
Abstract
Background
COVID-19 was devastating for many frontline nurses embroiled in health care's response. Most media outlets reported from several large metropolitan areas in New York, California, and Florida, leaving other regions to wonder about the extent to which their nurses were suffering.
Objective
The purpose of this article was to understand the specific needs and experiences of Northeast Ohio nurses caring for patients with COVID-19 before designing interventions targeting negative mental outcomes.
Methods
This phenomenological study interviewed 16 Northeast Ohio nurses to understand their experiences of caring for patients with COVID-19.
Results
Although not asked about it directly, the participants’ stories consistently included details that could be linked to moral distress. Two themes describing their lived experiences included “acquiring moral distress” and “living with moral distress.” Additional findings are also reported separately because although they do not represent the lived experience of COVID-19 nursing, they did represent significant concerns that participants had for the future and are reported here to assist other researchers with the intervention design. Furthermore, these participants thought that participation in support groups with other nurses who cared for COVID-19 patients and possibly led by mental health advanced practice nurses offered the best intervention to process their trauma from the pandemic.
Conclusions
The long-term effects of moral distress have been discussed routinely in recent literature and are further complicated by the effects of the COVID-19 pandemic. Threats to the shrinking workforce of nurses must be taken seriously and interventions to improve the mental health and morale of frontline nurses must be prioritized and tested.
Nurses caring for patients during the COVID-19 pandemic were deeply affected by its impact both on the job and at home. Recognizing the heroic acts performed daily by health professionals caring for COVID-19 patients, Dr Amy Acton, director of the Ohio Department of Health, stated in a daily news conference that “Not all heroes wear capes.” This catchphrase quickly went viral and subsequent conversations with nurses showed that the phrase inadvertently added pressure to the already struggling nursing workforce to keep going at all costs (personal communications). As the pandemic wore on and nursing burnout increased, nurses continued to vacillate between feeling the self-protective need to leave direct patient care, which had become increasingly dangerous, or to continue heroic acts of patient care for those who needed them, events which Schwartz (2022) claims elevated the significance of “moral injury” to the American lexicon (Aloweni et al., 2002; American Nurses Foundation, 2022).
Nursing leaders quickly recognized that the COVID-19 pandemic would have long-lasting impacts on the profession by further eroding a workforce already coping with staffing shortages, mental health strain, and morale (Lopez et al., 2021). But while most media outlets reported about the effects of COVID-19 on nurses from large metropolitan areas in New York, California, and Florida, it is also important to understand regional or institutional differences in how nurses experienced the pandemic before designing interventions aimed at lessening its effects. This study will examine the specific needs and experiences of Northeast Ohio nurses caring for patients with COVID-19.
Moral Distress and Injury
Moral distress occurs when individuals cannot follow through with what they believe is right because of organizational or institutional constraints. Morally distressing events include unethical practices or violations of an individual's moral code (American Association of Critical Care Nurses, n.d.). Moral injury occurs after one or more exposures to morally harmful events occur, leading to deeper psychological or existential wounds (British Medical Association, 2021; UKCEN: et al., n.d.). Symptoms of moral distress and injury are reported similarly across research and include psychoemotional, spiritual, and physical symptoms (Table 1).
Moral Distress/Injury Symptoms.
