
Abstract
Introduction
Early identification of developmental dysplasia of the hip (DDH) is necessary to minimize its negative effects. Ultrasound screening is useful for detecting DDH in hospitals. Awareness about community-based screening systems is low in Japan. Despite established nationwide home visiting services and child health checkups in the country, more than 10% of DDH patients are diagnosed at the age of ≥1 year. This review aimed to clarify the status of universal ultrasound screening for DDH among infants in community settings in Japan.
Methods
The electronic databases of Igaku Chuo Zasshi, MEDLINE, CHINAL, ERIC, and APA PsycInfo were searched for articles published between 2002 and 2022. Articles were evaluated with the reach, effectiveness, adoption, implementation, and maintenance framework.
Results
In total, 148 articles were identified. Two articles were manually added, and 67 articles were excluded through abstract reviews, of which 20 were duplicates. Finally, 18 articles were included in the analysis. There are two types of universal ultrasound screening in community settings: municipality-led and hospital-led. Since 1992, municipality-led screening has been conducted during public infant health checkups in five municipalities. Six hospitals implemented ultrasound screening. The participation rate was around 90%. The Graf method is typically used for this purpose. The prevalence of abnormal hips was 3.6%–16.6%. Owing to limited human resources and skills in ultrasound, all studies mentioned the necessity of a universal screening system for the early detection of DDH.
Conclusion
Embedding universal ultrasound screening in community health checkup systems enables collaboration between healthcare professionals and caregivers to improve health inequities and ensure early detection of DDH cases.
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a critical public health issue, and the global incidence is 0.2–120.1 per 1,000 (Kuitunen et al., 2022). DDH causes adverse health outcomes, including early development of osteoarthritis (Hasegawa et al., 1992), low quality of life and psychosocial well-being (Gambling & Long, 2019), and burden of medical expenditure (Harper et al., 2021). Important risk factors for DDH include breech position, female sex, and family history (O’Beirne et al., 2019). The early detection and treatment of DDH are crucial for preventing adverse outcomes, especially for developing hip osteoarthritis in the elderly (Agostiniani et al., 2020).
Traditionally, physical examination is a common strategy for the early detection of DDH, including the Barlow (1962) and Ortolani (1937) signs, Allice signs, limited abduction, and checking for asymmetric skin folds (Kang et al., 2019; Liu et al., 2022). Owing to the low sensitivity of clinical examinations (Chavoshi et al., 2022), radiological examinations are often used to prevent overlooking the signs of DDH (Norlén & Faergemann, 2022). Ultrasound screening methods have been developed since the 1980s (Graf, 1980; Harcke et al., 1984; Morin et al., 1985). There was strong agreement that clinical examination and ultrasonic screening were essential to assess suspected DDH cases in newborns and infants (O’Beirne et al., 2019).
Before 1965, the frequency of DDH in Japan ranged from 1.1% to 3.5% as newborns had trouble moving their legs because of “swathing diapers” (Yamamuro & Ishida, 1984). Local governments are in charge of preventing DDH cases through health screening and education during neonatal home visits and 4-month checks for infants. Public health nurses (PHNs) and midwives (MWs) promoted DDH prevention campaigns and decreased prevalence to 0.1%–0.3% (Yamamuro & Ishida, 1984). Despite hip dislocation being checked during newborn home visits and 4-month-old infant health checkups in Japan (National Center for Child and Development, 2017), a nationwide survey showed that 11.5%–15% of DDH cases were diagnosed after the age of one year (Den et al., 2023; Hattori et al., 2017). Only 2.3% of local governments implemented universal ultrasonic hip screening in Japan (Yoshioka-Maeda et al., 2023). However, the actual situation of universal ultrasound examination in Japan has not been reviewed, and the details remain unclear. Therefore, this review aimed to clarify the status of universal ultrasonic screening for DDH among infants in community settings in Japan.
Methods
A scoping review was conducted to identify the current status of universal ultrasound hip screening and to gain insight into the early detection and prevention of DDH. Scoping reviews are used to map and understand the concepts underlying a given research area. This study followed PRISMA-ScR (Tomori et al., 2020; Tricco et al., 2018).
