
Abstract
Background
Nurses play a key role in cases of cardiopulmonary arrest by promptly attending to and initiating cardiopulmonary resuscitation. Effective cardiopulmonary resuscitation thus requires nurses to possess appropriate attitudes, competencies, and adherence to the best nursing practice. Cardiac arrests are a prevalent cause of fatalities, being responsible for approximately 30% of deaths worldwide. Despite this statistic, however, research in this specific field is lacking in Namibia.
Objective
The objective of this research was to examine registered nurses’ knowledge, attitudes toward, and practice with regard to cardiopulmonary resuscitation at a selected teaching hospital in Namibia.
Methods
A cross-sectional survey design using a self-administered questionnaire was utilized to purposively recruit 158 registered nurses from the inpatient and outpatient departments of a teaching hospital in Namibia. Descriptive and chi-square tests were performed using SPSSv26.
Results
The results of the study indicate that a significant percentage of nurses have limited knowledge (14.7 ± 1.50), negative attitudes (36.2 ± 4.8), and poor practice (11.16 ± 1.18) when it comes to cardiopulmonary resuscitation. Their poor knowledge is strongly associated with poor practice (χ2 = 9.162, P = .002). The study further revealed a significant correlation between the departments in which the nurses worked and their practice of cardiopulmonary resuscitation, suggesting that the work environment is a crucial factor in determining a nurse's approach to emergency care.
Conclusion
The findings of study indicate that the cardiopulmonary resuscitation practice in the selected hospital is unsafe due to the registered nurses’ poor knowledge and negative attitudes. It is strongly recommended that hospital managers and policy-makers take steps to formulate guidelines that mandate regular cardiopulmonary resuscitation training at predetermined times.
Introduction
Cardiovascular diseases are a leading contributor to global mortality, accounting for approximately 30% of all fatalities (Abebe et al., 2021). Cardiopulmonary resuscitation (CPR) plays a crucial role in providing essential life support and remains an effective initial response in cases of cardiac arrest (Nolan et al., 2019). Stine et al. (2019) described CPR as a resuscitative medical procedure that involves a combination of rescue breathing and chest compressions until normal spontaneous blood circulation and breathing are restored. The potential of CPR to save lives during emergencies such as strokes, respiratory arrests, trauma, and airway obstructions is unquestionable (Nolan et al., 2019).
A successful resuscitation requires an integrated set of coordinated actions, including the immediate recognition of cardiac arrest, the activation of an emergency response system, early chest compressions, rapid defibrillation, effective advanced life support, and integrated post-cardiac arrest care (Berg et al., 2020; Kurz et al., 2020). In resource-limited settings, responding promptly to a cardiac arrest poses considerable challenges due to lack of capacity to roll out trainings of healthcare providers; however even developed countries experience challenges with knowledge of, attitudes toward, and practice relating to CPR (Abebe et al., 2021). Possessing the fundamental knowledge and skills, as well as the right mindset, is crucial for healthcare professionals if they are to deliver effective medical care (Ihunanya et al., 2020; Munezero et al., 2018; Zenani et al., 2022).
Review of Literature
The burden of cardiac arrest is on the increase, with global data suggesting a growing mortality rate in Africa as a result of poor CPR practice (Adedinsewo et al., 2019; Mc Namara et al., 2019). Several factors that can contribute to cardiac arrest include hypoxia and hypovolemia and imbalances in electrolytes including hypo-/hyperkalemia as well as hypo-/hyperthermia (Lee et al., 2019; Lott et al., 2021). Other potential causes include coronary and pulmonary thrombosis, tension pneumothorax, cardiac tamponade, and cases of poisoning (Imazio & De Ferrari, 2021; Lee et al., 2019). Additionally, studies have highlighted obstetric hemorrhage and amniotic fluid embolism as possible causes (Feldstein et al., 2022; Schaap et al., 2019).
