboration is helpful in understanding and addressing the needs of patients. This can improve patient satisfaction and outcomes (Clancy & Wehbe, 2022). Tangible aspects of care and efficient use of resources are also positively correlated with nurse–physician collaboration. This outcome suggests that when nurses and physicians work together, they are better able to avoid duplication of efforts and waste of resources and ensure that patients have access to valuable resources (Khatoon, 2020; Zubayer & Hoque, 2019). The results also show that patient safety is positively correlated with nurse–physician collaboration. This can lead to fewer medical errors, reduced complications, and better patient outcomes (Wei et al., 2020). Finally, nurse–physician collaboration impacts the outcome of patient care, which is reflected in improvements in care service.
Previous studies have found a strong positive correlation between nurse–physician collaboration and the quality of healthcare services provided to patients (Yaya et al., 2021). In a systematic review by Matthys et al. (2017), nurse–physician collaboration was associated with positive patient outcomes, including hospitalization, patient satisfaction, and blood pressure. A study by Falana et al. (2016) also demonstrated that efficient nurse–physician teamwork is helpful in providing improved healthcare services. Similarly, a study by Kamel and Rashad (2019) showed that nurse–physician collaboration significantly affects the patient safety climate. This indicates the importance of nurse–physician collaboration in providing quality care to patients. Mutual respect and a desire to cooperate have been identified as the basis for successful functional collaboration, regardless of functional, linguistic, and religious differences (Yaya et al., 2021). However, disincentive factors such as pressure to increase productivity and reporting a high administrative workload can hinder collaboration (Kieft et al., 2014).
Female participants reported better nurse–physician collaboration than their male counterparts. Only some studies have discussed the gender issues in nurse–physician collaboration in healthcare settings. Our findings are exciting and consistent with a previous study (Migotto et al., 2019). It seems that nurses’ gender influences perceptions of collaborative practice, with female nurses reporting more positive collaboration experiences with physicians. The differences in reported nurse–physician collaboration between female and male nurses may be attributed to gender-based variations in communication styles, interpersonal skills, and perspectives on teamwork and shared decision making. Interprofessional gender bias in nurse–physician collaboration in healthcare settings could negatively affect job satisfaction, patient care, wellness, burnout, and self-doubt (Manchanda et al., 2021). Therefore, gender should be considered as a potential factor when developing strategies to promote collaboration, and efforts should be made to address gender biases and stereotypes that may be impacting collaboration.
RN-to-patient staffing ratio of 1:3 or fewer was associated with better nurse–physician collaboration. Adequate nurse staffing is critical to ensure safe and effective patient care. Nurse–physician teamwork is an essential component of providing effective and safe patient care. Previous research has shown that lower patient-to-nurse ratios and better nurse–physician collaboration were associated with lower patient mortality rates. Thus, the number of patients per nurse is critical in successful nurse–physician collaboration and in improving patient outcomes (Kang et al., 2020). Understanding the relationship between staffing ratios and nurse–physician collaboration can help healthcare organizations make informed decisions about staffing levels. With fewer patients, nurses may have more time to engage in collaborative activities such as communicating with physicians, sharing information, and coordinating care. Additionally, with lower patient loads, nurses may feel less stressed and have more job satisfaction, which could positively impact their ability to collaborate effectively with physicians.
The Study Limitations
It is important to interpret our study's results in light of the following limitations. First, our study relied on self-reported data from nurses, which could introduce bias or inaccuracies. Additionally, we did not include the perspective of physicians in our examination of collaboration. Second, our study focused on the correlation between nurse–physician collaboration and the perceived quality of healthcare services, without delving into the potential mechanisms or processes that underlie this relationship. Third, our study used a cross-sectional design. Future research could address these limitations by using longitudinal designs to establish causality, incorporating objective quality-of-care measures, and using a larger, more diverse sample to increase generalizability.
Implications
The current study has essential implications for nursing education, practice, and research. Introducing topics related to nurse–physician collaboration in the educational curricula for nursing and medicine students is recommended. Top management should implement effective practices for greater nurse–physician collaboration. This can be done through team-building activities, communication training, and regular meetings to discuss patient care. Creating an inclusive and supportive culture that promotes nurse–physician collaboration should be prioritized, regardless of their gender. Proper staffing ratio should be considered to promote better nurse–physician collaboration. Future studies could conduct an in-depth exploration of the gender differences found in this study and how this issue can be addressed to promote more equitable collaboration. Future studies could also investigate other factors impacting nurse–physician collaboration, such as organizational culture, leadership styles, and job satisfaction. Finally, healthcare organizations should invest in promoting effective practices that foster collaboration. This can lead to a better patient experience, better patient outcomes, and an overall enhancement of the quality of healthcare services.
Conclusion
The current study is one of the unique studies that connect nurse–physician collaboration with the perceived quality of healthcare services from the perspective of nurses. Nurse–physician collaboration is essential to provide high-quality patient care; when nurses and physicians work collaboratively, quality improvement can be achieved in both the process and outcome of care. Nurses generally perceived nurse–physician collaboration and the quality of healthcare services as positive. However, there is still room for improvement in promoting cooperativeness, tangible services, continuous improvement, and efficiency. Nurse gender and nurse–patient ratios have significant effects on nurse–physician collaboration. Nurse–physician collaboration is not created alone, and top management needs to cultivate it by establishing policies and procedures that create an inclusive and supportive culture that promotes collaboration.
Footnotes
Authors’ Contributions
MFA-B was involved in conceptualization, methodology, formal analysis, investigation, and writing—original draft preparation; AHR in conceptualization, methodology, formal analysis, investigation, and writing—review & editing; NFE, MHB, NR, DR, and MSA in conceptualization, methodology, and writing—review & editing; and RM in conceptualization and writing—review & editing.
Availability of Data and Materials
Data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The IRB Committee of Zarqa University approved this study in January, 2022. All participants signed the consent form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Study Approval Number
(6/2022).