Search Strategy
Literature was searched using the Igaku Chuo Zasshi, MEDLINE, CHINAL, ERIC, and APA PsycInfo databases. The search was conducted for studies published from 2002 to 2022. For Igaku Chuo Zasshi, a Japanese medical literature database, researchers used Japanese words as search terms: “Kankotsukyuukeiseihuzen” (DDH in Japanese) or “kyuugaikeiseifuzen” (acetabular dysplasia in Japanese) or “Kokansetsu” (hips) and “nyuuji” (infants), “chouonpa,” “echo” (ultrasonography). Three search terms were used: thesaurus, title, and abstract. For other databases, the keywords used were (“Japan” [Title/Abstract] AND (“DDH” [Title/Abstract] OR “development dysplasia of the hip” [Title/Abstract] OR “acetabular” [Title/Abstract])).
Selection of Articles
Original articles and case reports were eligible because of the possibility of pilot projects or short reports from municipalities. Conference proceedings that mentioned ultrasound for diagnosis were eliminated, as were those that did not reference screening or screening techniques including ultrasounds for DDH. Programs were included where ultrasound screening for the infant population was implemented before the detection of signs of DDH. Selective screening, which only included infants for whom signs or risk factors of DDH were identified through interviews or physical examinations, was excluded.
The first author screened all the identified articles with titles. The first and second authors independently examined the abstracts. The full text was examined independently by the first and third authors. Inconsistencies were resolved through discussion, and, if necessary, a specific author made the final decision.
The PRISMA flow diagram is shown in Figure 1. The number of publications selected in the different phases of this scoping review, along with the final number of articles included, is presented.

PRISMA flow diagram.
Data Charting Process
First, based on the screening provider (municipalities, hospitals, and clinics), researchers identified the pattern of the DDH screening system using ultrasound in Japan. Second, the reach, effectiveness, adoption, implementation, and maintenance (RE-AIM) framework to extract the details of the screening programs and categorize the contents of each article (Glasgow et al., 1999) was used. This framework combines five dimensions (i.e., reach: description of the target population; effectiveness: measurable impacts of interventions; adoption: qualitative and quantitative data for individual and organizational adaptation of interventions; implementation: the detailed strategy of interventions; and maintenance: the promoter and barrier of sustainable implementation of interventions) (Glasgow et al., 1999). RE-AIM framework was used as a guide to clarify and categorize the content of each article.
Reach
The number and age of the participants who underwent ultrasound screening were extracted. For municipality-led systems, if available, the number of eligible populations for municipality health checkups where DDH screening was conducted was extracted and the participation rate (i.e., screened participants/population) was calculated. Owing to the unknown number of targeted populations, these rates in giving-birth hospital settings were not calculated.
Effectiveness
Researchers extracted data on how many infants were detected as having abnormal hips at screening and how many infants received treatment after the examination. Then the prevalence of abnormal hips was calculated. The positive predictive value was calculated as the number of participants needing treatment divided by the number of referred participants.
Adoption
Researchers summarized the organizational factors that influenced the implementation of ultrasound screening, including the history of the screening system, occupation of providers, venue, cost, setting, and frequency.
Implementation
Researchers extracted a detailed strategy for performing ultrasonographic screening, including the notification process, equipment, time required, and referral for special examination.
Maintenance
Prompters or barriers to the sustainable implementation of ultrasound screening were identified. These items include the authors’ opinions.
The data was graphed using a Microsoft Excel extraction form. The members of the study team created and evaluated the data extraction form. All authors received the outcomes of the data extractions so they could discuss each manuscript's content and ensure its caliber.
Results
Initially, 61 articles were identified from Igaku Chuo Zasshi, 65 from MEDLINE, 22 from CHINAL, 0 from ERIC, and 0 from APA PsycInfo. Twenty articles were duplicates. Two manuscripts were retrieved from the reference lists of the included manuscripts. After reviewing 130 article abstracts, 63 of them were included in the full-text review. Ultimately, 18 articles were included in the analysis. The details are shown in Figure 1.