Within a hospital setting, the predominant factor leading to CPR is attributed to sudden cardiac-related conditions, which account for 60%, followed by respiratory insufficiency at 40% (Andersen et al., 2019). Research suggests that undiagnosed inherited arrhythmia conditions and idiopathic ventricular fibrillation are additional causes of cardiac arrest (Steinberg et al., 2021). Performing CPR has an important position in the chain of survival of adult cardiac arrest; thus it is important for nurses to possess up-to-date information so that cardiac arrest is recognized immediately and implemented effectively, including advanced life support and integrated post-cardiac arrest care (Berg et al., 2020; Soar et al., 2021). Numerous healthcare regulatory bodies acknowledge that the American Heart Association (AHA) and European Resuscitation Council Guidelines have been regarded as a “gold standard” for the management of cardiac arrest and other life threatening emergencies (Rikhotso et al., 2021). Nurses, being the backbone of any health sector, are expected to initiate CPR in emergency situations (Tíscar-González et al., 2020; Umuhoza et al., 2021).
A notable increase in survival rates has been observed in nations that have prioritized CPR training. A significant improvement in patient recovery and discharge rates has been observed in several well-developed nations, such as Sweden and Denmark, which have implemented a comprehensive CPR training policy (Uny et al., 2023). Unfortunately, the implementation of CPR training is a costly endeavor that can only be afforded by highly industrialized countries that have the capacity to roll out training to both healthcare providers and the general population (Barnes & Paterson-Brown, 2017; Heeks & Ospina, 2019). There are inconsistencies in the evidence from lesser developed countries; some studies report that most nurses lack the necessary knowledge to detect initial signs of cardiac arrest, perform a carotid pulse assessment, and use a defibrillator (Chaudhary et al., 2023; Rajeswaran et al., 2018; Sachdeva, 2020; Veronese et al., 2018), while others report that health workers, including nurses, have adequate knowledge and a good attitude regarding CPR (Botes & Moepeng, 2020; Mersha et al., 2020). For this reason, there is an urgent need to investigate nurses’ knowledge, attitudes, and practice in a less developed country like Namibia, where no studies on this topic have been conducted.
In Namibia, CPR is still a developing science, despite a high number of non-communicable diseases such as hypertension, high cholesterol, and diabetic mellitus (MoHSS, 2017), as well as road accidents, all of which can lead to cardiac arrest (Adanu et al., 2020; Jones et al., 2020). CPR training is part of nursing training at both the undergraduate and postgraduate levels. In 2011, the Health Professions Council of Namibia (HPC) issued a directive that mandates all registered health professionals to successfully participate in a set of approved continuing education activities on an annual basis (Mbidi & Damons, 2020). Nevertheless, the extent to which nurses in Namibia have benefited from this compulsory directive in terms of acquiring the necessary knowledge and attitudes concerning CPR remains unknown. This is due to the absence of any directives that require nurses to pass CPR course such as Basic Life Support (BLS), which is provided by the AHA to work as a registered nurse in Namibia.
Methods
Design and Setting
A cross-sectional survey design was used. The study participants were registered nurses working in the medical, surgical, gynecology, intensive care, and outpatient departments of a teaching hospital in Namibia. The hospital has a capacity of 200 beds and admits a high number of patients with both chronic and acute conditions. It is one of the biggest and most specialized referral hospitals in the Kavango east region, located in the eastern part of Namibia.
Sample
The study employed purposive sampling to recruit 158 registered nurses at the training hospital across various departments (see Figure 1). The sample was calculated using Slovin’s formula: n = N/(1 + Ne2) (Mahfouz & Farag, 2015; Tomas et al., 2022), at α = 0.05 confidence level. However, given the small population of nurses at the selected training hospital, the sample size was augmented from the initial calculated sample size of 133 to 158 in order to increase the study's statistical power. The study's eligibility criteria were being at the registered nurse rank, having performed CPR in the past 6 months, and being willing to participate in the study. Considering that the research utilized declarative statements rather than observational methods to examine the practice of nurses, the researchers deemed it suitable to purposefully choose participants who had conducted CPR within the past 6 months. This deliberate selection enabled the participants to reflect and evaluate on their recent practical experiences. Participants who were on leave and those who were unwilling to participate in the study were excluded.
