
Abstract
Introduction
Differences in availability and choices of contraceptive methods among postpartum women have been found to influence their quality of life as the fertility rate is very high, and the contraceptive usage rate persistently remains low in Nigeria.
Objectives
This study assessed the determinants of contraceptive options among postpartum women in Nigeria.
Methods
Two Local Governments were randomly selected from the four Local Governments. Within these two local governments, five health facilities were selected. A multistage sampling technique was used to select the 240 respondents, while a structured questionnaire was used to collect data.
Results
Findings from the study indicated that 81.7% of the respondents have planned to have their current baby, and about 65.4% of the women have resumed sexual activities since delivery. Of those who have resumed sexual activities, the majority, 91.1% did so 6 weeks after delivery. Some form of contraceptive usage was prominent among 59.2% of the respondents, as the most common contraceptive method used was withdrawal (24.8%). Contraceptive prevalence was slightly lower for urban respondents than rural respondents, although the relationship was not significant. Also, there was a statistically significant relationship between the current use of contraceptives and resumption of sexual activities since delivery (p = .001), resumption of menstruation (p = .001), and information received about postpartum family planning (p = 0.013).
Conclusion
Findings from this study emphasize the urgent need for enhanced accessibility and availability of contraceptive methods, with a parallel emphasis on targeted interventions and effective communication strategies to promote contraceptive uptake and family planning. Addressing these determinants is vital in improving postpartum women's overall quality of life in the study area.
Introduction
Globally, more than 90 percent of women during the first year of the postpartum period desire to either delay or avoid future pregnancies (Ross & Winfrey, 2019). Thus, during postpartum family planning (PPFP), mothers are counseled after delivery and encouraged to initiate a modern contraceptive method within the specified period. In most cases, sexual activities in the postpartum are resumed before the first menstruation following delivery without the use of any contraceptive method, even though this has not been proven to be safe according to research (Ndugwa et al., 2020).
In sub-Saharan Africa, postpartum women account for approximately 33 percent of sub-Saharan Africa's population of 973.4 million (Kyilleh et al., 2018). The proportion of postpartum women who are exposed to the risk of pregnancy by having sex without any contraceptive method within 2 years after childbirth is nearly one-third of the population (Ndugwa et al., 2020). The increasing number of postpartum pregnancies and abortions in Sub-Saharan Africa indicates that the continent's efforts to prevent this scourge have been insufficient (Tchokossa & Adeyemi, 2018). Numerous postpartum women are sexually active despite having limited knowledge of contraceptive options, which has increased the rate of unintended pregnancies, maternal morbidity, and mortality (Ashebir & Tadesse, 2020). The percentage of the population using PPFP varied among the various countries: 40% in Zambia, 25% in Kenya, 20% in Tanzania, 15% in Nigeria, and less than 10% in Ethiopia (Gebreselassie et al., 2008).
Literature Review
PPFP is the use of contraceptive methods in the first 12 months following childbirth to prevent unintended and closely spaced pregnancies (WHO, 2018). The risks of maternal and child morbidity and mortality are very high when pregnancy occurs within short intervals after childbirth (Van Soest & Saha, 2018). PPFP is essential for improving maternal and child health outcomes, as it can help to reduce the risk of maternal mortality, morbidity, and malnutrition, as well as the risk of preterm birth and low birth weight. However, PPFP utilization in Nigeria is relatively low yet fertility rate is high, with only 27% of postpartum women using contraceptives (Solanke, 2017). This is lower than the global average of 41%. Consequently, women in Nigeria are exposed to the dangers of unwanted and unplanned pregnancies postpartum. Across the various states in the country, the demand for PPFP is lower compared to the availability of the family planning services.
Many postpartum women in Nigeria are not aware of the different contraceptive methods available or do not have the knowledge to choose the right method for them (Alspaugh et al., 2019). On the other hand, contraceptive services are not always readily available or accessible to postpartum women in Nigeria, especially in rural areas. Also, the cost of contraception can be a barrier for some postpartum women in Nigeria. Furthermore, some socio-cultural factors, such as religious objections to contraception or gender inequality, can also prevent postpartum women from using contraception (Mahande et al., 2020).
