
Abstract
Introduction
In all countries, the burden of mental disorders (MDs) spans the entire life course. Smartphones are currently widely used by families with a history of MD looking for the required mental health information. The use of digital media is an alternative to improving the ability of families to care for person with MD at home.
Objectives
This study aimed to explore the opportunity and the benefits of e-coaching as a method and media for empowering families of MD person.
Methods
This study was a qualitative study that recruited 21 participants. The mean age was 45.7 years old, male 42.9%, and female 47.1%. They were divided into four groups: families who have a family member with MD, nurses who provide mental health services, mental health cadres, and government elements in Pekalongan, Central Java, Indonesia. An in-depth interview was applied to collect data. Further, the data were analyzed using thematic content analysis using Colaizzi's frame.
Results
There were four themes related to the possibility of using e-coaching to empower families with a family member with MD: menus, needs, supporting factors, and hindering factors. The use of information technology can be used to improve the ability to take care of families, especially in treating MDs at home with the e-coaching application.
Conclusions
The findings show that developing e-coaching as a method and media is beneficial for person, families, and healthcare providers. In an effort to increase families’ capacity to treat MD at home, the findings of this study might be used to create an easy-to-use smartphone e-coaching application.
Recommendation
It is essential to establish e-coaching through a smartphone-based application in the Indonesian context. Additionally, to better treat MD person, nurses who provide mental health care should consider utilizing the mobile application.
Background
Health is a state of complete physical, mental, and social well-being and is not just the absence of illness or infirmity. Mental disorders accounted for 5.1% of the global burden (WHO, 2022). In all countries, the burden of MD spans the entire life course: from early life, where conditions such as development MDs and childhood behavioral disorders are the most significant contributors to the burden, through to adulthood and old age, where depressive and anxiety disorders dominate (WHO, 2022)
In the context of research conducted in Indonesia, it has been reported that the prevalence of households with members experiencing mental disorders is 4.0 per million. This indicates that out of every 1,000 households, there are four households where at least one member suffers from a mental disorder, specifically psychosis. Given that Indonesia's population in 2023 is approximately 278 million, this statistic translates to an estimated 1,112,000 households affected by mental disorders (Ministry of Health of the Republic of Indonesia, 2023)
The government has provided specific laws to support people with MDs. The law states that mental health efforts in Indonesia are activities to create an optimal degree of mental health for every individual, family, and community. The activities include promotive, preventive, curative, and rehabilitative approaches that are carried out in a comprehensive, integrated, and sustainable manner by the government, local government, and/or the community (State Secretariat of the Republic of Indonesia, 2023)
While many individuals demonstrate resilience, those exposed to adverse circumstances such as poverty, violence, disability, and inequality face elevated risks. Factors contributing to resilience or susceptibility encompass individual psychological and biological traits, including emotional skills and genetic predispositions (WHO, 2022).
Healthcare systems have yet to adequately address the needs of individuals with mental health disorders, facing significant resource deficits. There exists a considerable gap between the demand for treatment and its provision globally, with services often being of poor quality when available. Moreover, individuals with mental disorders require substantial social support, including assistance in establishing and nurturing personal, familial, and social connections. Additionally, they may benefit from support in accessing educational programs, employment opportunities, suitable housing, and engagement in meaningful activities (WHO, 2022).
Research indicates that perceived social support plays a moderating role in the relationship between common mental disorders and active coping strategies (Luce et al., 2022). Given the mediating influence of social support on mental well-being, interventions aimed at enhancing social support networks and reducing stigmatization should be developed to promote mental health. These interventions should be implemented at both the familial and community levels to effectively address mental health concerns (Zhao et al., 2024). Additionally, a social trust may improve the perception of social support from family and friends and may lessen the intensity of traumatic experiences, two independent functions that reduce the chance of mental health issues (Duren & Yalçın, 2021). Professionals assert that an integrated family approach to mental health care is beneficial for families because it addresses the many roles, positions, and connections, implements a flexible complementary treatment plan, and empowers professionals through multidisciplinary consultations (Stolper et al., 2022). A study stated perceived social support moderates the relationship between common mental disorders and active coping (Luce et al., 2022).