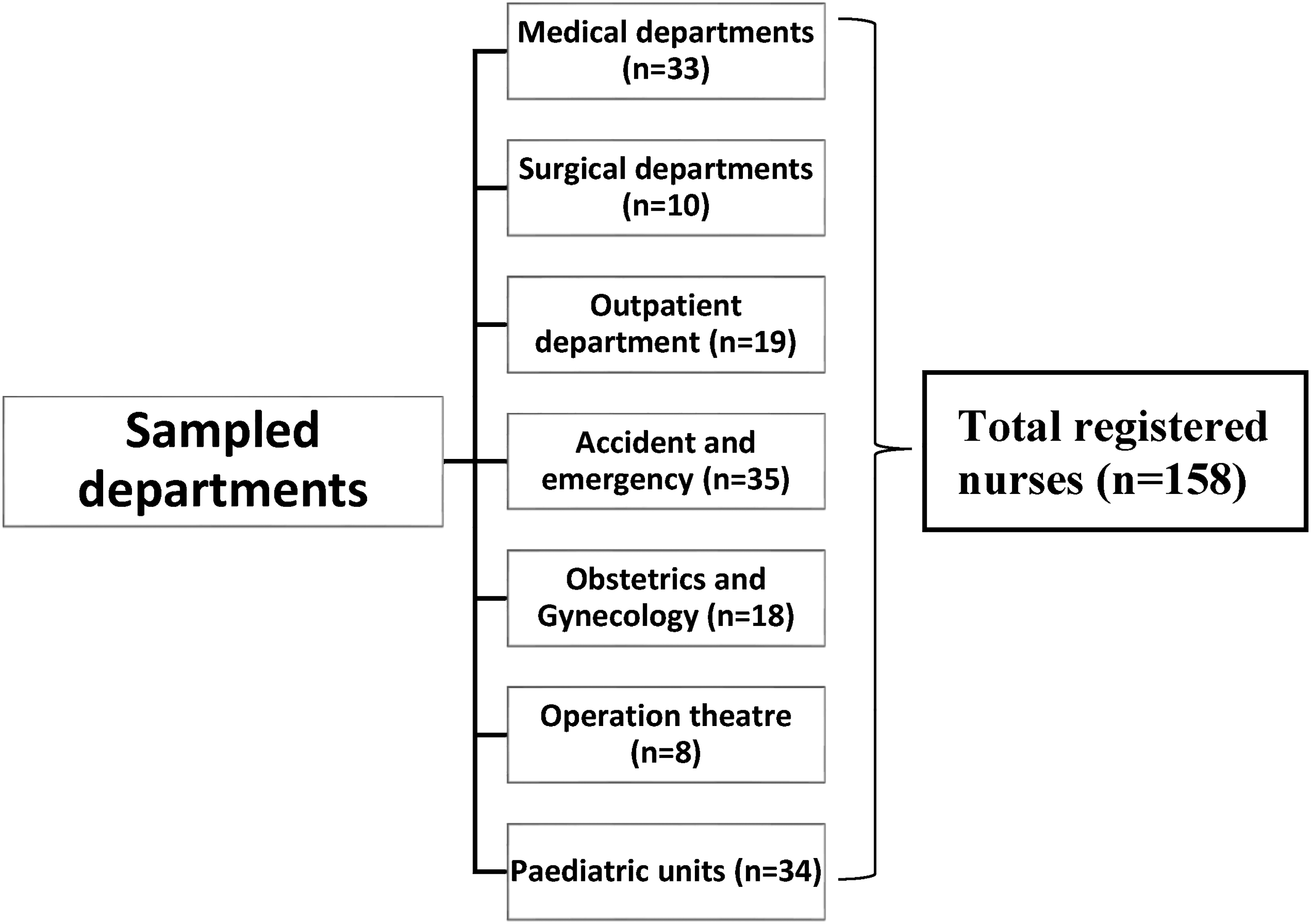
Schematic presentation the study sample at the training hospital in Namibia.
Measurement
The study data were collected through the use of a self-administered questionnaire developed from literature (Ihunanya et al., 2020) and in line with the study objectives. The adaptation of this tool required no permission. Five demographic characteristics of the participants were measured.
Knowledge
Twelve yes/no questions (α = 0.70) measuring knowledge were asked, including “CPR supports and maintains breathing and circulation for an infant, child or adolescent,” “The compression to ventilation ratio for a lone rescuer giving CPR to victims of any age is 20:1,” and “I take 25 s to check for the pulse of an adult before commencing CPR.” The overall scores varied between 12 and 24, with the highest score indicating good knowledge and vice versa. The responses were classified based on their scores, ranging from 19 to 24 indicating good knowledge, while 12 to 18 was classified as poor knowledge.