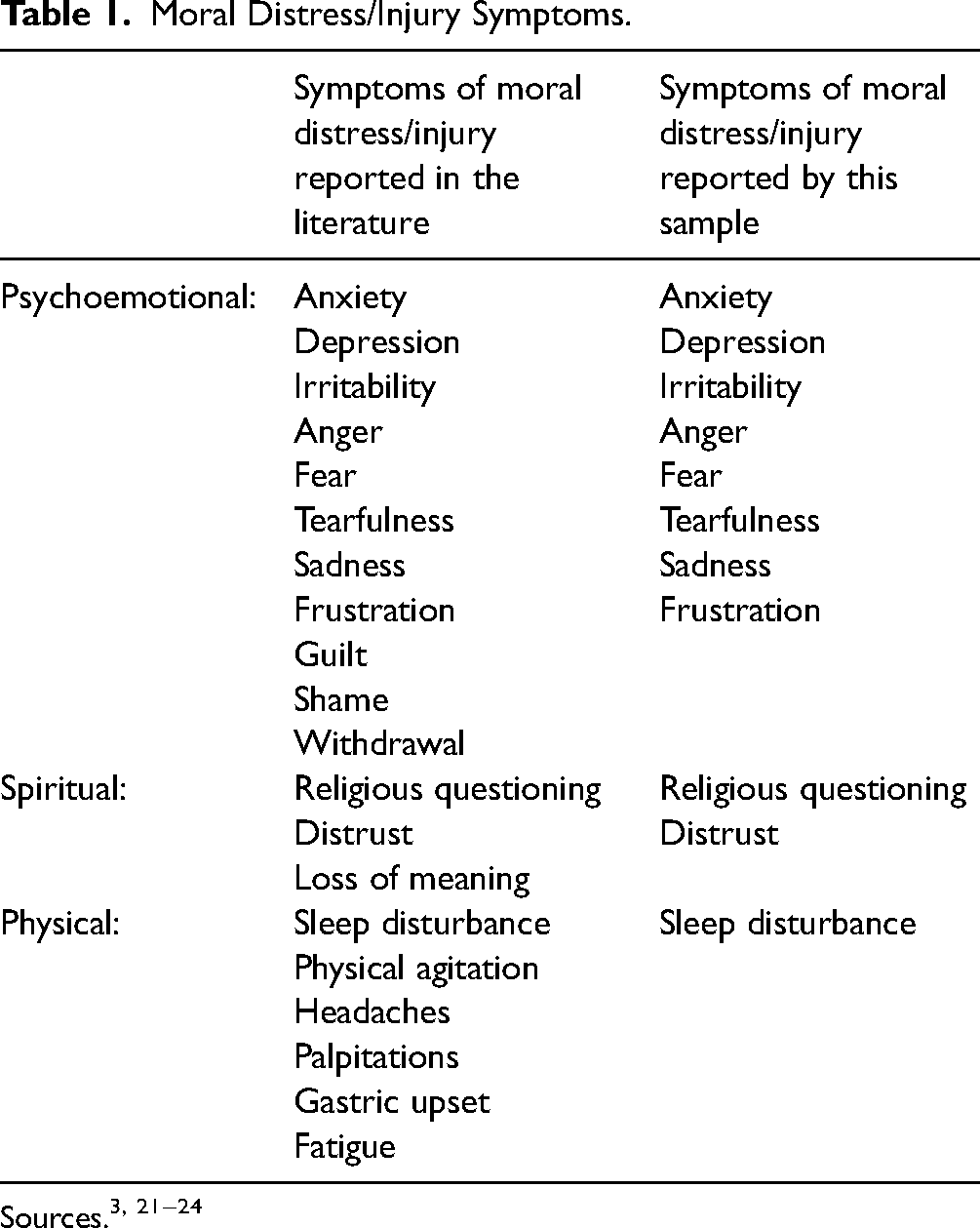
Sources.3, 21−24
Moral distress and injury originated in military science with mixed opinions as to whether the caliber of injuries required to cause moral injury was transferable to nursing. Specifically, opinions differed about whether unethical nursing situations paralleled the brutality of war. With the onset of the COVID-19 pandemic, however, comparisons between hospitals and “war zones” became more prevalent, accelerating the application of moral injury principles to nursing situations (American Association of Critical Care Nurses, n.d.; White, 2021).
