
Abstract
Introduction
The use of electrocardiograms (ECGs) is widespread among emergency room (ER) nurses for diagnosis and triage, making it crucial for them to have the appropriate level of competency in interpreting ECGs. This can lead to better healthcare and patient outcomes.
Objectives
This study aims to assess the competency level of emergency nurses in Palestine in interpreting normal ECG and certain cardiac arrhythmias, and to explore the association between socio-demographic characteristics and their ECG interpretation competency.
Methods
The study used a cross-sectional descriptive design, and 196 ER nurses were conveniently recruited to fill out a self-administered questionnaire based on previous literature. The data collected were analyzed using SPSS with strict adherence to ethical considerations.
Results
The results showed that 70.9% of the nurses were males, 65.3% held a bachelor's degree in nursing, 46.9% had 1–5 years of experience, and 60.7% had received previous courses on ECG interpretation. The mean competency level of the ER nurses was satisfactory at 60.714%, but 38.8% had a poor level of competency. This was significantly higher among nurses with higher educational levels (p-value < 0.001), those who had taken previous ECG courses (p-value = 0.045) and life support (p-value < 0.05), and those who were exposed to more ECG interpretations per day (p-value = 0.001).
Conclusion
There is a need to focus more on ECG competency levels in Palestinian literature and compare them between different departments. It is also essential to evaluate nurses’ needs for continuous education.
Introduction
The ECG is non-invasive cardiac test that reduces risks for patients with coronary artery disease by detecting cardiac problems and irregular rhythms. Nurses in critical care units are responsible for monitoring and interpreting ECGs (Nabil Malk et al., 2018). The ECG is crucial for diagnosing conditions like MI (Sridhar et al., 2021).
Nurses working in emergency rooms (ER) play a critical role in the timely diagnosis and treatment of patients presenting with cardiovascular emergencies. One of the most commonly used tools for this purpose is the electrocardiogram (ECG) (Shah & Algiraigri, 2021). ECG competency is important as it is also considered a crucial step in the primary care of ER patients (Malak et al., 2022; Rahimpour et al., 2021). In cardiac emergencies, nurses need to be proficient in interpreting ECGs due to their frontline positions and initial patient assessments (Alanezi, 2018). To ensure prompt interventions and life-saving measures in the event of dysrhythmias, emergency nurses must possess the knowledge and skills necessary to identify dangerous and life-threatening arrhythmias, and appropriately react to them (Kadush et al., 2023). However, interpreting an ECG accurately and promptly requires specialized knowledge and skill. Inadequate competency in ECG interpretation by ER nurses may lead to delayed diagnosis and inappropriate treatment, which can have serious consequences for patients (Faraji et al., 2019).
Review of Literature
Enhanced competency skills among emergency department personnel may increase patient safety by lowering the possibility of misinterpretation in situations involving life-threatening situations. (Salamehet al., 2023; Vand Tamadoni, 2020). The competency of nurses’ knowledge and skills regarding ECG and arrythmias interpretations has been observed by Several studies worldwide, such as in Saudi Arabia, Spain, Iraq, Iran, Ethiopia (Aljohani, 2022; Belay et al., 2023; Coll-Badell et al., 2017; Kadush et al., 2023; Mousa et al., 2016; Rahimpour et al., 2021).
In a recent study conducted in Iraq, it was found that 80% of nurses had poor knowledge regarding ECG interpretations (Kadush et al., 2023). Another study conducted in Iran revealed that ER nurses have a low competency level regarding ECG interpretations (Rahimpour et al., 2021). A similar low competency level was also noted in a study carried out in Addis Ababa Ethiopia, which revealed that 90.9% of ER nurses were not competent (Belay et al., 2023). However, a study conducted in Spain found out the ER nurses possess a high level of knowledge regarding ECG interpretations (Coll-Badell et al., 2017).
According to Antiperovitch et al. (2018), misinterpretation, misdiagnosis, and missing ECG patterns can lead to adverse outcomes. Emergency nurses play a critical role in assessing, evaluating, and managing patients with cardiovascular diseases in the emergency units. However, as reported by McGrath and Sampson (2018), nearly 30% of patients with myocardial infarction may be under-triaged, indicating inadequate competence in ECG interpretation among emergency nurses. Therefore, continuous training courses are urgently needed to enhance their competency, as highlighted by Haristiani and Tanrewali (2021).