An integrated family approach to mental health care includes a multidisciplinary approach to treating the family as a whole since a family of mental illness person who become caregivers for person tends to have higher anxiety. In discussing family structure and dynamics concerning mental illness, family nursing dialogues provide opportunities for families to discover fresh interpretations and potentialities in their daily lives. Healthcare practitioners hold a significant responsibility in fostering a secure atmosphere where young adults and their families can engage in open discussions about their encounters with and handling of mental health conditions (Aass et al., 2020)
An integrated family approach to mental health care benefits families by addressing the many responsibilities, positions, and connections, implementing a flexible complementary treatment plan, and empowering professionals through multidisciplinary consultations (Stolper et al., 2022). However, families with MD person, especially those living in Indonesia, have some hindering factors in running their role to become a caregiver to person. Lack of knowledge and the limit of accessed information become a problem when running their role as caregivers. Affordable and flexible coaching is essential for them to, for example, use smartphones.
Review of Literature
Online and mobile technologies may be leveraged to expand the reach of evidence-based health and mental health promotion programs to individuals in these non-clinical mental health settings. According to the National Survey of Social and Economic data in Indonesia, mobile phone ownership has risen from 59.59% in 2017 to 65.87% in 2021. As mobile phone ownership rises, so does the population's use of mobile phones, rising from 68.59% in 2017 to 81.28% in 2021 (Sutarsih et al., 2021). Digitally enhanced health interventions were robust at providing high-quality assistance and support to caregivers by improving caregiver psychological health, self-efficacy, caregiving skills, quality of life, social support, and problem-coping abilities (Sun et al., 2021).
To our knowledge, which tested the use of Motivational Interviewing (MI) in digital coaching = protocols for the first time, showed the importance of MI expertise in digital health coaching for increased engagement and health improvement. For effective involvement and to maximize = favorable behavioral results, coaching models in digital Cognitive Behavior Interventions that incorporate MI must be developed (Serio et al., 2022).
At present, family empowerment activities remain traditional, predominantly conducted by health workers and local cadres through face-to-face interactions. A novel strategy in implementing evidence-based preventive interventions is termed “family coaching.” This approach holds promise due to three recent advancements in health promotion (D’Avolio et al., 2023). Several programs that support efforts to prevent the recurrence of mental disorders are carried out using various strategies, one of which is empowering people with mental disorders and psychosocial disabilities, for example: peer group, community-based intervention, social support, training, promotion, and coaching (Bashir et al., 2020; Carleton et al., 2023; Roberts et al., 2022; Saleem et al., 2021). However, the shift in mental health services from conventional to digital applications may result in increased social isolation for those who require human interaction, that research that focuses on using technology to support everyone in mental health prevention and intervention is feasible greater attention in the coming decades (Rudd & Beidas, 2020). Currently, the use of technology for coaching in various cases, especially in mental health, is showing a positive impact (Allemand & Flückiger, 2022; Olaru et al., 2022; Zahed et al., 2023). Previous studies have reported the use of coaching in a variety of cases, but coaching for an MD person is a new approach.
This study aimed to explore e-coaching opportunities to improve the family's ability to care for MD person.
Methods
Study Design
This study was a qualitative study with a phenomenological approach. The choice of using qualitative methods is that the research objective is to understand how a community or individuals perceive certain issues. Researchers conducted in-depth interviews to explore participants’ experiences providing care with MDs at home. This study followed TOEH + P framework developed by Cristianto for grouping the participants with 12 items of the consolidated criteria for reporting qualitative research checklist (Christianto, 2020). The TOEH + P framework encompasses several critical aspects: Technology, which considers the advantages, field suitability, and safety of the technology when implemented; Organization, which evaluates the available infrastructure such as health services, management support at Community Health Centers and Health Services, and the availability of health services, particularly those catering to mental disorders; and Environment, which examines the local socio-cultural conditions. The questions have been through expert review and tested first on a small group of participants to avoid possible problems and ambiguity in the questions given.