Method
This study used interpretive phenomenological analysis (IPA) outlined by Smith et al. (2009) to understand the experiences of nurses caring for COVID-19 patients in Northeast Ohio. IPA seeks to understand the everyday lived experiences of a phenomenon, but with particular interest in those experiences that participants are more than simply aware of, but live with intensity. This was an important distinction for this sample because COVID-19 was not just a work phenomenon. Rather, the nurses lived with COVID-19 around the clock and with little relief from its impact, making IPA an acceptable methodology for this project.
Permission to conduct this research was obtained from the authors’ Institutional Review Board. After providing written informed consent, 16 nurses who met the eligibility criteria for caring for COVID-19 patients were recruited from Northeast Ohio hospitals using purposive and snowballing strategies (Smith et al., 2009). Study flyers that explained the study purpose and eligibility criteria, as well as providing investigators’ contact information were distributed to professional colleagues. Those colleagues were asked to share flyers with other colleagues. Interested nurses were screened for eligibility and scheduled for interviews.
Semistructured, open-ended interviews were conducted with participants and lasted from 45 to 60 min. Broad questions such as “tell me about your nursing unit” were used to begin the interviews. Other interview questions are provided in Table 2. Due to in-person restrictions associated with the pandemic, the authors conducted interviews via telephone. Face-to-face interviews are often preferred but telephone interviews have also been reported as an accurate and valid method of data collection (Drabble et al., 2016; Saarijärvi & Bratt, 2021). Interviews were digitally recorded, transcribed verbatim, and quality-checked by the interviewer.
Interview Guide.

According to methods outlined by Smith et al. (2009), transcripts were read and independently coded by each investigator, who are also the authors of this study. The investigators met several times to discuss their interpretation of the data by closely following six steps outlined by Smith et al. (2009): reading and rereading, initial noting, developing emergent themes, searching for connections between themes, moving to the next case, and looking for across cases patterns. Disagreements in coding were resolved by consensus between the two investigators. Study rigor was maintained for trustworthiness using prolonged immersion in the data, peer debriefing between investigators, and maintenance of audit trails (Lincoln & Guba, 1985).
Results
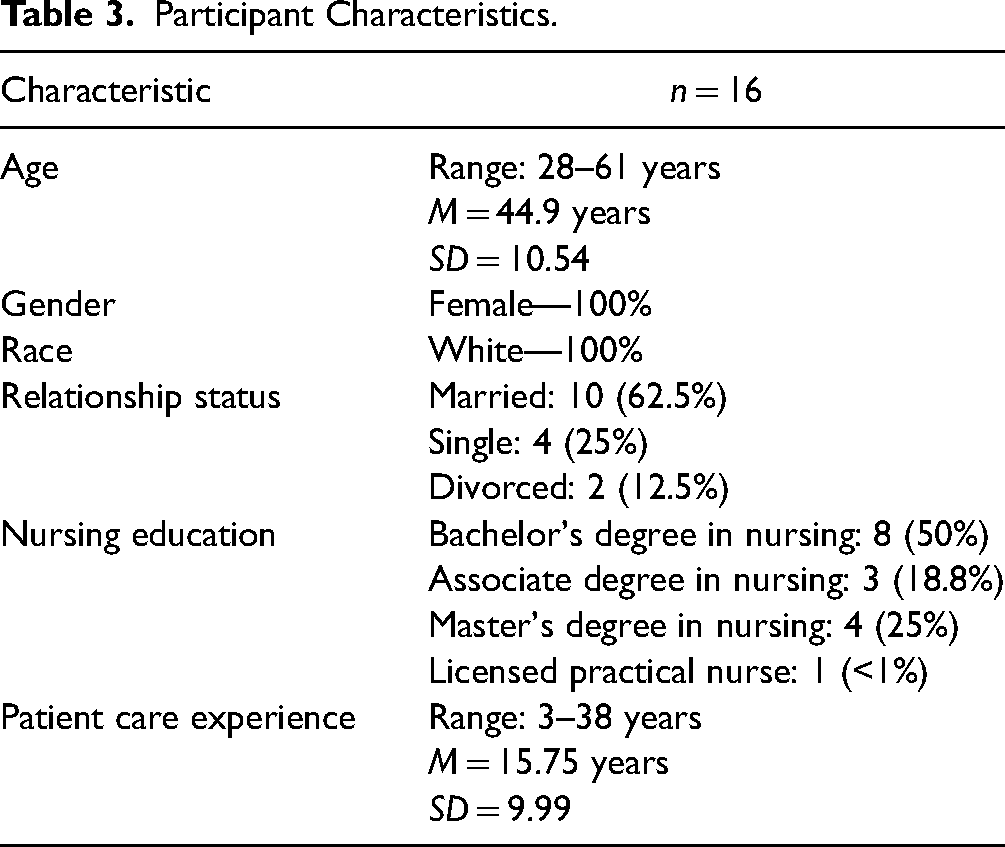
The sample consisted of White females with an average age of 44.9 years (Table 3). All participants had a bachelor's degree in nursing except for two participants with associate degrees. One nurse was only a few weeks from completing her master's degree in nursing. Clinical nursing experience ranged from three to 38 years. Two themes emerged from the data that described participants’ experience of caring for patients with COVID-19. Acquiring moral distress outlined the sources of moral distress and how it affected patient care. Living with moral distress described the symptoms and sequelae participants lived with around the clock and throughout the duration of the pandemic (Table 4).