All identified articles were written in the Japanese language. To date, all existing research in the field has involved case-series studies whose aims were to explain natural trajectory following ultrasound screening for DDH. No randomized controlled studies have been conducted.
The number of infants included in the articles ranged from 145 to 58,995 (mean: 4,734.6, SD: 13,274.2, median: 1,098.5). Excluding articles that did not report results or only reported results using hips as the unit, the number of infants considered to have abnormal hips ranged from 20 to 2,102 (mean: 278.2, SD: 506.3, median: 152) and the number of infants treated ranged from 1 to 217 (mean: 37.8, SD: 69.6, median: 7). The details are shown in Table 2.
Pattern of Ultrasound Screening Systems in Japan
Universal ultrasound hip screening systems offered in Japan were categorized into two types: (1) completed as part of the public baby health checkup program run by the municipality (hereafter, municipality-led screening), and (2) performed on all newborns or infants who visited the giving-birth hospital where they were born, but not in the public health checkup program (hereafter referred to as hospital-led screening).
Five municipalities reported the implementation of a municipality-led screening system: Niigatashi-in Niigata (Hatakeyama & Takahashi, 2005; Takahashi et al., 2014), Gouzu-shi in Shimane (Hoshino, 2021; Hoshino & Nakadera, 2014), Nakajo-machi in Niigata (Minagawa et al., 2005), Shimosuwa-cho in Nagano (Asagai et al., 2005; Ishida & Yamamoto, 2009), and Sendai-shi in Miyagi (Ohashi, 2018). For hospital-led screening, five hospitals were reported in five municipalities (Aoki & Suetsuna, 2013; Aoki et al., 2011; Murakami et al., 2014; Ogawa et al., 2002; Shiraki et al., 2003; Watanabe, 2002; Yamada et al., 2016; Yamada et al., 2017).
The characteristics of each municipality, including those in this study, are listed in Table 1. Niigata-shi, Sendai-shi, and Nagoya-shi are ordinance-designated cities with large populations, and high-level health administration functions were transferred from the prefectural government.
Characteristics of the Municipalities that Implemented Ultrasound Screening for Developmental Dysplasia of the Hip Among Infants in Community Settings in the Articles Included in This Study.

Ministry of Internal Affairs and Communications stipulates an ordinance-designated city as a city with more than 500,000 people and a core city as a city with more than 200,000 people. It allows them to conduct certain tasks without the intervention and permission of the prefectural governors.
