
Abstract
Introduction
Poststroke internal stigmatization in patients is often overlooked, yet it makes significant contribution to their recovery and quality of life. After stroke, the survivors often have negative perception toward themselves triggered by the internal stigma. Consequently, it affects the rehabilitation outcomes and increases the risk of long-term complications. Therefore, deeper analysis related to the factors influencing the internal stigma was crucial in order to develop an appropriate and innovative strategy to overcome this issue and optimize the recovery in stroke survivors.
Objective
This study aimed to identify predominant factors influencing the internal stigma in stroke survivors in Indonesia.
Methods
This study used descriptive analytical design and applied stratified nonprobability consecutive sampling involving 439 poststroke respondents from nine hospitals in Bali throughout 2023. This study used various instruments, namely stroke stigma scale (SSS), perceived family support, stroke self-efficacy scale (SSEQ), stroke awareness questionnaire, self-acceptance scale, knowledge of stroke and the respondents’ demographic data. The analysis was conducted using Pearson product–moment correlation and multiple regression.
Results
The results from multiple regression analysis showed that self-acceptance (β = .374, p = .000), self-awareness (β = .132, p = .000), self-efficacy (β = .154, p = .000), family support (β = .090, p = .015), age (β = .083, p = .000), and stroke symptoms (β = −.347, p = .000) could explain the internal stigma for 62.8% (F = 124.266, p = .000).
Conclusion
Self-acceptance became the most predominant factor towards internal stigma in the stroke survivors because it showed the ability in accepting changes after stroke, which eventually helped them to overcome the challenge and free themselves from internal stigma that interrupted the process of recovery and adaptation to poststroke physical and psychosocial changes.
Introduction
Stroke has been the second most common cause of death after cardiovascular disease (Bartoli et al., 2018). In 2021, in every six deaths caused by cardiovascular disease, one was caused by stroke. In the US, every 40 s, one person has stroke, and within every interval of 3 min 14 s, one person dies of stroke (CDC (Centers For Disease Control and Prevention), 2021). Every year, more than 795,000 people in the US have stroke, with approximately 610,000 new cases. Only a quarter, about 185,000 cases, occurred on a person who had previously had stroke. In terms of the type, 87% of stroke cases were ischemic stroke, which was caused by the interruption or blockage of blood flow to the brain (CDC (Centers For Disease Control and Prevention), 2021). Stroke causes approximately 5.5 million deaths every year. Apart from having an impact on high mortality rates, stroke also results in chronic disability rates which reached up to 50% in 2018 and was estimated to continue to increase in the following years. Therefore, stroke is a major public health problem with serious economic and social impacts (Donkor, 2018).
Stroke has also become a leading health concern in ASEAN countries. Based on data from South East Asian Medical Information Center (SEAMIC), Indonesia has the highest death rate for stroke, followed by Philippines, Singapore, Brunei, Malaysia, Thailand, and China (Suryani Panjaitan et al., 2020; Venketasubramanian et al., 2017). The increasing prevalence of stroke in Indonesia, especially in Bali, is an issue that requires special attention, considering that the impacts can be worse if not handled properly. Stroke, as a serious medical condition, can disrupt the daily lives of individuals, families and communities. Thus, increasing public awareness and improving the access to health services are required to face this complex challenge (Restikasari et al., 2022).
Review of Literature
Several literature reviews mention various struggles experienced by stroke survivors after stroke, namely long-term physical disability like paralysis and inability to move, perceptual disorders relating to vision, hearing and speech, emotional disorders such as anxiety, stress, and depression, low self-esteem, feeling ashamed of their condition, losing their role in the family, and low optimism to recover that could affect their quality of life (Dewi et al., 2020; Masdiana et al., 2022; Payton & Soundy, 2020). Their inability to develop emotional adjustment to poststroke symptoms make them reluctant to follow the rehabilitation process and tend to be inconsistent to do medical follow-up at the healthcare facilities (Kalavina et al., 2019). It can be seen from the poststroke rehabilitation proportion response in healthcare facilities in Bali which showed that 40.28% did not maintain regular medical follow-up, and 15.76% did not come back after being diagnosed of stroke (Tini et al., 2020).