In-depth interviews were conducted with participants following a structured interview guide, each lasting approximately 45–60 min. The interviews were conducted in Bahasa Indonesia and recorded using a digital recorder in a private room to ensure confidentiality. The transcripts were subsequently translated into English. Anonymity was maintained by excluding names from the recordings, and the data was securely stored on the researcher's private computer, to be used solely for academic purposes. The interviews continued until data saturation was reached, which occurred when no new information or themes emerged from the interviews). Data saturation was achieved with 8 participants from families with individuals suffering from severe mental disorders, 8 health workers including mental health program nurses at Community Health Centers, Heads of Community Health Centers, mental health specialists, and 3 district government staff from Pekalongan, including the Head of Bappeda and coordinators, Head of Non-Communicable Diseases (NCDs), mental health program managers, and 2 community health cadres.
The question items are shown in Table 1.
The Questions of the In-Depth Interview for Each Participant Group.
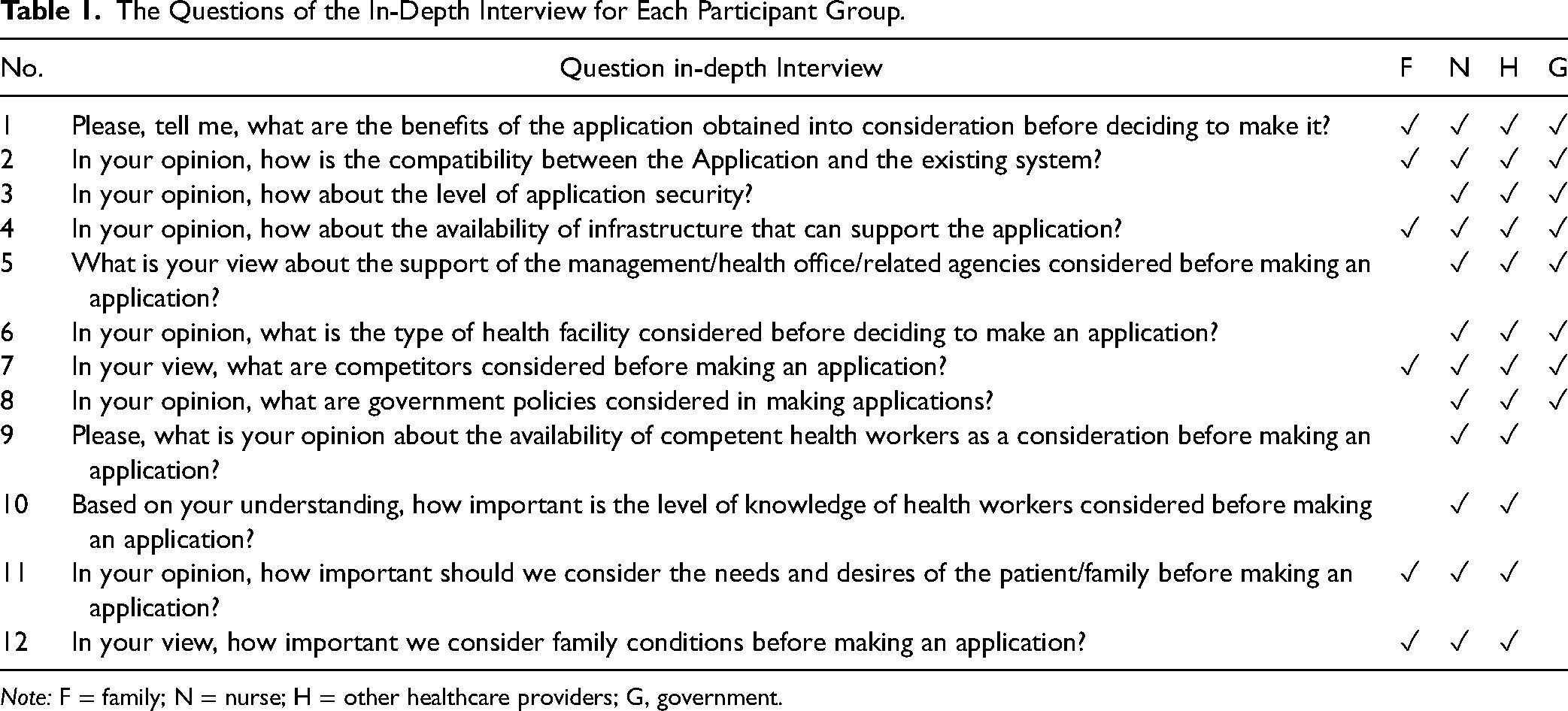
Note: F = family; N = nurse; H = other healthcare providers; G, government.