Adapted from “Surveys of Population, Population Change and the Number of Households based on the Basic Resident Registration (2022)” by Ministry of Internal Affairs and Communications (2022). retrieved from https://www.e-stat.go.jp/en/statistics/00200241.
Characteristics of Articles and the Results of Ultrasound Screening for Developmental Dysplasia of the Hip Among Infants in Community Settings Using the RE-AIM Framework.
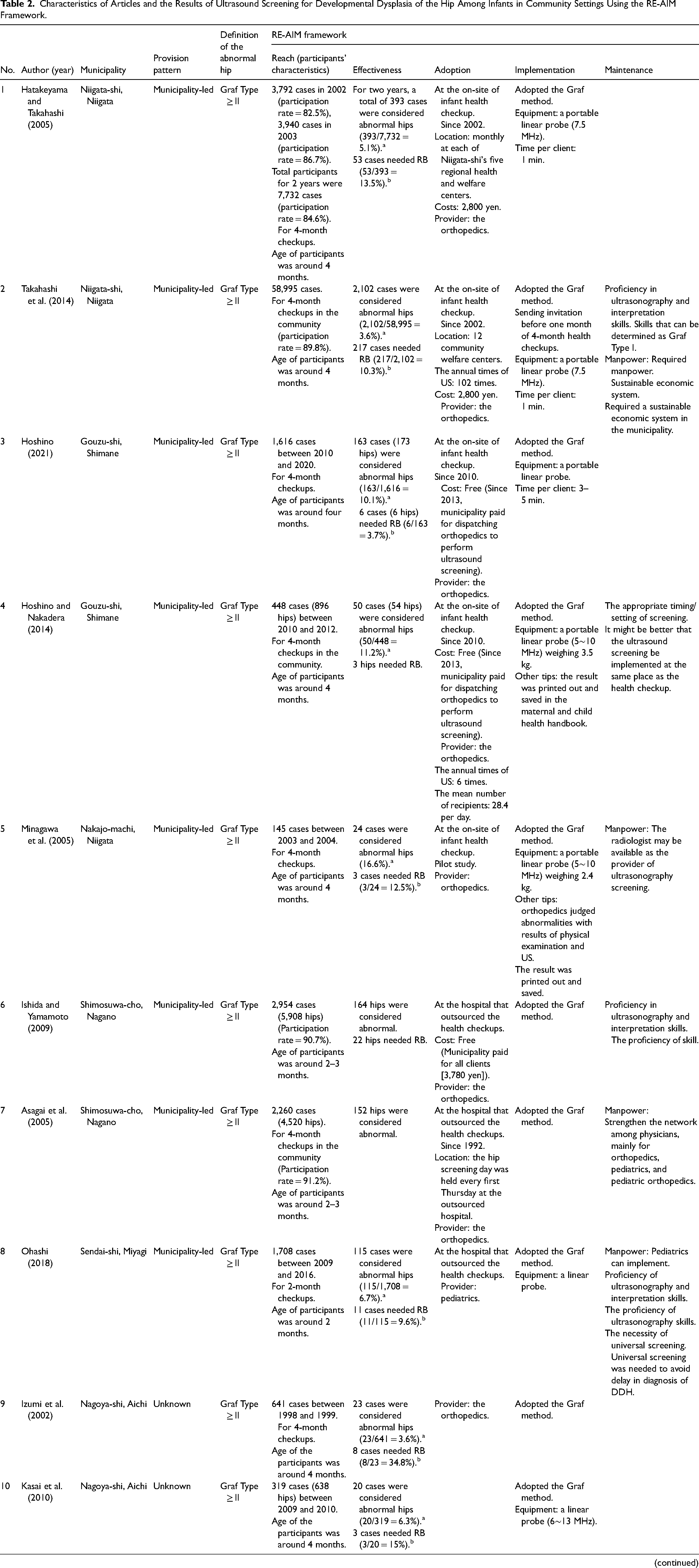
Note. All articles were case-series studies. DDH = developmental dysplasia of the hip; US = ultrasound screening for DDH; RB = Riemenbuegel brace; NICU = neonatal intensive care unit. Giving-birth hospital: all newborns who were born here. a Prevalence of abnormal hip (i.e., participants with abnormal hip/participants received ultrasound screening for DDH); b positive predictive value (i.e., participants needing treatment/referred participants).
Reach
Municipality-Led Screening
The participation rate in universal ultrasound screening for DDH was 84.6% (Hatakeyama & Takahashi, 2005) to 91.2% (Asagai et al., 2005) in municipality-led screening. Six municipalities performed universal ultrasound screening for infants’ hips at 2- or 4-month health checkups.
Hospital-Led Screening
Participation rates could not be calculated for hospital-led screening, which is an opportunistic screening in which persons who have visited a hospital are eligible for screening because the target population is unknown. Ultrasonographic screening was conducted for all newborns born at each hospital, and informed consent was obtained. Screening conducted on neonatal intensive care unit (NICU) newborns had almost 50% dropout owing to death, discharge, and transfer (Murakami et al., 2014). The mean age of the participants was 2.9 (Aoki et al., 2011) to 110 (Yamada et al., 2016) days.
Effectiveness
Municipality-Led Screening
The prevalence of abnormal hips, with cases referred to special examinations, ranged from 3.6% (Takahashi et al., 2014) to 16.6% (Minagawa et al., 2005). The positive predictive value ranged from 3.7% (Hoshino, 2021) to 13.5% (Hatakeyama & Takahashi, 2005), and the pooled mean was 10.4%. These percentages are based on cases (infants) as the unit of analysis and did not include articles that reported only the number of abnormalities or treatments using hips as the unit of analysis.