This study holds significance because it evaluates Emergency nurse's competency in interpreting primary ECG parameters and life-threatening and non-life-threatening ECGs. This proficiency is critical in emergency situations and plays a crucial role in preventing future problems from a patient's pre-existing cardiac condition (Qaddumi et al., 2020). In Palestine, no prior studies have examined the competency level of ER nurses in basic and arrhythmias ECG interpretation with a specific focus on identifying the most important conditions.
By evaluating the current knowledge and competency of emergency nurses in interpreting ECG arrhythmias, recommendations can be established for healthcare administrators and policy makers. These recommendations can include providing focused ECG courses to improve the knowledge and competency level of nurses, which in turn can help reduce the morbidity and mortality associated with patients with ECG abnormalities. Therefore, the main objective of this study is to assess the competency level of emergency nurses in Palestine in interpreting normal ECG and certain cardiac arrhythmias, and to explore the association between socio-demographic characteristics and their ECG interpretation competency.
Research Question
What are the sociodemographic characteristics of nurses working in the emergency room?
What is the competency level of emergency nurses in Palestine in interpreting normal ECG and certain cardiac arrhythmias?
Is there a significant association between socio-demographic characteristics and their competency in ECG interpretation?
What are the predictors of competence among Emergency nurses?
Research Hypothesis
H0: There is no significant association between sociodemographic characteristics of nurses and their competency in ECG interpretation.
H1: There is a significant association between sociodemographic characteristics of nurses and their competency in ECG interpretation.
Method
The research used a quantitative cross-sectional descriptive design to determine the level of competency of emergency room (ER) nurses in Palestine regarding electrocardiogram (ECG) interpretation of normal ECG and cardiac arrhythmias.
Sample and Sampling Method
The study was conducted in emergency departments covering the north, middle, and south of Palestinian hospitals. The study population consisted of emergency nurses employed at Palestinian hospitals in the middle and northern regions of the West Bank. All registered nurses working in the emergency departments of these selected hospitals were invited to participate in the study, totaling 226 nurses. The final sample included all nurses who agreed to participate in the study and completed the study questionnaire, totaling 196 nurses, accounting for potential attrition rates and compensating for incomplete questionnaires. The response rate of 87% exceeded the minimum required sample size of 159 participants, which was calculated using G*Power software 3.1.9.7, with an effect size of 0.25, a power of 0.80, and a significant p-value of (0.05).
Inclusion and Exclusion Criteria
The inclusion criteria were full-time nurses with at least 6 months of experience, and incomplete questionnaires were excluded.
Instruments
The questionnaire used in the study was self-administered and had two sections. The first section included closed-ended questions about nurses’ demographic and professional information such as age, gender, education level, hospital type, district, experience in the emergency room, and previous courses in ECG, Basic Life Support (BLS), or Advanced Cardiac Life Support (ACLS), as well as the number of exposures to ECG per day.
The second section was adapted from a previous study by Coll-Badell et al. (2017) with permission and consisted of 12 multiple-choice questions, 2 theoretical and 10 clinical, designed to assess nurses’ competency in ECG interpretation. The questionnaire was edited to suit the study's objectives, resulting in a final version of 15 close-ended multiple-choice questions covering various arrhythmias and ECG interpretations, from basic to advanced levels. The competency score was calculated by adding up the correct answers and dividing them by 15, then multiplying by 100 to get a score out of 100%. The scores were classified into three levels: “Poor” for scores less than 60%, “Good” for scores between 60% and <80%, and “Excellent” for scores of 80% or higher, based on previous literature by Ruhwanya et al. (2018).
For the validity, the questionnaire was adopted from a previous study, and then modified to include questions that cover other areas of interventions related to arrhythmias. Also, the questionnaire was reviewed by 5 experts related to the topic of the study, including 2 specialist doctors and 3 expert nurses in the field of emergency nursing and ECG interpretation, who gave a positive feedback regarding the consistency and clearance of the questions. Two expert nurses suggested the addition of questions related to management of asystole cases, and an ECG figure related to pericarditis and hyperkalemia.