Research Question
E-coaching enables a unified engagement strategy and personalized feedback on intervention content or users’ mental health status. Individualized support during the intervention, access to social support, and tailored feedback tend to support participation in digital interventions for mental health promotion. Using this information, a study was conducted to assess how feasible e-coaching is to empower the family of person with MD. So the research question is “What are the prospects for e-coaching applications in empowering families?”.
Participant
The researcher conducted interviews with 21 selected participants representing various roles. These participants included families (9 person) and health workers at community health centers (specifically mental health nurses (4 person), heads of community health centers (2), and mental health specialists (1 person), district government staff (3 person), and cadres/caregivers (2 person). The period for data collection was between September 2021 to December 2021. We used purposive sampling to reach the participants. This sampling strategy was chosen to ensure that we obtained individuals who served our purposes and met the requirements. For a family with MDs, persons were taken from six different community health services in six different areas in Pekalongan Regency. To reach the expected participants, the researcher initially contacted the gatekeeper, the mental health service program coordinator in Pekalongan Regency under the Department of Health. He assisted in the recruitment process and subsequently provided a list of potential participants for each category. Following this stage, the researcher made an appointment with the potential participants to do the Interview. Based on a discussion with the potential participants, considering the effectiveness, efficiency, and privacy, the interview venue for families, was at their homes, while goverment, mental health nurse, cadre, and officers of the department of health (3 person) were in their own office. The Interview was individual since the distance was far between one participant and others.
Inclusion and Exclusion Criteria
The participants should meet inclusion and exclusion criteria. Details of participants are described in Table 2. The inclusion criteria for families with MDs were: families with members with mental disorders; physically and mentally healthy; 18 years of age or older; and willing to be participants. The exclusion criteria were: families who cared for MDs for less than 3 months; and were not present during the interview process. While the inclusion criteria of the health care provider, mental health cadre, and the Department of Health officer were: physically and mentally healthy; have participated and been involved in mental health program in the selected area of research; willing and able to provide in-depth information related to mental health services in the Pekalongan Regency.
Participant Characteristics.

Institutional Review Board Approval and Informed Consent
Ethical clearance for this study was obtained from the Research Ethics Committee (Number: 544/UN6.KEP/EC/2021), valid until July 8, 2022, for a duration of one year. Before conducting the Interview, the researcher explained to the participants the purposes of the study and gave them an informed consent form.