Hospital-Led Screening
The prevalence of abnormal hips ranged from 5.3% (Yamada et al., 2016) to 34.3% (Aoki et al., 2011). The positive predictive value was reported to be 0.7% in one study (Aoki et al., 2011). One study reported that although all abnormal hips recovered after 3 months, one normal hip was dislocated after a 1-month follow-up (Shiraki et al., 2003).
Adoption
Municipality-Led Screening
There are three subtypes of ultrasound screening for DDH. The details are shown in Figure 2. Municipality-led screening has two styles: on-site (Niigata-shi, Nakajo-machi, and Gouzu-shi) and outsourced to hospitals (Shimosuwa-cho and Sendai-shi). First, the municipality directly implemented ultrasound screening. In Niigata-shi and Gouzu-shi, ultrasound screenings were performed at the same location as the baby health checkups (Hatakeyama & Takahashi, 2005; Hoshino, 2021; Hoshino & Nakadera, 2014; Takahashi et al., 2014).

Administration styles of ultrasound screening for DDH.
Second, in Shimosuwa-cho, ultrasound screening was conducted at a hospital stipulated by the municipality (Asagai et al., 2005; Minagawa et al., 2005). The hospital outsourcing style was also adopted in Sendai-shi (Ohashi, 2018). In these two styles, ultrasound screening is embedded in the public health checkup program but is not directed by the municipality or provided to all infants in the municipality.
Shimosuwa-cho (Asagai et al., 2005; Ishida & Yamamoto, 2009) launched ultrasound screening in 1992. The town paid 3,780 yen to each client receiving ultrasound screening for DDH, and the parents bore no cost. The orthopedic routine included ultrasound screening for DDH for all 4-month-olds at the hospital.
Niigata-shi (Takahashi et al., 2014) launched ultrasound screening in 2002. Infants whose parents requested screening underwent ultrasound screening by an orthopedist at a 4-month checkup, with a payment of 2,800 yen. Four-month checkups were held at 12 city-health centers 102 times per year.
Gouzu-shi (Hoshino, 2021; Hoshino & Nakadera, 2014) launched ultrasound screening in 2010. The city had outsourced its ultrasound screening system. An orthopedic stay at the 4-month checkup site and on-site ultrasound screening was performed for those whose parents intended to receive screening. The annual number of screenings was six times, and the mean number of recipients was 28.4 per day.
Hospital-Led Screening
Hospital-led screening was conducted on infants born in hospitals in a giving-birth hospital-led style (Aoki & Suetsuna, 2013; Aoki et al., 2011; Murakami et al., 2014; Ogawa et al., 2002; Shiraki et al., 2003; Watanabe, 2002; Yamada et al., 2016; Yamada et al., 2017). The timing of ultrasonography ranged from birth to discharge (Aoki & Suetsuna, 2013; Aoki et al., 2011; Murakami et al., 2014; Shiraki et al., 2003; Watanabe, 2002) to approximately three months of age (Yamada et al., 2016). The screening program from birth to discharge included all infants for whom consent was obtained, and later, screening was offered to infants who had been discharged from the hospital and wished to participate.
Two articles reported on the cost of ultrasound screening for DDH. Payments for the screening tests ranged from free (Yamada et al., 2017) to 5,250 Japanese Yen (Shiraki et al., 2003).
Implementation
Municipality-Led Screening
In most of the studies, a linear probe was used with an output set between 5 and 13 MHz. Sixteen articles mentioned that the provider was a physician. The Graf method was adopted for the ultrasound screening of DDH in all articles. In all cases, hips other than those identified as Graf Type I were considered abnormal.
In Niigata-shi, the municipality sends an invitation for ultrasound screening for DDH to infants one month before the 4-month checkup. An orthopedist implemented a 1-min screening per infant, and all infants were referred for secondary screening, except for the exact Graf Type I (Hatakeyama & Takahashi, 2005; Takahashi et al., 2014).
In Gouzu-shi, an orthopedic program screened each infant for 3–5 min. The results were printed and saved in the Mother and Child Health Handbook (Hoshino, 2021).