Tayo et al. (2019) conducted a survey on contraceptive awareness and use among postpartum women in Lagos, Nigeria, and discovered that 5% of postpartum women with contraceptive sensitization were users. Educational programs and campaigns can be used to raise awareness and knowledge about contraceptive methods among postpartum women and their partners. Making contraception more affordable, integrating PPFP services into routine postpartum care or providing mobile contraceptive services, and addressing socio-cultural barriers could help in improving PPFP in Nigeria.
Given the critical importance of PPFP in addressing the unmet needs of women during the postpartum period and reducing the risks associated with unintended pregnancies, understanding the determinants of contraceptive choices among postpartum women is paramount. This study is particularly relevant in Nigeria, where fertility rates are high, but contraceptive use remains low, posing significant health challenges. The identification of factors influencing contraceptive options among postpartum women can inform targeted interventions to bridge the gap between demand and access, ultimately reducing maternal and child health risks in the country.
The primary objectives of this study are to assess the current utilization of contraceptives among postpartum women, identify their preferred contraceptive methods, examine the range of contraceptive options they adopt, investigate the reproductive factors that influence their contraceptive choices, and analyze the health system factors that impact these choices. Through these objectives, the study seeks to provide a holistic understanding of the determinants of contraceptive options among postpartum women in Osun State, Nigeria, with the ultimate goal of informing targeted interventions to improve PPFP services and enhance maternal and child health outcomes in the region.
While previous research has shed light on the challenges of PPFP in low-resource settings, this study focuses specifically on Osun State, Nigeria, providing region-specific insights into contraceptive determinants among postpartum women. By examining current contraceptive usage, preferred methods, and the influence of reproductive factors and health system dynamics, this study contributes to the existing body of knowledge on PPFP, offering context-specific solutions to enhance maternal and child health outcomes.
Methods
Design
A descriptive cross-sectional survey was used. The study was carried out in the Postnatal and Infant Welfare Clinic, Obafemi Awolowo University Teaching Hospital Complex (O.A.U.T.H.C), Ife Hospital unit (Urban Comprehensive Health Centre, Eleyele), Comprehensive Health Centre (Arubiewe), Primary Health Centre (Odowara), Primary Health Centre (Ondo Road), and Primary Health Centre (Iloro).
Research Questions
What is the current contraceptive usage among postpartum women?
What are preferred contraceptive methods used among postpartum women?
What are the factors influencing contraceptive use among postpartum women?
Sample
The target population of this study consists of postpartum women attending selected health care facilities in Ile-Ife. The determination of the sample size for this study followed Fisher's formula, which considers several crucial factors. The prevalence of the attribute being studied was estimated at 0.16. Additionally, a non-response rate of 10% was considered. To calculate the sample size, we employed various variables such as the standard normal deviation corresponding to the 95% coefficient interval (equivalent to 1.96), and the complement of the prevalence of the studied attribute. The margin of error, or the desired level of precision, was set at 5% (0.05).
With a total population of postpartum women of 245, we calculated the minimum required sample size to be 207 using the formula. However, to account for potential lost questionnaires, non-responses, and non-returns of filled questionnaires, an additional 10% of the sample size was added as a precaution. This resulted in an expected total sample size of 227.7, which was then rounded to a final sample size of 228 for the study.
A multistage sampling technique was used to select the respondents. This is when large clusters of population are divided into smaller clusters in several stages to make primary data collection more manageable. Out of the four (4) existing LGAs in Ife, two were selected, Ife Central and Ife East. In Ife Central: Obafemi Awolowo University Teaching Hospital (Urban Comprehensive Health Centre, Eleyele), Community Health Centre, Arubiewe. In Ife East: Primary Health Centre, Odowara, Primary Health Centre, Iloro, Primary Health Centre, Ondo Road. Proportionate allocation to size was done to select the appropriate number of subjects from the sub-populations for the study.
Inclusion Criteria
The inclusion criteria were: (a) postpartum women who had delivered within the last six weeks and (b) postpartum women who were willing to participate in the research study.
Exclusion Criteria
Postpartum women who did not speak and understand English or Yoruba and postpartum women who were not willing to participate.