Data Analysis
The results of the interviews were made into verbatim transcripts. Then, verbatim transcripts were analyzed using thematic analysis with a framework of Colaizzi's method. It is transcripted without the participant's name, including double reading for each text to get an in-depth sense of the “comprehensive” participant experiences, putting phrases and statements which directly pertained to the phenomena in a significant statement, reviewing significant statements and identifying themes, and resubmitting the inquiry to participants for confirmation (Colaizzi, 1978). Colaizzi's method of data analysis is rigorous and robust and, therefore, a qualitative method that ensures the credibility and reliability of its results. It allows researchers to reveal emergent themes and their interwoven relationships. The researchers ensured the trustworthiness of the data through various methods. First, member checking involved verbally confirming certain statements with participants to ensure they accurately reflected the phenomena discussed (Credibility). Second, the completed transcripts, along with field notes, were provided to a data analyst to identify themes, allowing the supervisor to review the obtained data (Dependability). Thirdly, discussions were held with other researchers employing similar methods to ensure consistency and reliability of the findings (Confirmability). Last, descriptions of the identified themes were shared with different participant groups not involved in the research process to validate the results, including two patient families receiving nursing services, two mental health programmers as nursing service providers, and one representative from the Health Service as a policy maker (Transferability). Thematic Analysis discribed ini Figure 1.

Thematic Analysis.
Results
Participants Characteristics
The characteristic of participants is described in Table 2.
Research Results
This study found specific characteristics of participant and indicated four themes related to the opportunity of using e-coaching to empower MD families, namely the menus of e-coaching, the needs, supporting factors, and the hindering factors. Each theme will be explained in detail below.
Menus
Participants stated that their preference menus could be provided in an e-coaching to ensure the coaching type will benefit them. Menu is known as a list shown on the display of a computer from which a user can select the operation the computer is to performa (Menrriam-Webster, 2024). The kinds of components can be seen from their statements below:
Menu 1: health education and guidance for caring MD person
Participants said the mobile application could include health education on caring for and treating MD person. “Yes sir, a guide for caring for the mother is necessary” (P1) “Yes, how to teach families how to care for ODGJ (people with MD)..” (P20) “…maybe there is a lesson for the family, how to handle it, that is all, sir” (P8) “the patient's family can self-assess.. the family can recognize the patient's condition at home, for example, what kind of hallucinations are there.. what the delusion is…etc. Because it is closely related to health education. Medication adherence..” (P17)
Menu 2: patient data
Participant considers patient data as a beneficial menu “If possible, there is a menu of patient data to monitor them, sir” (P13). “.. personnel involved in handling MDs will obtain accurate data..” (P18)
Menu 3: consultation room
Two participants stated about the consultation room. “Maybe the consultation room, sir” (P3) “If possible, you can add another link for the first consultation, sir” (P8)
Menu 4: Treatment monitor, medicine monitor, and a reminder to visit a healthcare provider
Another essential menu is treatment monitoring. Four participants stated their opinion about this menu. “In my opinion..especially in monitoring taking medication…” (P17) “If there is this application, it is hoped it can help the community to take medicine regularly, sir” (P7) “it would be better if there was a link with the hospital, not PIC care so that any patient who dropped out of medication could be monitored. Because when person drop out of medication, the risk of relapse is high for severe MDs, which can eventually become zero again.” (P18) “Should be a warning when the patient should visit health center…” (P13). “Hopefully, this system will facilitate monitoring and evaluation..” (P21)
Menu 5: Interconnection, coordination, and early detection
Participants stated that interconnection and coordination between health care providers and village cadres should be provided in the e-coaching. “should involve cadres villages, security agency, and community health center… if the application is running.. everything is connected.. automatically… so that it can be done quickly, for example, if someone goes berserk and noisy..” (P16) “By using this system, we hope to be able to help, especially the health office, which has been reporting MDs were to be sidelined..” (P21) One participant said that a menu enabling to do early detection is beneficial. “in my opinion, for example, one of them is for early detection” (P8).
Menu 6: Video
Participant stated the need for video in the application. “Yes, there is a video menu so we can accompany families with MDs… Usually, ordinary people are afraid to care MDs, Sir..” (P17)
Menu 7: Explanation about MD.