Hospital-Led Screening
All articles reported linear probes, and the Graf method was used for screening. The outputs were 7.5 and 8 MHz. Regarding the criteria for hip abnormalities, only one article reported that from Graf Type Ia to IIb were normal hips, Graf Type IIc was borderline hips, and Graf Type ≥ III was abnormal hips (Shiraki et al., 2003). Others used the same criteria as municipality-led screenings.
Maintenance
In the dimension of maintenance, five categories emerged throughout the articles.
The Necessity of Proficiency in Ultrasound and Interpretation Skills
Takahashi et al. (2014) reported that screening for hip abnormalities took only one min per infant, and 3–5 min per infant was reported in another study (Hoshino, 2021). Training to improve ultrasonography skills was deemed necessary to expand ultrasound screening nationwide (Ishida & Yamamoto, 2009; Ohashi, 2018; Yamada et al., 2016). Aoki et al. (2011) suggested that skill proficiency may affect the rate of referrals for special examinations.
Human Resources
The lack of human resources preventing the expansion of ultrasound screening for DDH was reported in several articles. Minagawa et al. (2005) and Ohashi (2018) indicated that radiological technologists or pediatricians could perform ultrasound screening for DDH with training instead of orthopedists.
Sustainable Economic System
The cost of dispatching orthopedists and implementing ultrasound is a major issue (Takahashi et al., 2014).
Appropriate Timing/Setting of Screening
Several articles reported the appropriateness of the timing or setting of ultrasound screening for DDH. Hoshino and Nakadera (2014) suggested that it might be better to implement ultrasound screening in the same location as health checkups. According to Murakami et al. (2014), screening and follow-up in NICU had the benefit of allowing the provision of early guidance on daily care for infants. However, according to Ogawa et al. (2002), the 1-month checkup is the ideal time to avoid causing mothers undue stress.
Need for Universal Screening
All articles suggested that universal ultrasound screening was valuable in preventing a late diagnosis of DDH.
Discussion
Overview of the Results
To the best of our knowledge, this is the first literature review on universal ultrasound screening for DDH among infants in community settings in Japan. This review revealed the actual number of articles addressing ultrasound screening for DDH among infants in community settings. This study focuses on summarizing the clinical evidence regarding the universal ultrasound hip screening program in Japan. These findings may provide useful information for other countries wishing to promote community-based ultrasound DDH hip screening programs. The results showed two patterns of ultrasound screening—municipality-led and hospital-led—and the cost varied. The target population participated in screenings organized by municipalities at a rate of 85% or higher, showing that these screenings had a higher reach than those organized by hospitals. Each local government in Japan offers maternity and child health services, such as home visits for newborns and infant checks for illness screening and health advice (National Center for Child and Development, 2017; Osawa et al., 2019). Public baby health examinations are provided as part of a community-based healthcare system that is easily accessible and free for parents. The participation rate in 1–2-month and 3–5-month health checkups was approximately 90% (Ministry of Health, Labour and Welfare, 2021). Therefore, caregivers would have undergone municipal-led ultrasound screening with easy access and peace of mind. They would accept accurate ultrasound examinations without radiation exposure, despite the varying costs. These results also suggest that ultrasonography is still being used for universal screening in Japan. To promote health equity in each community, local governments require the development of an ultrasound screening system in collaboration with pediatric orthopedic surgeons.
The results showed that the positive predictive value ranged from 3.7% to 13.5% for municipality-led screenings, and it was 0.7% for hospital-led screenings. There is controversy regarding which screening method is best for preventing late diagnosis (Kuitunen et al. 2022). Previous studies reported that the positive predictive value of clinical screening was 5.4%, and ultrasonic screening 3.6%; meanwhile, it was 1.8% in Denmark (Husum et al. 2021), and that of community-based screening for infants under 15 months was 0.93% in Israel (Wilf-Miron et al., 2017). Although the current study revealed that the Japanese positive predictive value of universal ultrasonic screening was similar to other countries’ reports, the positive predictive value varied depending on each report. These findings suggest the need for adequate accuracy in the management of hip screening and enhancing clinical training for healthcare professionals.