Study Instrument
An adapted semi-structured questionnaire (Solomon et al., 2019) was used to elicit information from the respondents. This questionnaire was well-suited for the research objectives and consisted of four sections, aligning with the specific goals of the study. To ensure the quality and appropriateness of the questionnaire, it underwent a rigorous validation process. Copies of the questionnaire were distributed to both the study supervisor and experts in nursing research. These experts reviewed the questionnaire for its face and content validity, ensuring that it effectively captured the information needed for the study's objectives and that the questions were clear and relevant.
The reliability of the questionnaire was determined through the test–retest method. To carry out this assessment, a subgroup of 20 respondents from Ife central local government, who were not part of the main study, were selected. These respondents completed the questionnaire, and their responses were collected. After a specific period, likely designed to minimize recall bias, the same respondents were approached again to complete the same questionnaire for a second time. The data collected from the 20 respondents in the test–retest process was analyzed. This analysis aimed to assess the consistency of responses between the initial and subsequent questionnaire completions. A reliability coefficient was calculated to quantify this consistency. In this case, the reliability coefficient was determined to be 0.78, indicating a satisfactory level of reliability for the instrument.
With the validated and reliable questionnaire in hand, the primary data collection phase commenced. The study participants, postpartum women, were approached, and the questionnaire was administered. The respondents were selected from the study area in accordance with the research's inclusion criteria. By following these systematic steps, the research team ensured that the data collected using the adapted semi-structured questionnaire was of high quality in terms of its validity and reliability. This robust data collection process was crucial for the study to yield accurate and meaningful results in addressing the research objectives.
Statistical Analysis
The data collected was examined for completeness, coded, and entered using Statistical Product and Service Solution (SPSS) version 26. The data was then analyzed using both descriptive and inferential statistics. Descriptive statistics such as frequencies, percentages, mean, and standard deviation were used. Inferential statistics was done using chi-square linear regression to test the hypotheses generated, and the level of significance was set at 5% (0.05). Results were presented in tables and figures.