The participant stated that the menu of MDs’ explanation is also essential. The explanation should be about hallucinations, self-care, etc. The full explanation is here. “I need an explanation about hallucinations, self-care deficit, social isolation, violence, and low self-esteem” (P16) “Please give me an explanation of anger, hallucinations, self-care deficits, and social isolation” (P13) “need an explanation about someone in a trance, rage, sleep disorder, restless” (P2)
Needs
They are developing e-coaching such a good chance, considering the participant's needs regarding a mobile application that can help their work as nurses and families of MD person. The E-coaching mobile application is an application that has good opportunities in society, considering the need for applications that can help their work as nurses and families of MD person. But currently the e-coaching App is still not available, so this application has the potential to be developed to increase family empowerment in the treatment of mental disorders People said, “There is no such application yet.. yesterday we followed the zoom from hospital Semarang, they said they will create…..but until now there has not been one…” (P15)
Supporting Factors
The supporting factors were also identified, such as the wide use of cell phones, the availability of Internet connection, and the availability of WhatsApp groups among participants. The detailed information can be seen below:
(1) Wide use of smartphone
Participants stated that they could use smartphones well “We can use a smartphone, sir..” (P15) “Oh, healthcare provider can use their smartphone” (P18)
“We can use a smartphone, sir..” (P20)
“I think the officer is using Android. So, it is not a problem. The more important is that the availability of notes on the Android so they can be printed if needed. It will make everything easier” (P10)
“Later, if I learn the application, I can use it on my smartphone…” (P9)
“Later, I will operate my smartphone so that I can use the application” (P11)
(2) Friendly internet connection Internet connections are now available in the area of research, as stated by the participants below: “If it is in the rural area, it is difficult. However, now all villages have WIFI at their village halls so we can access Applications easily… on average, 13 villages already provide WIFI… but at least 75 percent of the internet connection is covered….” (P15) “The signal covers all villages, Sir…. Because we are in the semi-urban area.. near the city” (P17).
“Good signal, never any interference” (P10)
(3) The availability of WhatsApp group The availability of WhatsApp groups helps them to communicate within the group, so every difficulty or problem of a patient or using an e-coaching Application might be discussed in the group. “My healthcare center has a group with mental health cadres. Thus, we can monitor from there… so we will know immediately if the patient faces a problem (P15)
Hindering Factors
The family's inability to use the smartphone and provide an internet connection was the hindering factor in using mobile apps. It contrasts with supporting factors, which means that most people using android do not totally understand how to use it. Other hindering factors are bureaucratic difficulties and difficulty reaching an internet connection in some areas. “..yes, but I can only answer the phone; WhatsApp cannot” (P2) “Not all people can access android” (P10)
“.. the problem is when I have no cellular data, sir” (P3)
“At Ujung Negoro village (read: rural), the internet connection is a bit difficult” (P15)
“In the mountains area is difficult to reach for the signal” (P7)
“That is the regulation, sir. … it is effortless to implement, but when it reaches the bureaucracy, it gets stuck” (P14)
Discussion
This research aims to examine the prospects for using e-coaching as a strategy and media for empowering families of MD person. The study produced numerous insights and ideas that were discussed in light of the findings.
Menus
Based on the result, participants provide insight into the menus that can be provided in the e-coaching applications, which will benefit them as families and caregivers of MD person. The menus appearing from interviews were: health education on how to care for and treat MD person, consultation room, treatment monitoring, Interconnection and coordination, Early detection, Video, and Explanation about the MD problem. We have consolidated the findings and made a summary based on the result, as shown in Table 3.
Themes and Subthemes.

Health education and MDs require detailed information so families can readily access it on one platform to explain the MD problem. Health education has continued to develop digital communication tools, and the communication marketplace has grown more crowded and complex, enabling people to navigate competing information sources and meaningfully engage with social and economic determinants of health. To lessen the consequences of chronic illnesses and enhance a person’s quality of life, nurses want to think about developing health education and monitoring support programs (Aree-Ue et al., 2022). Health knowledge among people and communities is significantly increased through health education (Abu-Baker et al., 2022; Kuo et al., 2021; Rasberry et al., 2022).