Participant Characteristics.
Moral Distress Themes.

Acquiring Moral Distress
Participants described several occurrences that created moral distress for them. The sources of moral distress included, (a) patients forced to die alone, (b) families prohibited from visiting patients, (c) improper withdrawal of life support, and (d) the futility of patient care.
Caring for patients who died alone because nurses could not get to them in time was highly distressing for participants. Several factors contributed to the likelihood that patients would die alone, including how quickly patients declined, the need to keep patients in isolation (private rooms and behind closed doors), and the amount of time it took nurses to dress in isolation gear before entering the room. A telemetry nurse caring for COVID-19 patients explained how hard it was to monitor patients who had to remain behind closed doors due to isolation. She explained, “you walk in the door and these patients are fine. And then 30 min later you're having to code them.” A medical-surgical (med-surg) nurse corroborated that she felt “like a hawk sitting on a wire. You’re watching these people … waiting to see who was gonna be next.” Another telemetry nurse elaborated on the frequency with which this occurred: You hear the nurses screaming outside the doors saying, ‘Okay take a deep breath you've got to take a deep breath.’ That was like our mantra. You could just walk down the hall and hear the nurses telling the patients, ‘You need to take a deep breath.’
Not being able to reach patients in time so they did not die alone was against participants’ nursing values and contributed to moral strain. A critical care nurse explained, “As a nurse, the last thing you ever want is a patient who is dying to be by themselves and to die by themselves. I’ve had more patients die by themselves … and it is just awful.” In most pre-COVID-19 situations, family members were at the bedside when a patient died. While participants understood the reasons for prohibiting visitors, the inability of hospital leaders to find alternative solutions so patients were not alone interfered with basic nursing principles of presence and advocacy. One med-surg nurse commented: I’m definitely smart enough to understand why they (the family) can’t be there, but I still think it's awful …. But you’re also telling me that we don’t have the staff … or ‘sorry, you (the nurse) don’t have the time’ to sit there either … I didn’t sign up for that and that is not OK! You’re never gonna tell me that's OK. We don’t want them to be in their room all by themselves when they take their last breath, so you’re watching and waiting for that pulse ox to start dropping so you can gown up and get into that room while there is still time so you can at least talk to them while they take their last breath.