Before the final data collection, the questionnaire was disseminated to 10% of the recommended sample size (15 nurses), who were working in the targeted hospitals, and were asked to give feedback about the consistency and build of the questionnaire, especially in terms of it coverage to different areas of ECG interpretation. Replies were taken in consideration, and mostly focused on the clearance of ECG figures, as well as the addition of receiving courses specific to ECG interpretation, rather than focusing on BLS and ACLS. The questionnaires that were filled in the pilot period were excluded from the final analysis.
Ethical Consideration
Ethical approval was obtained from the health research ethics committee of the Arab American University (AAUP), and from hospital administrators where the study was conducted.
A consent form was obtained from nurses. The research study objectives and its significance were explained and clarified. Enough time was given to consent, and all information remained confidential (by giving the questionnaires serial numbers rather than names) to maintain anonymity of the participants. The nurse received a written declaration in the informed consent (and verified verbally) that the collected data are kept secret and were used by the researcher only and for the purposes of research, with the right to withdraw from the participation at any time without the need to declare any reason.
Data Analysis
For the purpose of data analysis, IBM Statistical Package for Social Sciences (SPSS) software v25.0 was used to produce descriptive and analytical results regarding the nurses’ data. Descriptive statistics include the observation of frequencies and percentages of nurses’ demographic data and their responses to the questions of the ECG interpretation, and the mean and standard deviation (SD) of the overall level of competency about ECG interpretation.
As the data are not normally distributed, non-parametric analytical tests were used, while the type of analytical results was based on the types of variables, therefore, Mann-Whitney U test was used to investigate the relationship between dichotomous independent variables (nurses’ gender, hospital type, and whether the nurse received a course or not) and the level of competency in replacement to independent sample t-test, while Kruskal-Wallis was used to investigate the relationship between non-dichotomous independent variables (age as a categorical variable, educational level, district, experience in ER and number of ECG interpretations per day) and the level of competency in replacement to one-way analysis of variance (ANOVA), and Spearmen Correlation test was used to investigate the correlation between nurses’ age (as a scale variable) and their competency in replacement to Pearson Correlation test. The value of 0.05 was considered for the significance level (p-value) for these relationships.