Attitudes
This was assessed through 10 questions (α = 0.74) that were rated using a 5-point Likert scale, including “I feel CPR is complex and time consuming,” “I feel mouth-to-mouth ventilation should be performed if a mask is not available on a patient during CPR,” and “I feel doctors should be responsible for initiating CPR.” The overall scores exhibited a range from 10 to 50, with a higher score indicating a positive attitude (40–50) and scores between 10 and 39 indicating a negative attitude.
Practice of CPR
The survey utilized nine yes/no questions (α = 0.71) for this section. The participants engaged in introspection and shared the self-reported CPR techniques they utilized during their most recent emergency by answering declarative statements regarding their opinions of their practice, e.g., “I wore latex gloves before commencing CPR,” “I pinched the patient's nostril before giving mouth-to-mouth ventilation,” and “I checked for the patient's pulse rate before commencing CPR.” Numerous studies have employed declarative statements to assess the practice of nurses (Abebe et al., 2021; Guteta, 2022; Nasri & Bulushi, 2020). The overall score spanned between a minimum of 9 and a maximum of 18, with a score of 14 to18 denoting good practice, while scores of 9 to 13 indicated poor practice.
Procedure
One of the researchers (ZAK) visited various departments to explain the study purpose to the potential participants. After obtaining their informed consent, the researcher and a trained researcher assistant distributed 200 self-administered questionnaires enclosed in envelopes to different departments. The participants were required to complete the questionnaires from the comfort of their homes and return the completed questionnaires enclosed in the envelopes. The completed questionnaires were collected for a period of 2 weeks, after which the researcher made verbal reminders to the participants through the unit supervisors. The questionnaires were distributed in September 2022, based on the number of registered nurses allocated to the specific units. A maximum of two reminders as a follow-up were made for those who did not complete the questionnaire the first time.
Ethical Considerations
The Research Ethics Committee of the Ministry of Health and Social Services and the teaching hospital (Ref: 22/4/2/3) granted approval for this study. In conducting the research, the researchers have strictly followed principles outlined in the revised Declaration of Helsinki, including obtaining written informed consent; ensuring confidentiality, privacy and anonymity; and respecting the participants’ right to withdraw from the study. Participation in the study was completely voluntary, and there was no obligation to provide personal identification data. The collected electronic data could only be accessed by the researchers involved.
Data Analysis
The statistical analysis of the data was conducted through SPSSv26. Descriptive statistics, such as frequency, mean, percentages, and standard deviation, were employed to provide a comprehensive overview of the demographic characteristics, knowledge of, attitudes toward, and practice of cardiopulmonary resuscitation. The inferential statistics were derived through the use of the chi-square test at 0.05 significance level.
Results
The demographic information collected from the participants in the study is presented in Table 1. Of the 200 questionnaires distributed, 158 individuals completed the questionnaires, resulting in a response rate of 93%. The participants were asked to indicate their age in years, with the majority falling between 20 and 29 years (51%), followed by 30 to 39 years (43%), 40 to 49 years (4%), and 50 years or older (1%). The educational qualifications of the participants were also recorded, with 64% possessing an RN/diploma, 7% having an RN/post basic, 25% holding a BSc, and 4% being MSc candidates. Only six participants did not respond to this question. The participants were then asked about their years of experience, with 78 (n = 123) having 0 to 5 years of experience, 21% (n = 33) having 6 to 15 years, and only 1% (n = 2) having more than 25 years of experience. Regarding professional rank, 77% (n = 121) of the participants were registered nurses, 15% (n = 24) were specialized registered nurses, and 8% (n = 12) were senior registered nurses. One participant did not provide a response to this question. Finally, the departments in which the participants worked were identified, with the highest percentage working in the accident and emergency department (22%), followed by the medical ward (21%), outpatient department (12%), obstetrics and gynecology (11%), other departments (22%), surgical ward (6%), and theater (5%). Only one participant did not provide a response to this question.
Demographic Characteristics.

Overall Nurses’ Knowledge
Table 2 shows that the nurses’ knowledge regarding CPR was poor (mean 14.7 ± 1.50; 63%). The study revealed that many nurses were unaware of the appropriate time required to check for a pulse before initiating CPR, with 94% of respondents agreeing that it should be done after 25 s. In addition, a considerable number of nurses incorrectly believed that chest compressions for an adult should be 7 in. (10 cm) deep instead of the recommended depth of 2.5 in.
Mean Score of Nurses’ Knowledge.