As new policy mandates prohibited family members from visiting, nurses on the front lines were often the ones explaining visitation restrictions and besieged by desperate family members begging for one last chance to see their loved one, which several nurses described as “awful.” Nurses’ own life experiences often overlap with these family tragedies. For example, a med/surg nurse explained why it was important for her to help family members say goodbye. Despite having a full load of COVID-19 patients, several of whom were seriously ill, she described helping a mother and daughter say goodbye before the mother died: I might cry with this story, but I had a lady they were terminally weaning from oxygen and there were no visitors allowed. The lady was unresponsive, so I just held the phone while her daughter talked to her as the lady passed away. For me personally, that was probably my hardest day.
She recalled her father's passing a few months earlier, noting that it was not, “COVID-related but he lived in Florida, and I couldn’t be with him. So, I felt like I wasn’t able to be with him but I’m able to be with someone else's family member.”
Another source of moral distress was orders to wean patients from oxygen too quickly, which conflicted with their ethical duty to provide patient comfort. One med-surg nurse reported: There have been a few patients who were made DNRs, and the doctors would write orders to ‘turn the oxygen down.’ And I was always taught that oxygen was a comfort measure. … I always left the oxygen to the point that the patient had easy breathing.
The final source of moral distress among participants was the futility they felt because they did not know how to treat COVID-19 in the early days when so many patients were dying. This was described by a float nurse who was often pulled to work on a COVID-19 unit: It feels traumatizing. As fast as I watch them roll in with COVID, I watch them roll right back out but in a body bag …. I never thought I’d see anything like this in my nursing career, but it was defeating. You’re working so hard and you’re so exhausted and they’re dying anyway. It felt very powerless, very helpless.
A sense of futility also occurred when patients refused treatment because they minimized the severity of the disease, as reported by the same float nurse: It was hard. It was so frustrating. Because it's like we’re there to take care of the patients and all of the sudden you're in this weird political war like is this virus real, and is this really what they have, and whether or not the government was really giving it to them? After a while I just had to ask people to keep their opinions to themselves because I'm here to take care of you. I don't really want to talk about what you think is going on. Because I'm here sacrificing my life every day taking care of you.
One med-surg nurse explained how similar denials led to hostilities between nurses with opposing views: We had a coworker who doesn't believe in the vaccine and she's not afraid to tell everybody that we're all dumb for taking the vaccine—those of us who did. Well, she said that we're all just guinea pigs and the government is just using us, and it's just a way to get money from people and things like that. Just little snide comments.
Living With Moral Distress
Exposure to sources of moral distress created moral distress symptoms for these participants. Eight symptoms were identified in this research, including psychoemotional (i.e., anger, irritability, anxiety, depression, fear), spiritual (i.e., questioning beliefs, mistrust), and physical (i.e., insomnia) symptoms. Living with moral distress was selected as the title of this theme because participants were not able to leave the sources of distress at work. The pervasiveness of COVID-19 threatened the participant's families at home, leaving few opportunities to escape the ordeal.
Anger and irritability were the psychoemotional symptoms described most often by participants. A med-surg nurse explained, “You could tell nurses are getting angry at each other. Aids are getting angry with the nurses. And everybody's blaming the manager (laughs).” Participants who said things like “normally I’m a laid-back person …” were finding themselves more “irritable,” “short-fused,” or easily “pushed over the edge.”
Anxiety and depression were common among participants. In the early days of the pandemic, anxiety stemmed from not being allowed to wear personal protective equipment at work. A critical care nurse explained: We had people at the hospital who were like, ‘I have grandchildren who are immunosuppressed, and I take care of them,’ or ‘I'm immunosuppressed!’ or ‘I have a mother who's on chemo and I need to protect her.’ And it wasn't even like they wanted an N95 mask. They just wanted to wear a regular surgical mask or any kind of mask. And they were getting written up because they (managers) said it was inciting fear…. I just couldn’t breathe. I couldn’t breathe. I was crying and I remember one of my friends there saying, ‘It's OK, it's OK’…. I had anxiety and I’ve never had an anxiety reaction before in my life. I thought I was gonna throw up. I had my head between my knees. One of the doctors was saying, ‘It's OK, take a deep breath. We’ll get through this.’ I said I don’t know if I could do this again. I can’t hold people's hands when they’re dying. I can’t zip up those body bags….