Results
Nurses’ Sociodemographic Data
Table 1 distributes the sociodemographic data of the nurses who were enrolled in the current study (n = 196), and shows that most of the nurses (60.2%) are between 20 and 29 years old, with a mean age of 29.12 ± 5.67 years old, ranging from 20 to 50 years old, while another one third of the nurses (33.2%) are between 30 and 39 years old, with around three fourths of them (70.9%) are male nurses, compared to only 29.1% female nurses in emergency rooms (ER).
Distribution of Nurses’ Sociodemographic Data in Frequencies and Percentages or Means.
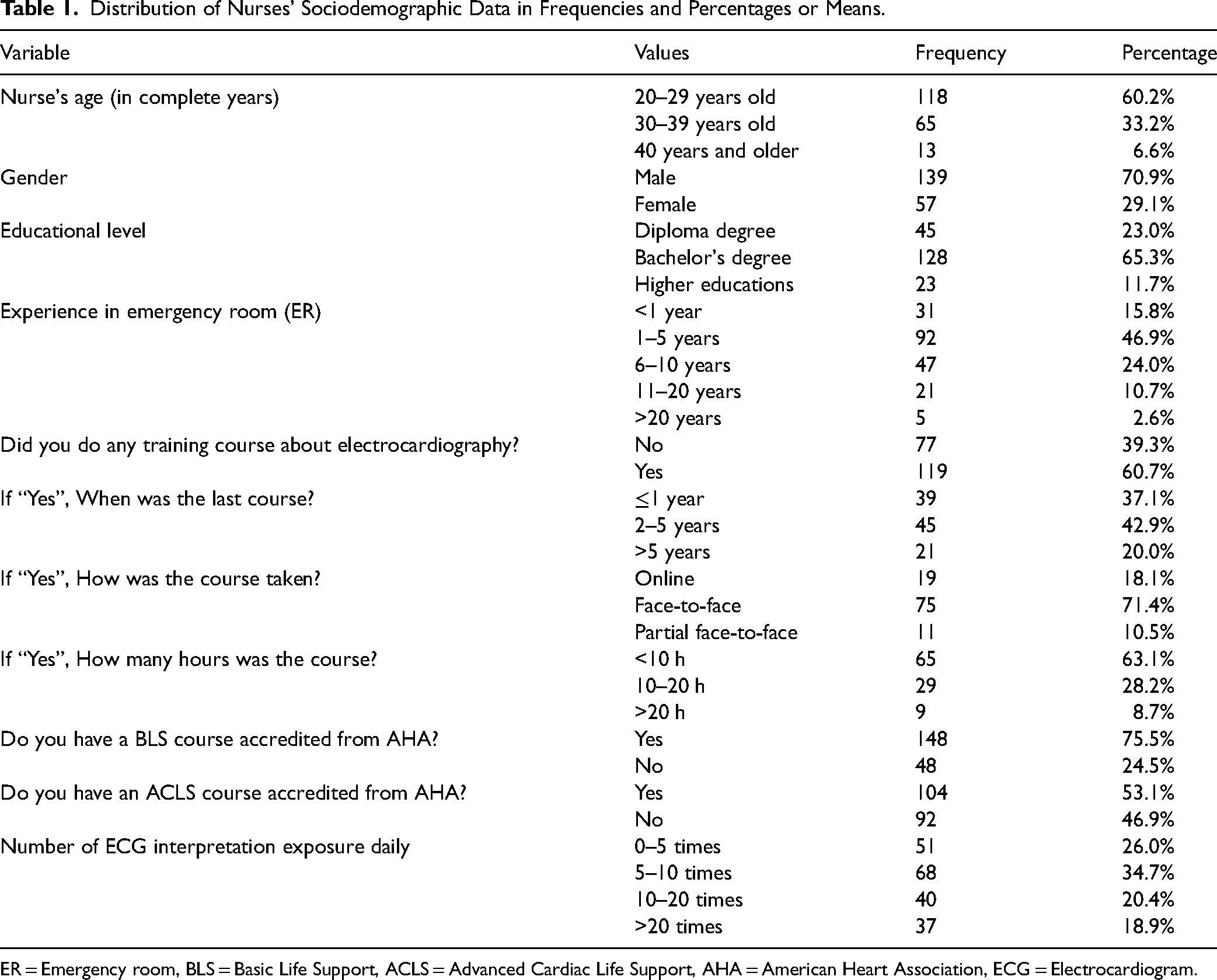
ER = Emergency room, BLS = Basic Life Support, ACLS = Advanced Cardiac Life Support, AHA = American Heart Association, ECG = Electrocardiogram.
The table also shows that around two thirds of the nurses (65.3%) have bachelor's degree in nursing, compared to around one fourth of them (23.0%) who have diploma degree, and only 11.7% who have master's degree in emergency or other nursing specialty.
In general, less than half of the nurses (46.9%) have experience between 1 and 5 years in ER, compared to 15.8% with less than one year of experience and 24% with an experience between 6 and 10 years. Moreover, 60.7% of the nurses stated they have received a training course about electrocardiography (ECG). Of them, 42.9% stated the last course was taken within the last 2 to 5 years, 71.4% took it face-to-face, and 63.1% had it for less than 10 h. Lastly, more than three fourths of the nurses (75.5%) in ER stated they received a BLS course accredited from the American Heart Association (AHA), compared to almost half of them (53.1%) who received an ACLS course accredited from AHA, with around one third of them (34.7%) stated they are exposed to 5 to 10 ECG interpretations per day, compared to 26% who are exposed to 0 to 5 ECG interpretations per day. The following figures illustrate the distribution of ER nurses’ sociodemographic data.
Level of Competency About ECG Interpretation among ER Nurses
Figure 1 distributes the frequencies of the correct answers for each of the 15 questions in the level of competency section regarding ECG interpretation. The mean number of correct answers among the sampled ER nurses was 9.107 ± 3.537 out of 15, which indicated that the mean level of competency among the ER nurses about ECG interpretation is 60.714%, which is fairly a split above the satisfying level of competency (above 60%), ranging from zero to 15 correct answers.