Results
Sample Characteristics
Table 1 shows the socio-demographic data of the respondents. Most women were between the ages of 25 and 34, and age 35 and over account for 20.8%. In terms of marital status, the majority of the respondents (98.8%) were married. Slightly over half (56.7%) reside in urban regions, and 54.2% have a secondary education or higher. Regarding employment, the majority (76.3%) were self-employed. In terms of family structure, the majority (88.8%) of the respondents identify as monogamous. Also, most of the population (81.7%) have planned to have their current baby.
Socio-demographic Characteristics of Respondents.
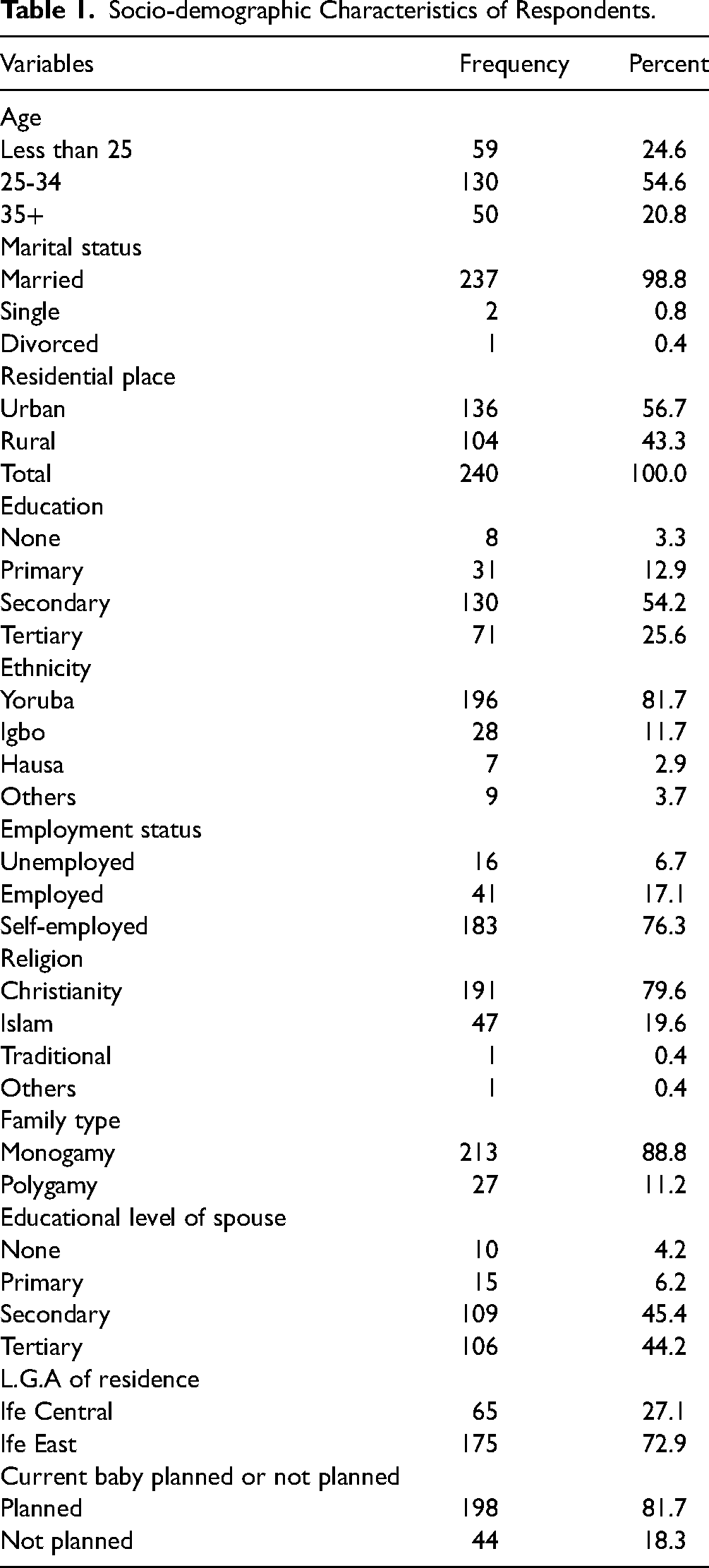
Table 2 provides information on contraceptive use among women who have given birth. Over half (65.4%) of the respondents have resumed sexual activities since delivery; of those who have resumed sexual activities, the majority (91.1%) did so 6 weeks after delivery. Over half (67.5%) of the women have used contraceptives previously following childbirth, and 59.2% of the women are using some form of contraceptive. Withdrawal is the most common contraceptive use (24.8%) as the most common reason for using contraception is to prevent unwanted pregnancy (73.2%). Most women (62.7%) obtain their contraceptives from hospitals, as most of the respondents (91.6%) know their current contraceptive method choice. A high proportion of respondents (85.2%) report that their partner is aware of their contraceptive choice. Most of the respondents (76.8%) intend to use contraception in the future, and 81.7% are satisfied with their current contraceptive method.
Contraceptive Information and Current Use.

Figure 1 shows the pie chart of the percentage of respondents who reported current contraceptive use by the sources of contraceptives. The majority of the respondents accessed their method choice from hospitals (42.4%), health centers (31.5%), and pharmacies/chemists (18.5%). Fewer respondents had their source of contraceptive from the private clinic (3.3%) and health post (4.3%).

Distribution of respondents by sources of contraceptives.
Figure 2 shows the results of the percentage of postpartum mothers who have knowledge of the current method choice and their assessment of the method. Among those who had knowledge of the current method choice, 62.4% rated the method as good. Among those who had no knowledge of the method, 2.1% assessed the method as good, and most of them assessed it as poor (5.7%).