Furthermore, the substantial financial outlay of poststroke care and rehabilitation also affects the family's economic stability, which leads to the unwillingness to go to the healthcare facility. This situation arises due to the condition of stroke survivors and their families who tend to have negative thoughts of stroke, which eventually develops internal stigma in stroke survivors (Göksu & Katı, 2021). Internal stigma includes enacted stigma, which is based on the actual experience of being discriminated in social environment, and felt stigma, which refers to feeling ashamed, different or discriminated (Minfang et al., 2019). A study conducted in China showed that 90% of stroke survivors had felt stigma and 72.5% had enacted stigma (Deng et al., 2019). A study in Africa found that 16.9% of stroke survivors had poor internal stigmatization (Akinyemi et al., 2021). Meanwhile in Indonesia, 63% had mild stigma and 37% had moderate stigma after stroke, but there has not been much research related to internal stigma on stroke survivors conducted in Indonesia (Yuniarti, 2022).
Poor internal stigmatization in stroke survivors might affect their motivation to follow the rehabilitation and therapy and make them doubt their ability to fully recover (Fan et al., 2023). Internal stigma also makes them decline help and support from other people, accusing that they are a burden on their family or society. Feelings of hopelessness, frustration or depression which might arise due to internal stigma could worsen their emotional condition and interfere with their overall recovery process (Göksu & Katı, 2021). Thus, special attention towards this issue is required because poor and prolonged internal stigma can cause stroke recurrence, reduce motivation and initiation to recover, and interrupt the rehabilitation process, which might worsen the condition and increase the healthcare cost (Deng et al., 2019; Zheng, 2022).
Internal stigma, or self-negative perception due to certain condition, is strongly influenced by the local community culture and might affect the quality of life. People who feel humiliated by the community due to certain characteristics or conditions oftentimes develop internal stigmatization, which can lower their self-esteem and quality of life, so this can prevent them from seeking the care and support they need, and disrupt their overall quality of life (Harris, 2023).
Bali, as one of the tourist provinces in Indonesia with numerous local cultures, apparently has a fairly high stroke rate with a fairly high risk of recurrence if appropriate efforts are not made to reduce the potential for internal stigma. One effort that can be made to reduce the prevalence and negative impacts of stroke is to increase self-awareness of stroke survivors or their families concerning prevention and the rehabilitation process (Kariasa et al., 2022). Additionally, investigating factors influencing internal stigma would give insight to nurses to help patients and families to keep their quality of life. Therefore, it is very important to explore in depth the level of stigma and factors that influence negative perceptions among Balinese people who have experienced a stroke. It is hoped that the results of this research can be a valuable reference for health professionals in designing effective and targeted intervention programs to overcome internal stigma after stroke (Kariasa et al., 2022; Yuniarti, 2022).
Objective
This study aimed to identify predominant factors influencing the internal stigma in stroke survivors in Bali Province, Indonesia.
Research Question
What are the factors influencing the internal stigma in stroke survivors in Bali Province, Indonesia?
Method
Study Design
This study used quantitative cross-sectional design and applied stratified nonprobability consecutive sampling to analyze the factors related to poststroke internal stigmatization in patients. This study was conducted from June to November 2023. The study followed STrengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guidelines (Cuschieri, 2019; Vandenbroucke et al., 2007; von Elm et al., 2007).
Sample
The sample size was determined by G*power linear multiple regression. We set the effect size to 0.07, the significance level to .05, the power to 0.95, and the number of predictors to 15. The results showed 411 respondents, and the total with a 10% attrition rate was 452. However, only 439 respondents finished the questionnaires appropriately.
Inclusion/Exclusion Criteria
The study used convenient proportional sampling. It applied several inclusion criteria, namely stroke patients with compos mentis consciousness who were willing to be the respondents, aged ≥18 years old, undergoing treatment in hospital as outpatients, and living with family. The patients were excluded if they had aphasia, severe depression, cognitive impairment, and were under antidepression medication/psychiatric medication.