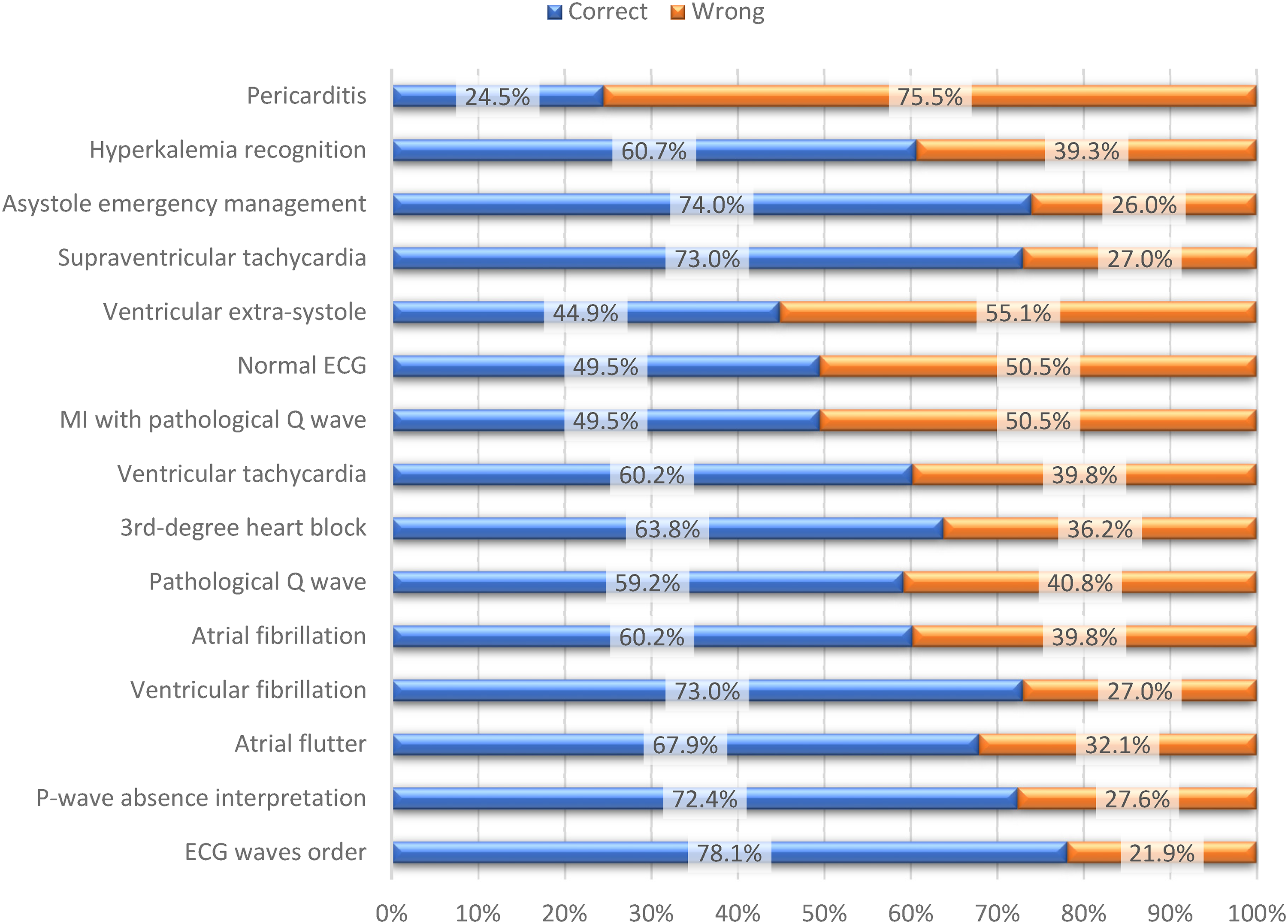
Distribution of the correct and wrong answers for each question.
Table 2 distributes the frequencies and percentages of the satisfactory competency level among the ER nurses regarding ECG interpretation. The table shows that there is an approximate distribution among levels of satisfaction regarding competency about ECG interpretation, where 38.8% of the nurses had poor, 29.6% had acceptable and 31.6% had excellent levels of competency satisfactory.
Distribution of Level of Competency Satisfactory Levels among ER Nurses Regarding ECG Interpretation.

The Relationship Between ER Nurses’ Sociodemographic Factors and Their Level of Competency
Table 3 shows the results regarding the relationship between ER nurses’ sociodemographic factors and their level of competency. It shows that older nurses have higher level of competency (mean = 10.3 for 40 years and older compared to 9.15 for 20–29 years old), but in an insignificant way (p-value = 0.554), and the same is found in the Spearman Correlation test, which gave a weak result of 0.075 (p-value = 0.326), with male nurses (mean = 9.26) had insignificantly higher level of competency than female nurses (mean = 8.72, p-value = 0.392).