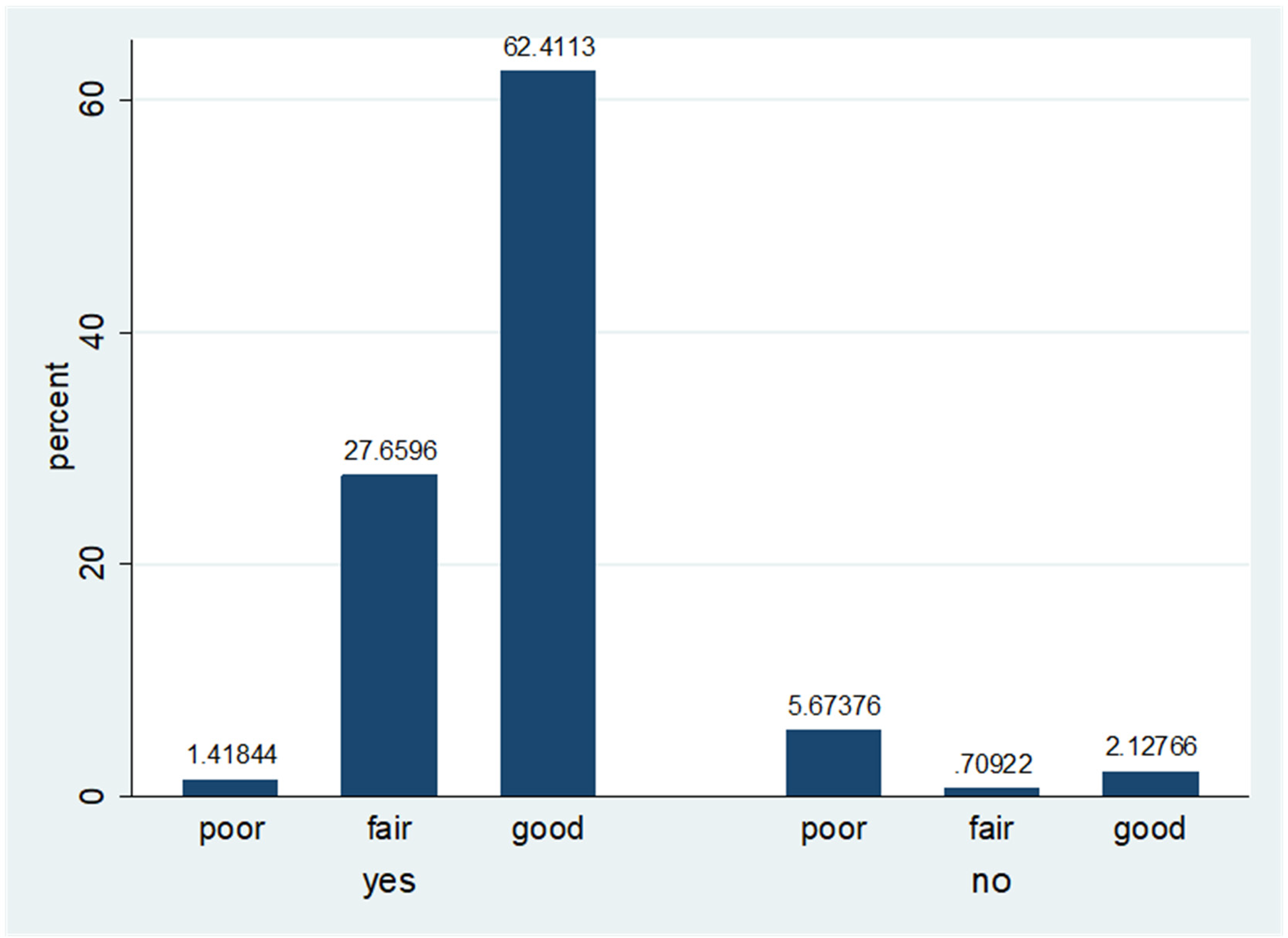
Distribution by knowledge and personal assessment of current method.
Table 3 details the participants’ awareness of contraceptive options as well as their top choices. Most of the respondents (82.9%) have knowledge of the method of choice of contraceptive. The proportion of participants who are aware of various contraceptive techniques was 87.9% and 87.1% awareness, respectively; injection and implant are the most well-known techniques. Vaginal spermicidal (11.3%) and female condoms (27.9%) are the least popular techniques.
Contraceptive Options and Preferred Method.

Figure 3 shows the percentage distribution of respondents by current method choice. The results indicate that the withdrawal method was most widely practiced (24.8%), followed by condoms (19.2%), implants (17.0%), and LAM (11.4%). Other methods reported were injection (9.9%), IUCD (7.8%), and oral pills (4.3%). Only 1.4 percent of the postpartum mothers used the permanent method of tubal ligation.