The number of participants who became tearful during their interview suggested the possibility of depression resulting from the pandemic. One critical care nurse remarked, “I've had periods of time where it was rough. Where I would come home and I'd cry in the car every day on the way home, for several weeks.” Fear of the unknown was an indicator of moral distress symptoms, especially in the early days of the pandemic when fear led one med-surg nurse to take extreme measures to manage the source of their fear: In the beginning, it was so unknown so like we did strip our clothes off in the garage …. Yeah, I feared getting it, fear of contracting it, fear of giving it to somebody else. Just fear of the unknown. Because we didn't know what was going to happen!
There were also spiritual indicators of moral distress in participants’ stories that included questioning their current beliefs and mistrust of others. A telemetry nurse said that spirituality was “something that I continue to struggle with” as she tried to make sense of the pandemic. “To think that things like this can happen is mind-boggling because there's no reason. You don't know ‘why?’ And these people who are so sick. And that's the frustrating thing is that there are no answers.” In other cases, participants said they lost trust in others because of an “every man for himself” attitude that came from “a lot of employees being at odds with each other” and managers failing to deal with it. Perceived lack of administrative support that nurses felt (e.g., “I just don't think that our input is very important to them.”) made them feel “expendable,” and “not very important.” One med-surg nurse reported: I know that they (the hospital board) had stuff they were dealing with too hospital CEOs and everybody … but I do know they got vaccinated first. And that was upsetting. I'm not happy with it. It's just been rough. I don't know maybe after a few years, I'll have a fresher perspective but for now I apologize but I'm just still very salty about it.
Although only mentioned by one participant, insomnia may also be associated with the COVID-19 pandemic. Inability to sleep was described by a med-surg nurse who said, “… probably if I had to bet, the day that that happened (moral distress event), I probably didn't sleep well. I would say in the last couple or three weeks I probably had 2 or 3 days that I didn't sleep well, and I maybe could correlate that to work.”
Additional Results Beyond the Lived Experience
Though not directly associated with the phenomenological themes of this study, each participant also shared their concerns about the future and asked for interventions that they thought would mitigate their distress. This information is presented as additional results because they were very important to the participants themselves as well as to the development of future surveillance and intervention research.
Concerns for the Future—Evidence of Moral Injury
If events leading to moral distress are persistent, they can reach the level of moral injury, which has significant existential consequences for the person experiencing multiple moral assaults (British Medical Association, 2021). Several participants expressed concerns about the long-term consequence of COVID-19 on themselves and other nurses that included descriptions of posttraumatic stress disorder (PTSD), demoralization, and paralyzing self-doubt. These outcomes could rise to the level of moral injury for some nurses.
Some participants were comfortable labeling what they saw within themselves and among coworkers as PTSD while others struggled to discern if their experiences were equivalent to those in combat settings. One telemetry nurse stated, “Yeah, there's a couple that I actually think they’re in PTSD and I know on stressful days it kind of all floods back.” A med-surg nurse expressed her concern about coworkers, noting: … the nurses are starting to feel different now. It's almost like posttraumatic stress if that makes any sense. You think this has got to get better (work stress from the pandemic), but then it doesn't. We've kept a lot of people alive, been figuring out a lot of things, but it still sucks. There's so many aspects that people don't think about, like having to call the family who can't visit and having to tell them that they passed. Having to be on the phone with families and having to talk with them and never having the right answer. There were some very vivid conversations and a couple that really stick out in my mind. A daughter saying “Am I doing the right thing? Am I doing the right thing by letting her go?” Those are awful conversations to have. And I guess that kind of stress and anxiety for a year, how could it not affect someone?