Differences in Mean Score of Competency (out of 15) About ECG Interpretation According to ER Nurses’ Sociodemographic Data.

Significance marked as *p-value < 0.05, **p-value < 0.01, ***p-value < 0.001. Test values are for Mann-Whitney U test for mean differences according to gender, hospital type, receiving ECG training, receiving BLS or ACLS, while for Kruskal-Wallis for differences in mean according to age group, educational level, district, ER experience, ECG course details and exposure.
On the other hand, educational level of the nurse was significantly correlated with his/her level of competency regarding ECG interpretation, with higher level of competency with higher education (mean = 11.39) compared to bachelor's (mean = 9.63) and diploma (mean = 6.47) degrees (p-value < 0.001). The more experienced ER nurses had higher mean competency scores, but insignificantly.
As expected, receiving courses related to ECG interpretation was significantly correlated with higher level of competency (p-value = 0.045), and while the period since the last course was not significantly correlated with the level of competency (p-value = 0.657), results showed that nurses who received the ECG interpretation courses via face-to-face method (mean = 10.43) were significantly more competent than who received it partially face-to-face (mean = 8.73) or via online method (mean = 7.58, p-value = 0.014). Also, nurses who received the courses for more than 20 h had significantly higher level of competency (mean = 11.67, p-value < 0.001).
Moreover, ER nurses who received BLS and ACLS courses had significantly higher competency level (mean = 9.58 and 9.68, respectively) than those who did not (mean = 7.64 and 8.45, respectively), which are accredited by AHA (p-value = 0.003 and 0.016, respectively). Finally, ER nurses who are exposed to more ECG interpretation times in their duty are more competent (p-value = 0.001).
Predictors of Competency Level among ER Nurses
To determine the predictors of the competency level among the ER nurses, a linear regression was conducted between significantly associated demographic factors and the competency level, as shown in Table 4. It shows that the nurse's educational level is considered a significant positive predictor (p-value < 0.001), where each level increased in nurse's education (e.g., from bachelor's to higher education) is predicted to increase level of competency by 2.615 out of 15 (95% CI = 1.834–3.396). Also, receiving a course in ECG interpretation was positively predicted to increase the competency level by 1.053 out of 15 (95% CI = 0.041–2.066, p-value = 0.041), although both course type and hours of ECG were not predictors for competency level (p-value = 0.103 and 0.252, respectively).
Predictors of Competency Level among ER Nurses.

Significance marked as *p-value < 0.05, **p-value < 0.01, ***p-value < 0.001. CI = Confidence interval.
On the other hand, receiving accredited courses from AHA (BLS and ACLS) were significantly predicted to increase competency level by 1.935 (95% CI = 0.806–3.064, p-value = 0.001) and 1.226 (95% CI = 0.240–2.212, p-value = 0.015) out of 15, respectively. Lastly, more exposure to ECG interpretations per day was also a significant positive predictor (p-value < 0.001), where an increase of exposures by 5 times per day (each categorized level of exposure) is predicted to increase competency level by 0.842 out of 15 (95% CI = 0.385–1.300).
Discussion
The present study aimed to assess the competency level of emergency nurses in Palestine in interpreting normal ECG and certain cardiac arrhythmias among 196 emergency room nurses.
The review by Haristiani and Tanrewali (2021) and the current study both found that the competency level of emergency room (ER) nurses in interpreting electrocardiograms (ECGs) varied depending on factors such as their educational level, experience, and exposure to ECG interpretation. In contrast, a study conducted in Saudi Arabia found out no significant relationship between age, educational level, experience, and the competency of ECG interpretations (Aljohani, 2022). Similarly, Coll-Badell et al. (2017) found no significant relation between nurse's experience and ECG interpretations.
The study by Aljohani (2022) also investigated the order in which nurses correctly identified different ECG arrhythmias. The study found that the order of correct identification differed from that in the current study. However, both studies found that nurses’ competency in ECG interpretation was higher among those with higher educational levels and those who had taken courses, rather than being solely dependent on experience.