Both screening methods had a different prevalence of abnormal hips referred for special examinations after the initial screening based on the Graf method. Physicians mainly conducted ultrasound screening, with only one article mentioning the possibility of radiologist screening (Minagawa et al., 2005). The timing of inspections has been controversial in previous studies (Agostiniani et al., 2020; Kilsdonk et al., 2021; Paton, 2017). The different ages at which the examinations were performed and the different ultrasonography examiners may have affected these results (Dezateux & Rosendahl, 2007; Hoshino & Nakadera, 2014). Additionally, the lack of personnel who can conduct ultrasound screening is a barrier to the development of an ultrasound screening system in the community (Ohashi, 2018; Takahashi et al., 2014; Yamada et al., 2016). A previous study showed that nurses could use ultrasonography images with an appropriate training program (Husum et al., 2022). In Japan, nurses are increasingly assessing each client's health condition using ultrasonography (Yamada et al., 2023; Yoshida et al., 2020). PHNs and MWs are crucial in providing maternal and childcare services in community settings (Osawa et al., 2019; Yoshioka-Maeda et al., 2023). Hence, further research focusing on educating nurses in ultrasonography is required, and training PHNs and MWs to use ultrasonography may enable DDH screening in community settings.
Most articles suggested that a universal screening system was needed to detect DDH at an early stage, despite the limited ultrasound skills and lack of human resources. Universal ultrasound screening is effective in the early detection of DDH, and there has been controversy regarding which method is suitable for preventing late diagnosis (Kuitunen et al., 2022). The referral rate would impact secondary hospital screenings; this is necessary for efficient and effective primary ultrasound screening systems in community settings.
Limitations
This study had several limitations. First, randomized controlled studies were not found to be included in this review. Owing to the limited evidence, careful interpretation of the results is needed. Second, only published studies were collected; undetected works and programs could also exist. Third, the implementation strategies of each local government were not identified. Despite these limitations, this is the first literature review of ultrasound screening for DDH among infants in Japan. Developing community-based healthcare systems to detect DDH cases early and providing educational programs for nurses to assess DDH cases using ultrasonography is necessary.
Implications for Practice
Although risk factors for DDH are well-known (Kuitunen et al., 2022; Shorter et al., 2013), nurses may not pay attention to this issue in community settings owing to limited cases of DDH. Therefore, educational programs should be developed for nurses who require improvement of their assessment skills and DDH knowledge. Additionally, local governments must develop an ultrasound hip screening system in each community to detect DDH cases at an early stage. To this end, collaborating with pediatric orthopedic surgeons, nurses, and infant caregivers would be crucial.
Conclusions
This review identified two types of ultrasound screening in Japan: municipality- and hospital-led. In municipality-led, the participation rate ranged from 84.6% to 91.2%. The Graf method was used mainly, and the positive predictive values of screening programs differed widely. A lack of personnel to conduct ultrasound screening hindered sustainable implementation. Training healthcare professionals would enhance universal ultrasound screening for the early detection of DDH cases in the community.
Footnotes
Acknowledgments
The authors would like to express their thanks to all members who supported conducting the current study.
Availability of Data and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
Conceptualization, A.I.-A., C.H., H.M., and K.Y.-M.; data curation, A.I.-A., C.H., H.M., and K.Y.-M.; formal analysis, A.I.-A., and H.M.; founding acquisition, K.Y.-M.; investigation, A.I.-A., C.H., and H.M.; methodology, A.I.-A., C.H., H.M., and K.Y.-M.; project administration, K.Y.-M.; resources, A.I.-A., C.H., and H.M.; software, H.M.; supervision, K.Y.-M.; validation, A.I.-A., C.H., H.M., and K.Y.-M.; visualization, A.I.-A., C.H., H.M., and K.Y.-M.; writing—original draft preparation, A.I.-A., C.H., H.M., and K.Y.-M.; writing—review and editing, A.I.-A., C.H., H.M., and K.Y.-M. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Neither research ethics approval nor informed consent were needed for the conduct of the current review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Culture, Sports, Science and Technology named “Research Data Ecosystem Development Project to Promote the Use of Artificial Intelligence” (to K.Y.-M.).