Instruments
The questionnaire pack had seven parts. First, it explored the demographics of the participants, including their age, length of illness, sex, education, symptoms, caregiver, relationship with caregiver, medication, comorbidity, and habit. Subsequently the remaining parts covered the internal stigma scale, family support, stroke self-efficacy, self-awareness, self-acceptance, and knowledge of stroke.
The questionnaire used to assess the internal stigma was stroke stigma scale (SSS) developed in 2018 by Minfang Zhu et al. to evaluate stigma in stroke patients, consisting of 16 questions and divided into four main aspects: physical weakness (four questions), social isolation (three questions), discrimination experience (four questions), and internalized stigma (five questions). The respondents were asked to evaluate their stigma experience in 7 days by using Likert scale ranged 1–5, thus the total score for this scale ranged from 16 to 80, where the higher the score, the higher the stigma level they had (Zhu et al., 2019). The validity and reliability testing results showed Cronbach α = .92 and Pearson correlation ranged between .73 and .90 (Zhu et al., 2019). The questionnaires were translated by the experts and reviewed by the expert panels. Two professional translators were independently translated. Then, the results were compared by three experts who hold doctoral degrees (one nursing instrument expertise and two experts in stroke) and one nursing professor in medical-surgical. The reliability in this study was 0.84.
The questionnaire used to assess family support was perceived family support developed by Procidano and Heller (1983), which was modified for stroke condition, consisting of 18 questions of yes/no/don’t know answer options (Yuniarti, 2022). The answers were assessed by giving 1 for every “yes” answer and 0 for every “no” and “don’t know” answers and vice versa for negative statements. Negative statements were written in items no. 3, 4, 15, and 18. The scores were accumulated by calculating the score from every question. The higher the score, the higher the family support level. This questionnaire has been tested for validity and reliability, with r-count > .374 and Cronbach α = .744 (Yuniarti, 2022). The reliability in this study was 0.85.
Poststroke self-efficacy in stroke patients was assessed by using stroke self-efficacy scale (SSEQ). We considered the questionnaire because have been used in the Indonesian stroke population and might be involved in some way with stigma. Based on the validity and reliability testing, they demonstrated that all items in this questionnaire were valid and reliable. The validity test on 13 questions resulted in r = .538–.828. This questionnaire was reliable, considering that the Cronbach α was.937 (Kariasa et al., 2022). The reliability in this study was 0.92.
Self-awareness was assessed by using awareness scale which was modified to measure the patients’ self-awareness towards deficits or problems caused by stroke or other neurological condition (Kariasa et al., 2022). We considered the questionnaire because have been used in the Indonesian stroke population. The score ranges from 23 to 115 with a 5-point Likert scale (1–5). A score higher than 60 is adequate, otherwise inadequate. This questionnaire has been tested for reliability as well, with Cronbach α = .76 (Kariasa et al., 2022). The reliability in this study was 0.96.
The next questionnaire aimed to assess self-acceptance by using self-acceptance scale. We considered the questionnaire because have been used in the Indonesian stroke population. This questionnaire measured the level of self-acceptance by observing the stages of self-acceptance experienced by the patients. The score ranges from 25 to 100 with a 4-point Likert scale (1–4). A score higher than 50 is adequate, otherwise inadequate. This questionnaire has been tested for its validity and reliability, with r-table = .444 and Cronbach α = .910 (Irawandi, 2018). The reliability in this study was 0.87.
The questionnaire to assess knowledge was a stroke knowledge test (SKT) which comprised 15 statement items relating to signs and symptoms of stroke, risk of stroke, and mitigation. This questionnaire was developed by the Principal Investigator (PI) (Cyntia et al., 2020). Each statement was given 1 point, which was accumulated. The reliability in this study was 0.63.
Data Collection Procedure
The procedure was started by identifying the respondents who were stroke survivors through hospitals, clinics, and health organizations selected from nine cities in Bali. A total of 452 questionnaires were distributed. The proportional method was arranged based on the number of stroke survivors in each area. The researchers contacted the hospital and coordinated with the hospital's outpatient department team to facilitate questionnaire completion.