In our study, the majority of emergency nurses successfully identified conditions such as Asystole, SVT, ECG wave order. However, they encountered challenges when interpreting ECG changes associated with conditions like Pericarditis, Extrasystole and MI with pathological Q wave. A study carried out in Iraq revealed that nearly all CCU, ICU, and ED nurses could accurately respond to all knowledge-based questions, except for those concerning changes in ECG for both new and old myocardial infarction (Al-Husaunawy, 2015). Moreover, a recent study conducted in Iraq found that the majority of nurse possess poor knowledge regarding ECG interpretation (Kadush et al., 2023). This underscore the need for additional effort on the practical application, requiring more advanced instruction and training (Tahboub & Yılmaz, 2019).
The current study found a lower mean score for ECG interpretation compared to the previous study conducted by Coll-Badell et al. (2017). Both studies found a positive relationship between taking previous ECG courses and level of competency. Furthermore, the competency levels observed in the Turkish study align closely with those in the current study (Tahboub & Yılmaz, 2019).
The present study aimed to investigate the predictors of competency level among ER nurses in ECG interpretation. The results of the study showed that educational level, receiving ECG training course, receiving BLS course, receiving ACLS course, and ECG exposure significantly predicted competency level among ER nurses in ECG interpretation. These findings are consistent with previous literature. Several studies have reported that education and training are essential factors in improving competency levels among nurses in ECG interpretation (Al-Turaiki et al., 2017; Kashou et al., 2020; Najafi Ghezeljeh et al., 2019). Additionally, studies have shown that exposure to ECGs and experience in interpreting them play a significant role in improving competency levels (Al-Turaiki et al., 2017; Chen et al., 2022; Kashou et al., 2020; Najafi Ghezeljeh et al., 2019).
The present study also found that the type of ECG course and ECG course hours did not significantly predict competency levels among ER nurses in ECG interpretation. However, previous studies have reported conflicting results regarding the effect of ECG course type and duration on competency levels (Al-Turaiki et al., 2017; Chen et al., 2022; Kashou et al., 2020; Najafi Ghezeljeh et al., 2019).
Furthermore, longer courses and specific types of ECG courses, such as advanced ECG courses, can improve competency levels (Kashou et al., 2020).
Recommendations and Implications for Practice
Overall, the present study provides further evidence supporting the importance of education, training, and experience in improving competency levels among ER nurses in ECG interpretation. The findings of this study can be used to develop targeted educational programs that address the identified predictors and improve competency levels among ER nurses in ECG interpretation.Additionally, decision-makers should acknowledge the importance of ongoing assessments of emergency nurses’ skill levels, encouraging ongoing improvement in their clinical competency for ECG interpretation.
Conclusion
The results indicated a mean competency slightly above the satisfactory threshold of 60%. Notably, variations were observed in competency levels across different ECG interpretations, with the highest competency level identified in sinus rhythm and the lowest in atrial fibrillation. While gender, and age showed trends toward greater competency scores, these relationships were not statistically significant. Conversely, educational level, experience, receiving ECG training, more exposure to ECG interpretations, and receiving accredited courses from AHA (BLS and ACLS) were found to be significant predictors of higher competency levels. The result revealed a diverse distribution of competency satisfactory levels, where 38.8% of the nurses had poor, 29.6% had acceptable and 31.6% had excellent competency levels. These findings, highlights the importance of assessing the competency levels before starting educational sessions, adopting different teaching techniques, and ongoing monitoring of the effects of new technologies in the teaching process. Finally, the study recommends the need for continuous education efforts and the recruitment of enough sample size to such comparative quantitative studies. Overall, the findings of this study can contribute to the improvement of emergency department nursing practice and the enhancement of patient outcomes.
Limitations
The self-reported survey, which considered as a limitation, primarily centered on the cognitive aspects of cardiovascular crises and ECGs. Notably, the authors did not assess psychomotor or skills competencies, such as the ability to participate in code blue or megacode, put the defibrillator pads correctly, choose the appropriate Joule, or administer shocks. Furthermore, the study employed parametric analysis. Therefore, its recommended that future studies consider employing parametric sampling technique, such as simple random sampling, systematic sampling, or stratified sampling.
Footnotes
Acknowledgment
We extend our heartfelt gratitude to all the nurses who participated in this study.
Authorship Statement
All authors listed meet the authorship criteria and all authors are in agreement with the content of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Ethical approval was obtained from the Arab American University and from the Palestinian Ministry of Health (MOH) to conduct the study in the Palestinian hospitals. Also, approved by the Helsinki committee number is PHRC/HC/1063/22.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.