Online media discussions are accessible using a variety of formats (video, e-mail, virtual, telephone, What App). Participants of this study prefer using video and online consultation rooms as beneficial menus. The findings of this study offer insightful data that can help specialists and, more importantly (mental) healthcare organizations create the ideal environment for ongoing, excellent, and selective use of online consultation (Aidemark, 2022; Hassija et al., 2022; Schoenwald et al., 2022; Van Daele et al., 2022). With the collaboration of mental health services, vocational rehabilitation, welfare agencies, and other community programs, care coordination is high-quality and crucial in health services for treatment monitoring (deJong et al., 2021; Havlicek & Bilaver, 2021; Sagan et al., 2022).
The early detection menu is an additional menu that has to be developed. The previous study indicates that telemedicine helped early mental health detection during the pandemic. Early identification of MDs is relatively complicated during the pandemic; thus, increasing the accessibility of telemedicine services and delivering psychoeducation to the general populace was helpful (Cuomo et al., 2022). For common MDs, early detection and effective intervention at the community level should be emphasized. Governmental initiatives should concentrate on establishing MD healthcare centers, as established by the Ethiopian government when developing drug rehabilitation facilities to treat Khat and cigarettes (Legas et al., 2022). Although there is evidence that prompt diagnosis improves therapeutic outcomes, this is a challenging task since no single symptom is distinctive to this serious MD. Currently, a precise diagnosis of this type of condition might take at least six months, and it is based primarily on interviews and the presence of some observable, repetitive behavior or symptom as an indicator (Lillo et al., 2022). Thus, providing an early detection menu would improve MDs’ diagnosis. We recognize the importance of screening for awareness in early detection and management. Educating teachers concerning depressive symptoms and assessing them on a regular basis is critical for early detection and control (Bete et al., 2022).
Needs
The goal of e-coaching is to guide users to find new ideas or ways to overcome challenges or achieve desired goals. The findings of this study reveal that participants had a demand for e-coaching. It indicates that e-coaching has the potential to be a practical application for the community, including the mental-health community. With many favorable factors, like the accessibility of internet connections, the widespread usage of smartphones, and the availability of WhatsApp groups, this is an excellent opportunity. Recently, research has begun to investigate personality change through intervention in nonclinical populations. One attractive and innovative interventional avenue may lie in using digital applications to guide and support people in their desire to change their personality and trigger change processes (Allemand & Flückiger, 2022). Several studies highlight the need to promote mental health in various areas of life to improve the quality of mental health in families and communities (Karki et al., 2024).
Supporting Factors
It is applicable to develop e-coaching utilizing web apps since most Indonesian areas, including the villages, already have internet access. The number of villages that could not receive the signal also decreased from year to year. In 2019, the number of villages unable to receive signals was as many as 5,972 (7.11 percent) villages, which declined in 2020 to 5,705 (6.79 percent) villages and continued to decline in 2021 to only 5,158 (6.13%) villages. The proportion of villages that received cellular phone signals rose yearly (BPS-Statisics Indonesia., 2022) Another supporting factor is the availability of WhatsApp groups supporting discussion among families and healthcare providers. This group enables the community to communicate well, discuss with MD person, and even talk about e-coaching in the future. Furthermore, e-coaching can be performed via the WhatsApp application, which enables the development of unique applications with e-coaching menus.
Hindering Factors
As an online application, e-coaching uses an internet connection. However, the number of villages in Indonesia covered by internet connection is high, and several villages, especially in rural areas, lack it. The lower population density and the lack of digital infrastructure in such rural areas make it difficult to develop technology-driven private businesses and public services (Gómez-Carmona et al., 2023). Despite the internet problem, using a smartphone with a simple application is applicable.