Percent distribution of respondents by type of current method choice.
Results from Table 4 showed that there was only a statistically significant relationship between education status and current use of contraceptives (p = 0.019), as there is no statistically significant relationship between other variables.
Association Between Individual Factors and Current Use of Contraceptive.

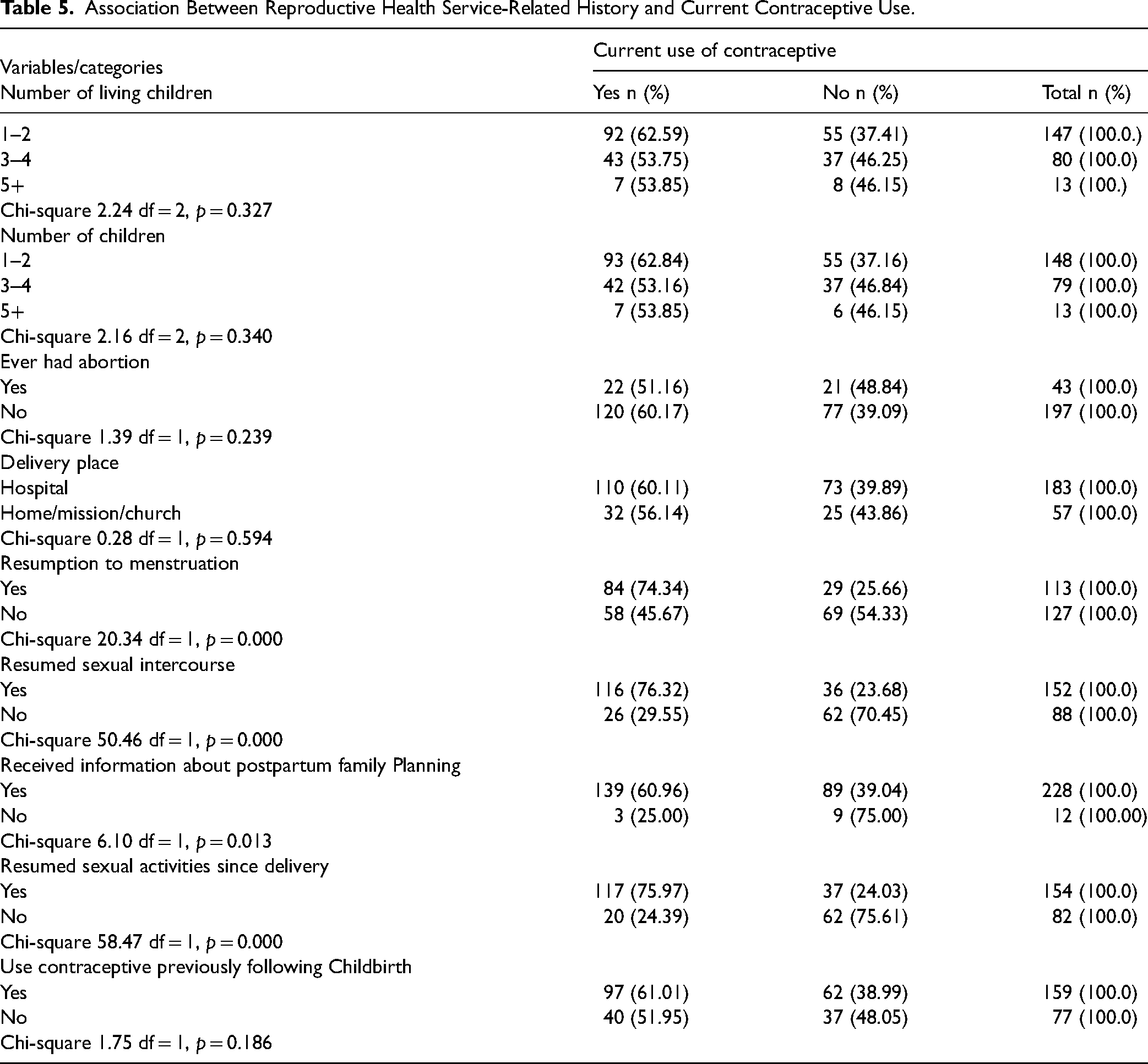
Findings from Table 5 revealed that there was a statistically significant relationship between the current use of contraceptives and resumption of sexual activities since delivery (0.000), resumption of menstruation (0.000), and information received about PPFP (0.013).