After identification, the respondents were selected based on the inclusion and exclusion criteria. Furthermore, the respondents were invited to participate in this study by explaining the objective and procedure of the study in details. Those who agreed to participate were asked to completed the consent form and were informed of their rights as the subjects, including the right to withdraw from the research anytime they wish with impact to their treatment. After filling and signing the informed consent, the respondents were asked to answer the questionnaires related to predominant factors influencing internal stigma after stroke. Respondents completed the questionnaires independently, but the research team was ready to provide assistance or explanation if needed. During the process, research ethical principles were strictly maintained, including the privacy and confidentiality of respondents’ data. Respondents were assured that their identities and personal information would be kept confidential. After completing all research procedures, the respondents were given appreciation for their participation in this research.
Data Analysis
The data were tabulated and edited using SPSS 24 software (IBM Corp., Armonk, NY, USA). The statistical analyses used in this study were descriptive analysis, Pearson product–moment correlation, and multiple regression. Descriptive analysis was used to identify the respondent characteristics. Pearson correlation aimed to measure the relationship between two variables in the study. In this context, Pearson product–moment correlation was used to analyses the relationship between the variables observed in the research and measure the extent to which the relationship was solid and significant.
Multiple regression analysis aimed to identify the factors influencing the internal stigma in stroke patients at the same time. The stepwise method was used. We separated and blocked the main variables and demographic variables. The regression testing was carried out to determine how much these factors were able to explain the internal stigma with a significance level of 95% (α = .05).
Effect sizes based on Cohen's f2 are categorized as small (f2 = 0.02), indicating modest differences with limited practical significance; medium (f2 = 0.15), suggesting moderate differences often with meaningful implications; and large (f2 = 0.35), signifying substantial differences with significant practical or clinical relevance (Cohen, 1977).
Ethical Considerations
This research has received ethical approval from the Research Ethics Committee. This ethical approval confirmed that this research has been assessed in accordance with the principles of research ethics, including the protection of privacy, data security, and the rights of research subjects. Therefore, it can be ensured that all research procedures were carried out in accordance with the applicable ethical standards.
Results
Respondent Characteristics
From the respondent characteristics in Table 1, it can be seen that most of the patients were male (60.8%) and the mean age was 63 years old. Most of them graduated senior high school (30.8%), had stroke for 3 years with symptoms in their left side of the arm and leg (40.3%). Most of them had caregiver (97.5%), which was mostly their child (37.6%). Most of them consumed antihypertensive drugs (66.7%) and had comorbidity of hypertension (64%). Most of them did not smoke nor drink alcohol (49.7%). On average, the patients had adequate self-awareness (62.76 ± 16.62), adequate self-acceptance (65.39 ± 9.69), moderate self-efficacy (32.69 ± 7.52), very supportive family (46.01 ± 5.89), lack of knowledge related to stroke (3.97 ± 1.79), and high internal stigmatization (50.81 ± 6.90).
Respondent Characteristics (N = 439).

Factors Influencing Stroke Internal Stigma
The correlation analysis results, presented in Tables 2 and 3, showed that caregiver existing (r = .150, p = .001), medication (r = −.106, p = .013), smoking and drinking alcohol habit (r = −.143, p = .001), self-awareness (r = .566, p = .000), self-acceptance (r = .688, p = .000), self-efficacy (r = .383, p = .000), and family support (r = −.202, p = .000) had significant relationships.
Correlation Between Demographics and Variables (N = 439).

Note: Awareness (1), Acceptance (2), Self-efficacy (3), Family support (4), Knowledge of stroke (5), and Internal stigma (6).
*p < .05. **p < .001.
Correlation Among Variables (N = 439).