Conversely, another critical care nurse offered the unique perspective that symptoms of PTSD for nurses on her unit predated the pandemic: I think the baseline on our units, we have a lot (PTSD symptoms) of that just from coding patients one after another. So, I think the PTSD is kind of already there— even before COVID. But I can definitely understand how other nursing units felt that way.
Some participants were hesitant to use the term PTSD for nurses’ experiences during the pandemic, as expressed by one telemetry nurse who said, “posttraumatic stress means that you're being raped or being in war.” Several nurses thought that symptoms they experienced or observed in others were “similar to that (PTSD),” because it “is definitely something that's going to affect me for the rest of my life” but that the phenomenon “need[s] a different term.” A med-surg nurse explained: Some of the nurses say they’re angry and they can’t get over their anger. I know I’m emotionally different—I’m not the same. I don’t want to call it PTSD … we need a different term for nursing. I mean we are not seeing awful things like the soldiers in war so there needs to be a new term to describe what we’re going through.
Many participants described feelings of incompetence because they did not understand new policy changes, (e.g., “Why you’re seeing the best with proning, or with this drug. I want to know … because I want to know that I’m doing the best I can for this patient.”), new drug regimens (e.g., “I had to call pharmacy and ask ‘Can I hang this drug with this drug’ ‘Well, we don’t know.’”), or could not answer families’ questions (e.g., “We had patients and families having to sign things [consent forms]—like, ‘are you willing to try this?”). At times, nurses felt “powerless and helpless,” exemplified by a med-surg nurse who explained: I used to find fulfillment in my work. But during this pandemic, it was really hard to find that. I mean I knew that I was helping those who were alone and doing the best that I could, but it was just so hard. It was hard.
Closely related to feelings of demoralization was self-doubt. Some of the nurses were reduced to second-guessing themselves and their ability to do the work. A critical care nurse explained, “It's not easy going in and not having a firm answer for a patient who's already scared about what is happening.” In those types of situations, a critical care nurse said she could not help but wonder “when am I gonna get outta here (patient's room)” because not having answers was so uncomfortable. Repeated interactions such as these, which she equated with not being able to properly care for her patients, contributed to feelings of moral distress. She noted, “Let me tell you how bad I wanted to turn around. I did not sign up for this and could I take this home to my family! Is it really worth all of that?” The same nurse described what it was like at the start of her shift early in the pandemic. She said, “I remember the first time coming out onto the floor I’m like ‘OK, you’re gonna, you have this (COVID) patient….’ It was one of those moments of like, ‘What kind of nurse am I? Am I gonna turn back and go into the break room?’” Or in other words, did she have what it took to care for this patient.
Suggested Interventions
Several participants said they thought talking with other nurses would help them cope with their stressors. The idea of nurses helping nurses stemmed from their experiences that talking with family was not always helpful because they could not understand what the nurses were going through. Support groups were most often described as the preferred way of giving and receiving emotional support by this sample. A med-surg nurse reported that the nurses on her floor “try to talk between shifts” but there is not much time. She added, “We need somebody to listen to us, and we need somebody to talk to. I think having a group of people all going through it together would be helpful.” Another med-surg nurse specifically suggested a “psychiatric mental health nurse practitioner to come in here and help us.” Although one participant voiced this suggestion to a hospital administrator, she said, “he just looked at me in shock and didn’t even respond really.”
Discussion
This study sought to understand how nurses from Northeast Ohio experienced caring for COVID-19 patients. Findings identified several aspects of moral distress, including how moral distress was acquired and lived with throughout the pandemic. Sources of moral distress from these findings are well-supported by previous research reporting individual, relational, organizational, and systematic sources of distress (Silverman et al., 2021; Splig et al., 2022). Furthermore, witnessing patients dying alone, preventing families from being with patients when they died, engaging in improper nursing requests, and experiencing nursing care futility were identified in other studies (Donkers et al., 2021; Kellogg et al., 2021; Lake et al., 2022; White, 2021). Previous research reporting nursing care futility primarily addressed treatment futility or delivery of substandard health care due to various constraints in the early days of the pandemic and a lack of knowledge about COVID-19 (Netters et al., 2021). Findings from this study further identified nursing care futility among participants who cared for patients in denial that COVID-19 was a legitimate concern. Nursing care futility stemming from denial was problematic because it contributed to mounting frustrations and anger that nurses experienced while caring for COVID-19 patients despite risks to the nurses themselves and their families.