Association Between Reproductive Health Service-Related History and Current Contraceptive Use.
Discussion
Current Use of Contraceptives among Postpartum Women
This study was carried out on 240 postpartum women aged between 18 years and 45 years who were randomly selected from health centers. It was found that the majority of the women who used contraceptives postpartum were between the ages of 25 and 34, making up 54.6% of the total population. This is similar to the statistics in Vietnam, where Vu et al. (2016) found higher PPFP among women aged 25–34 and lower for women aged 35 years and above. Based on marital status, 237 (98.8%) of the population were married. From this, it can be implied that more married women used PPFP. However, this opposes the findings from a survey by WHO (2015a) and Blanc et al. (2009). WHO found the highest level of contraceptive use among unmarried, sexually active women between the ages of 20 and 24 years and the lowest levels among postpartum married women between the ages of 25 and 49 years, similar to Blanc et al. (2009), who reported higher contraceptive use among sexually active unmarried females than among married women.
This research indicated that 81.7% of the respondents have planned to have their current baby; this negates Dehingia et al. (2020) conclusion that postpartum women are vulnerable to the possibility of unintended pregnancy. Also, about 65.4% of the women have resumed sexual activities since delivery. Of those who have resumed sexual activities, the majority (91.1%) did so 6 weeks after delivery, in line with Chandra-Mouli et al. (2014) but contrary to Baker (2015), who postulated that postpartum women find it difficult or impossible to speak about sex.
Preferred Method of Contraceptive Options among Postpartum Women
Approximately 67.5% of the respondents have used contraceptives previously following childbirth; this is similar to earlier studies (Chandra-Mouli et al., 2014; NDHSR, 2018; WHO, 2015a; 2015b). Currently, 59.2% of the respondents are using some form of contraceptive. The most common contraceptive method used was withdrawal (24.8%), followed by condoms (19.2%), and implants (17%). This does not conform with the findings of Weller and Davis (2022), who discovered that the perception of male condoms by postpartum women is strong, and even though it is one of the most widely used methods, condom usage rates are still poor. Apter (2018), in an earlier study, found out that the main contraceptive options for postpartum women were condoms backed up by hormonal contraception; however, hormonal contraceptives were used in a longer, mutually monogamous relationship. Vaginal spermicidal (11.3%) and female condoms (27.9%) were the least popular techniques (Apter, 2018; WHO, 2015a).
According to this study, the primary reason for using contraception is to prevent unwanted pregnancy (73.2%) among respondents, with the majority of women (62.7%) obtaining their contraceptives from hospitals. Contrarily, Patricia et al. (2017) noted that postpartum women found condoms humiliating to purchase or obtain from clinics. The proportion of participants who are aware of various contraceptive techniques showed that 87.9% are well-known about injections and 87.1% are well-known about implants. Most of the respondents (91.6%) have knowledge of their current contraceptive method choice, and the majority (64.1%) assess their knowledge as good. Also, a high proportion of women (85.2%) report that their partners are aware of their contraceptive choice, with most women (74.7%) making decisions about contraceptive use jointly with their partner. This is in tandem with previous studies (Blanc et al., 2009; Chandra-Mouli et al., 2014). More than three in five respondents who discussed family planning with their spouse reported current use of contraceptives compared with those who did not discuss family planning with their husband. These results show that both spousal communication on family planning and satisfaction with method choice are significantly associated with current contraceptive use, as supported by Chandra-Mouli et al., (2014).
After giving birth, slightly less than half of the respondents (47.1%) noted that they resumed their periods. This is similar to Yu-Jeong Jeong et al. (2021) findings. The majority of the respondents (95%) claimed they had been given information regarding PPFP similar to a previous study (Yu-Jeong Jeong et al., 2021). This study's findings revealed that most of the respondents (91.7%) affirmed that contraceptives are easily accessible. Other previous studies emphasized the need for contraceptives to be easily and readily available for postpartum women (Weller & Davis, 2022; WHO, 2013).