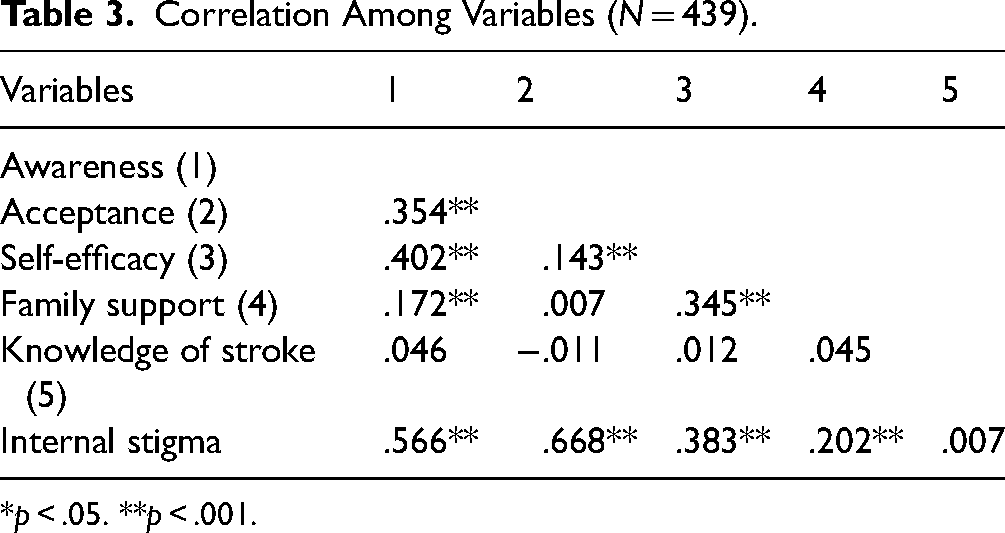
*p < .05. **p < .001.
The multicollinearity was assessed through variance inflation factor (VIF) that showed there was no multicollinearity in this study with value ranging from 1.00 to 1.36. The multiple regression analysis results, presented in Table 4, showed that self-acceptance (β = .374, p = .000), self-awareness (β = .132, p = .000), self-efficacy (β = .154, p = .000), family support (β = .090, p = .015), age (β = .083, p = .000), and stroke symptoms (β = −.347, p = .000) can explain the internal stigma for 62.8% (F = 124.266, p = .000). Based on the Cohen's f calculation, the effect size was high (1.724). The self-acceptance had a high effect size (f2 = 0.81), and the rest of the variables had a small effect size, including self-awareness (f2 = 0.14), family support (f2 = 0.08), self-efficacy (f2 = 0.03), age (f2 = 0.02), and stroke symptoms (f2 = 0.01).
Multiple Regression and Effect Size Results (N = 439).

Discussion
This study found several factors that influence the internal stigmatization. Based on the result of multiple regression analysis, the factors influencing the internal stigma are self-acceptance, self-awareness, self-efficacy, family support, age, and stroke symptoms.
Self-acceptance emphasizes the importance of accepting and respecting ourselves, including strengths and weaknesses. In terms of internal stigma, people with high self-acceptance tend to be able to overcome negative image of themselves that might occur due to stigmatization, like the impacts on stroke patients (Lowe et al., 2021). In Balinese culture, the concept of self-acceptance does not only include acceptance of physical or health conditions, but also involves spiritual and social aspects. Those who are able to accept themselves well in this context will be more likely to have a positive view of themselves, even in facing challenges such as stroke (Kariasa et al., 2022; Soetjiatie et al., 2022).
Conceptually, self-awareness can influence the way the person responds to the internal stigma, particularly in stroke patients. Increased self-awareness allows them to better understand the impact of stigma on their health and lives. With a better understanding of their health condition, stroke patients can face stigma more effectively and develop adaptive coping strategies (Adigwe et al., 2022). These findings were also confirmed by Smith in 2020, who stated that stroke patients with higher level of self-awareness tended to have a better ability to deal with internal stigma related to their condition. They showed that increased self-awareness allows patients to develop optimal coping strategies in dealing with their condition. Thus, self-awareness has an important role in reducing the negative effects of internal stigma in stroke patients (Lindsay et al., 2020; Smith et al., 2020).
This study also showed that stroke patients with high level of self-efficacy had better capability to overcome their internal stigma. They tended to have a more positive attitude towards themselves and the ability to deal with negative views from others (D. F. Wang et al., 2022).
Conceptually, self-efficacy refers to an individual's belief in their ability to overcome difficult situations and achieve desired goals. Persons with high levels of self-efficacy tend to have strong beliefs in their abilities and independence in facing challenges, including stigma related to medical conditions such as stroke. With confidence in their abilities and independence, they are also able to seek and obtain the support they need to face the stigma, such as family support (Yu et al., 2021).