Spirituality is associated with resilience, making it important to understand the relationships between spirituality, resilience, moral distress, and COVID-19 nursing (Roberto et al., 2020). Consistent with previous reports, the symptoms participants described related to moral distress were psychoemotional, spiritual, and physical (Silverman et al., 2021). However, spiritual components of moral distress are rarely discussed or have been merged with psychological sequelae (Sarro et al., 2022). Beliefs and important relationships with self, others, and the transcendent (e.g., God, Allah, etc.) are central dimensions of spirituality (Stephenson & Berry, 2015). Participants in this sample struggled to find meaning during the pandemic and subsequently questioned their religious or spiritual beliefs. Relationships with important others (i.e., spiritual relationships) were also jeopardized, either due to family vulnerabilities from illness or strain with coworkers and institutional leaders. Other investigators report that a sense of teamwork can offer support, improve resilience, and contribute to less moral distress for nurses (Silverman et al., 2021; Splig et al., 2022). However, this study showed that teamwork was often compromised in nursing units treating COVID-19 patients, thus jeopardizing the supportive bonds that many nurses share with coworkers and contributing to loss of support, spiritual distress, and nurse suffering.
Prolonged and repeated exposure to moral distress events may lead to moral injury, a condition with greater existential threats to victims (Griffin et al., 2019; Young et al., 2020). Several participants believed they saw evidence of serious mental health conditions such as PTSD and demoralization within themselves and among others, underscoring the need to continue to monitor the long-term effects of COVID-19 on healthcare providers.
Limitations to this study include a lack of diversity among the all-White and female sample. Future research on racial, ethnic, and gender diversity is needed. The small sample size limits the generalizability of this study; however, since the aim of this research was to understand the needs of nurses caring for patients with COVID-19 in Northeast Ohio before designing local interventions, this study served its purpose and data saturation was reached. Finally, public policies for social distancing during the COVID-19 pandemic required that telephone interviews be used to interview participants. Using telephone interviews has limitations such as the inability to monitor nonverbal cues, assure that participants have privacy during sensitive questioning, and establish rapport. However, having the ability to conduct interviews by telephone rather than driving across the state to reach remote participants was also advantageous by conserving time and traveling expenses (Drabble et al., 2016; Saarijärvi & Bratt, 2021).
Conclusion
In addition to previous studies, findings from this research reveal that the ongoing and unpredictable nature of the COVID-19 pandemic has severely compromised the nursing workforce although the extent of its impact will not be fully realized for many years to come. Study participants expressed genuine concern about their own futures in nursing and those of their coworkers due to what investigators categorized as moral distress and/or injury. This concern, coupled with an already existing nursing shortage, makes it imperative that academic and healthcare institutions, scientists, and professional organizations continue to monitor and support nurses experiencing moral distress and/or injury and related sequelae.
Implications
These research findings have implications toward helping nurses heal in the aftermath of the COVID-19 pandemic. Findings support the incidence of moral distress for this sample who also had real concerns of larger consequences, such as PTSD. These participants also described their preferences for follow-up care that centered around talk therapy and support groups. This is important information to have so that interventions to assist nurses still coping with the pandemic are based directly on their needs. If nurses continue to work under the duress of the pandemic, for which they feel traumatized and undervalued, they will be at a higher risk for burnout, compassion fatigue, and early separation from the workforce. All of which seriously jeopardizes the stability of the nursing profession and patient care outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Delta Xi Chapter of Sigma Theta Tau International.