Health Service-Related History and Current Contraceptive Use
Respondents with lower parity (1–2) and number of living children had the highest prevalence of current contraceptive use compared with those with five or more children. The proportion of respondents who reported having ever had an abortion and who currently use contraceptives was less than those who have never had an abortion (Chandra-Mouli et al., 2014; Dehingia et al., 2020). Among respondents who delivered in the hospital, the percentage of current contraceptive use was higher compared to those who had their child in a house/mission house. Current contraceptive use was significantly higher among the respondents who had resumed menstruation and among those who had resumed sexual intercourse than those who had not resumed menstruation and sex (National Population Commission - NPC and ICF, 2019). Similarly, respondents who received information about PPFP were significantly more likely to be currently using contraceptives than those who did not receive information on PPFP (Chandra-Mouli et al., 2014; National Population Commission - NPC and ICF, 2019; Stover et al., 2017).
Association Between Some Health System Factors and Current Contraceptive Use
Findings from this study indicate that 60.9 percent of respondents who reported the availability of contraceptives compared with 40.0 percent of those who said contraceptives were not readily available were currently using contraceptives as at the time of the survey. This suggests that product availability can enhance using contraceptives (Ashebir & Tadesse, 2020; Stover et al., 2017; Taye et al., 2019). In the same vein, among those who had easy access to clinic locations, a larger percentage was currently using contraceptives. Slightly more than three in five (60.6%) of postpartum mothers who adjudged the attitude of the service provider to be favorable currently use contraceptives when compared with 35.7 percent of those who found the attitude of the service provider unfavorable type (Kinaro et al., 2015).
Strengths and Limitations of the Study
The original and primary data collection from a randomly selected postpartum women sub-population formed the strength of our study. The study was limited by the size of the antenatal mothers studied and the self-report nature of the study. Also, the data were collected at a single point in time using a cross-sectional survey, thus, limiting the generalizability of the findings to other settings.
The Implication of the Study
The findings of this study could help policymakers and governments on the need to sensitize postpartum women to different contraceptives. It will also help the government, community, and policymakers to develop proactive measures to forestall problems associated with births and improve birth outcomes. The study will further help to improve the mental health of postpartum women. Nursing will also benefit from the study as the mortality and morbidity from postpartum women can be reduced. There should be more health education on different available contraceptive methods among postpartum women. Family planning services should be accessible and freely available to women. The stakeholders in health and government should do more advocacies.
Conclusion
This study underscores the profound impact of contraceptive availability on the quality of life for postpartum women in the study area. The evidence base drawn from the study unequivocally demonstrates the far-reaching benefits of accessible contraceptive devices and methods. These benefits encompass improved health outcomes, reduced maternal and infant mortality rates, economic empowerment, and increased educational and career opportunities for women. Moreover, the positive influence on psychological well-being, gender equality, and family dynamics cannot be underestimated. Family planning contributes to broader societal goals, including population and environmental sustainability. The reduction in unsafe abortions and alignment with global and national health policies further underscore the significance of contraceptive availability. As we move forward, it is imperative to prioritize policies and interventions that ensure continued and expanded access to contraceptives, thereby fostering a brighter and healthier future for postpartum women and their communities.
Footnotes
Acknowledgment
We appreciate all postpartum women who participated in this study.
Author Contribution Statement
YRA, OAO, and DTE designed the study. OAO, DTE, and DBO wrote the first draft of the manuscript. YRA, OAO, JAA, and CBB implemented the research. DTE and DBO managed the analyses of the study. YRA, OAO, DTE, CBB, JAA, and DBO managed the literature searches. DTE and DBO revised the manuscript. DTE and OAO supervised the project. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical clearance was obtained from the Ethics and Research Committee of the hospital (PROTOCOL NUMBER: ERC/2022/08/06). Informed consent was obtained from individual participants before the commencement of data collection. In addition, respondents were informed of their right to voluntarily participate or withdraw from the study at any stage without adverse consequences. All methods were performed in accordance with the relevant guidelines and regulations.