Strong family support can reduce internal stigma because the emotional support from family members, such as moral support, affection and attention, can increase their self-confidence and self-esteem (Chang et al., 2022). This emotional support gives patients a sense of security and psychological support, so they are able to overcome stigmatization and negative feelings related to their condition (Guo et al., 2021). In addition, practical support from their family, such as help with daily activities, physical care, and financial assistance, can also reduce internal stigma. These will make them feel better supported in facing challenges that may arise due to their condition, so they do not feel socially isolated. Strong family support can increase the self-confidence in stroke patients. By feeling supported by the people closest to them, patients feel more confident in facing the stigma and difficulties that may arise, because stroke can strike regardless of age (Deepradit et al., 2023).
This study showed that older people tend to have lower levels of internal stigma because they tend to have better self-confidence and adjustment to changes and challenges in their lives (Khalil & Lahoud, 2020). This is probably because they have more life experience, including experience in overcoming challenges and stigma that may occur in their lives. They are also more mature in managing emotions and dealing with negative views from others. Therefore, age can be a significant factor in influencing how individuals respond to internal stigma related to stroke, including the sequelae (Silván-Ferrero et al., 2020). This is because more severe or prominent stroke symptoms tend to increase internal stigma because individuals may feel embarrassed or have low self-esteem due to the physical or cognitive limitations caused by these symptoms. In addition, psychological and social aspects may have a more dominant role. Negative perceptions from other people and an unsupportive social environment can also worsen the internal stigma (Ge et al., 2021).
Another important finding that demographic data presented in this study provided an important picture of the characteristics of poststroke patients in this community. First, the results showed that the majority of respondents are male, which illustrated the tendency that men are more susceptible to stroke than women (Arauz et al., 2020). Factors such as lifestyle, genetics, and hormones might contribute to this difference (M. Wang et al., 2022). Second, the mean age of respondents was classified as old, which highlights that ageing is the main risk factor for stroke (Tromp et al., 2021). It is in line with the literature showing that the risk of stroke increases with age (Morseth et al., 2021). Third, the education level of the respondents, which senior high school graduates dominated, showed the need for health education programs that are tailored to the literacy level and understanding of people regarding stroke (Gan et al., 2022). In addition, considering local culture and beliefs is an important point in designing health education programs. The use of an approach that is aligned with the values and cultural norms of Balinese society strengthens the patient's acceptance and involvement in the program (Kariasa et al., 2022). It is expected to increase the patient's understanding about stroke, increase the awareness of risk factors and symptoms, and provide information about the appropriate prevention and management steps. Therefore, it can reduce the incidence of secondary stroke and improve the quality of life of stroke patients in Balinese community (Dewi et al., 2020).
Fourth, Internal stigma may hamper the efficiency of rehabilitation owing to the condition of self-acceptance, which is a factor that is influenced by the length of time that illness lasts, even when some rehabilitation is provided. Therefore, it is important to provide sustained attention to stroke patients so that they can receive optimal support and treatment to functioning independently in daily life (Glenis et al., 2021; Tini et al., 2020; Yusrika et al., 2020). Fifth, the majority of respondents had a companion, mostly their child, indicating the importance of the family's role in providing support and care for stroke patients (Abu et al., 2020). This underscored the need for strong family support to improve the quality of life of stroke patients (Elmawla et al., 2022). Sixth, most of the respondents consumed antihypertensive drugs and had comorbidity of hypertension, indicating a strong relationship between hypertension and stroke. Effective management of hypertension is pivotal in secondary stroke prevention (Przykaza, 2021). Lastly, low levels of smoking or alcohol consumption indicated that the majority of respondents did not have behavioral risk factors that contribute to stroke. However, it is important to note that there are other behavioral risk factors, such as diet and physical activity that also play an important role in the development of stroke (Lin, 2021). Overall, in-depth understanding of the demographic characteristics of poststroke patients is the key to reducing internal stigma and improving their quality of life by developing effective interventions against internal stigmatization (Kariasa et al., 2022).