E-coaching has been used for various purposes such as for sleep problems, solution for older, coach for educator, and persuasive system design (PSD) models for caregivers (Kuhn et al., 2022; Möller et al., 2022; Premanandan et al., 2023; Rowland et al., 2021). Similar to the general population, people with anxiety or depression own and utilize digital health tools, which suggests that these technologies offer new potential for health promotion among those with these diseases (Onyeaka et al., 2021; Paruchuri et al., 2021). Thus, e-coaching has the potential to develop in help families with a patient with MDs to be more aware of taking care of an MD person and reduce their anxiety.
Integrative empowerment had a significant impact on increasing the family's ability to care for and prevent relapses in MD person (Iswanti et al., 2024). The application will also help the Indonesian community as digital tools might improve the self-monitoring practice among MDs and families. It also improves the quality of life of those as digital services maintain confidentially, preventing family MDs from meeting too many people outside their homes. A previous study stated that unfair social health disparities, poor physical health, and poor behavioral health affect those who struggle with mental illness. Developing customized and effective self-management and self-monitoring strategies could be aided using these digital tools and services (Ye et al., 2022).
While virtual coaches and similar Digital Mental Health Platforms offer promising solutions to overcome barriers to accessing mental health services, their effectiveness could be constrained if individuals lose interest and fail to sustain engagement with them (Venning et al., 2021). Thus, after finishing the development of e-coaching, we consider conducting a clinical study to test the effectiveness of the application on MD person.
Strengths and Limitations
Family empowerment can be used to promote health improvement programs. The current digital age's utilization of information technology can strengthen families’ capabilities, particularly in treating mental problems at home with the E-Coaching Application, which is easily accessible by smartphone. Families and other health professionals from various levels of mental health services have participated in this research and can contribute to improving the quality of health services while reducing the risk of relapse in patients with mental disorders.
Implication for Practice
As a part of mental health services, nurses can investigate the enormous potential of recent information technology advancements to strengthen the role of families in treating MDs at home, one of which is the creation of an E-coaching application that families with smartphones can use.
Conclusion
This study aimed to explore the opportunity and the benefits of e-coaching as a method and media for empowering families of MD person. There were four themes related to using e-coaching to empower families with a family member with an MD: menus, needs, supporting factors, and hindering factors. The findings show that developing e-coaching as a method and media is beneficial for person, families, and healthcare providers to increase families’ capacity to treat MDs at home, the findings of this study can be used to create an e-coaching application that is simple for families to use via smartphones. Nurses who provide mental health care should monitor how local families utilize this application.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Universitas Padjadjaran Bandung and Universitas Muhammadiyah Pekajangan Pekalongan for their invaluable support. Special thanks are also extended to Dyah Putri Aryati, Siti Khuzaiyah, Nur Intan Kusuma, and Eko Mugiyanto for their insightful comments and suggestions during the revision process.
Author Contributions
M.A.: drafting the paper, methodology, investigation, validation, and writing original draft; N.S.: methodology, formal analysis, and data curation; A.S.: methodology, formal analysis, and data curation; F.S.i,.: methodology, formal analysis, and data curation; and all authors contributed to the conceptualization and approved the final version of the manuscript.
Consent for Publication
The authors give our consent for the publication of the manuscript in the SAGE Open Nursing Journal. We have reviewed the final version of the manuscript and approve of its contents and the submission for publication. We confirm that the manuscript has not been previously published and/or is not under consideration for publication elsewhere.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethic Approval and Consent to Participate
Ethical clearance for this study was obtained from the Research Ethics Committee (Number: 544/UN6.KEP/EC/2021), valid until July 8, 2022, for a duration of one year. Before conducting the Interview, the researcher explained to the participants the purposes of the study and gave them an informed consent form.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Universitas Padjadjaran Bandung and Universitas Muhammadiyah Pekajangan Pekalongan.
Study Approval Number
544/UN6.KEP/EC/2021.
Use of Ai Software
The authors declare that AI (Grammarly) was used to only check the clarity and readability of the manuscript the authors are responsible for the contents of the manuscript.