Strength and Limitations
To our knowledge, this article is the first investigation to specifically focus on factors influencing stroke internal stigma that comprehensively explored demographics (age, length of illness, sex, education, symptoms, caregiver, relationship with caregiver, medication, comorbidity, and habit), family support, stroke self-efficacy, self-awareness, self-acceptance, and knowledge of stroke. Therefore, it can be considered the strength of the study.
There were several limitations which were found in this study. One cluster province might not generalize Indonesia. This study used cluster random sampling to tackle this situation. Further studies could use a multicenter study to increase generalization in Indonesia. Second, this study did not separate the first-time stroke and recurrent stroke. The first experience and the second might give different results of factors. Third, other factors could influence stroke internal stigma that was not explored in this study. Fourth, the translated and developed questionnaire was not checked yet for construct validity further study would investigate this. Then, symptom severity was based on the patient's objectivity. Further studies need to limit the time of discharged patients to check the severity (degree of muscle strength) and its relation to internal stigma. Last but not least, the questionnaire might be too long, which impacts the stroke survivors when they fulfill it.
Implications for Practice
This research has far-reaching ramifications for both healthcare practitioners and politicians. Acknowledging the complex and diverse characteristics of internal stigma experienced by individuals who have suffered from strokes, it is imperative for interventions designed to alleviate stigma to employ a comprehensive approach that effectively targets the fundamental factors highlighted in this research. It is imperative for healthcare practitioners to give precedence to therapies that promote self-acceptance, self-awareness, and self-efficacy in stroke survivors. This approach will enable patients to effectively manage the difficulties linked with stigma. Furthermore, endeavors to improve family support networks and customize interventions according to age and stroke symptoms can also aid in diminishing internal stigma and fostering comprehensive well-being among individuals who have experienced a stroke. Policymakers can employ these findings to guide the creation of focused initiatives and policies with the goal of reducing the social stigma surrounding stroke survivors and enhancing their overall well-being. By thoroughly considering these aspects, stakeholders can strive to establish a more supportive and inclusive environment for those who have disabilities caused by strokes.
Conclusion
Deep understanding related to predominant factors influencing poststroke internal stigma in stroke survivors in Balinese community has significant implication for developing an effective and continuous intervention. This study identified several crucial factors, namely self-acceptance, self-awareness, self-efficacy, family support, age and stroke symptoms which play a role in shaping individual perceptions and experiences towards stigma. With a deeper understanding of these factors, intervention measures that can be adapted to local needs and context can be developed to reduce internal stigma and improve the quality of life of stroke patients in Bali, Indonesia, and globally.
Footnotes
Acknowledgments
We would like to express our gratitude to Universitas Indonesia for its full support, both moral and material, which has provided a strong foundation for this research. Furthermore, we also express our great appreciation to all respondents and related institutions who have demonstrated extraordinary collaboration, providing a solid foundation for the success of this research. We would also like to thank Ketut Lisnawati and Ni Made Nopita Wati, who helped with the data collection process.
Author Contribution
I Made Kariasa (IMK), Yupin Aungsuroch (YA), Elly Nurachmah (Professor), Prima Agustia Nova (PAN), Ni Luh Putu Thrisna Dewi (NLPTD), I Gede Juanamasta (IGJ), and Rapin Polsook (RP) made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. IMK, YA, EN, PAN, NLPTD, IGJ, and RP involved in drafting the manuscript or revising it critically for important intellectual content. IMK, YA, EN, PAN, NLPTD, IGJ, and RP gave final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This research has received ethical approval from the Research Ethics Committee Universitas Indonesia, reference number: KET-114/UN2.F12.D1.2.1/PPM.00.02/2023. This ethical approval confirmed that this research has been assessed in accordance with the principles of research ethics, including the protection of privacy, data security, and the rights of research subjects. Therefore, it can be ensured that all research procedures were carried out in accordance with the applicable ethical standards.
Funding
Funding for this research was fully provided by Universitas Indonesia through the PUTI Grant program which reflects a strong commitment to supporting quality research and facilitating the development of the academic and innovative potential of researchers.