Overall Nurses’ Attitudes
Based on the data presented in Table 3, it is evident that the attitude of nurses toward CPR was negative (mean 36.2 ± 4.8; 65%). The most prevalent negative perception was observed toward administering mouth-to-mouth resuscitation during CPR in instances where a mask was not available, with 39% (n = 62) of participants agreeing with this sentiment.
Mean Score on Attitudes.

Overall Nurses’ Practice
Table 4 indicates the inadequate level (mean 11.16 ± 1.18; 76%) of the nurses’ practice of cardiopulmonary resuscitation practice. The vast majority of the respondents, accounting for 51% of the total, indicated that they did not know that it is required to pinch patient's nostril before giving mouth-to-mouth ventilation, while 34% used the same procedure to administer CPR to children and adults, despite the age differences.
Mean Score on Practice.

Relationship Between Knowledge and Practice of CPR
This study explored the correlation between knowledge and practice of cardiopulmonary resuscitation (CPR) among nurses. The chi-square test revealed a statistically significant relationship between knowledge and practice of CPR (χ2 = 9.162; P = .002); therefore the results imply that a meaningful association exists between knowledge and practice of CPR among nurses (see Table 5).
Cross Tabulation of Knowledge and Practice of Cardiopulmonary Resuscitation.

Relationship Between Practice of CPR and Demographic Characteristics
Table 6 displays a statistically significant Pearson's chi-square correlation between the various departments in which nurses were employed and their practice of CPR (χ2 = 35.482; P = .00). A significant association was found between nurses’ qualifications, years of experiences, and safe practice (P = .05). Conversely, no significant association was detected between age, professional status, and the extent to which nurses implemented CPR (P ≥ .05).
Cross Tabulation of the Practice of CPR and Demographic Characteristics.

Discussion
In order to perform CPR effectively, it is crucial to have a thorough understanding and knowledge of the proper techniques needed (Pivač et al., 2020; Sok et al., 2020). This study examined the knowledge, attitudes, and practices of registered nurses in a selected teaching hospital in Namibia regarding CPR. The results showed that the participants had poor knowledge of the time required to check for a pulse before administering CPR, as well as the required depth of chest compressions for adults. These findings are consistent with similar studies, which have reported poor knowledge of CPR among nurses ranging from 63.3% to 77% (Abebe et al., 2021; Ihunanya et al., 2020). However, the findings of this study were higher than those of some previous studies, which reported nurses’ knowledge of CPR at 60% (Adal & Emishaw, 2023). The differences in results may be attributed to poor education, a lack of refresher training, and the Nursing Council's reluctance to allow nurses to maintain their annual registration without proof of attending any CPD activities (Baloyi & Jarvis, 2020; Mbidi & Damons, 2020).
A recent study in Spain showed that inadequate CPR training can have a negative effect on nurses’ knowledge, prompting the implementation of CPR training for general public (Villalobos et al., 2019). It has been reported that nurses’ poor knowledge of CPR can influence their competence and attitudes toward performing CPR effectively (Andriyani et al., 2019). Poor nurses’ knowledge regarding CPR can have negative implications on patient outcomes in emergency situations; therefore it is crucial for nurses to possess a thorough understanding of CPR techniques and best practices in order to quickly and effectively respond in a crisis. Additionally, the situation in Namibia requires the urgent attention of healthcare managers, policy-makers, and nursing educators to ensure the provision of ongoing education and training programs that equip nurses with the most up-to-date CPR knowledge.
The results of the study indicate a concerning outlook of nurses toward CPR, with the majority displaying negative attitudes toward administering mouth-to-mouth resuscitation in the absence of a mask. These findings align with the conclusions of a study conducted by Abebe et al. (2021) but contrasts with other studies that reported positive attitudes among nurses toward CPR (Hendy et al., 2023; Nasri & Bulushi, 2020). Negative attitudes toward emergency situations can be attributed to factors such as confusion, panic, lack of education, and fear of contracting infections (Hendy et al., 2023).
In addition to negative attitudes, the study also identified poor practices among nurses when it comes to CPR. This negative behavior could be attributed to shortage of registered nurses and high nurse–patient ratio at the selected hospital. Only about 200 registered nurses are allocated to oversee nursing care and are the first point of care in emergency situations. These findings underscore the need to recruit more nurses and focus on training among nurses to ensure the safe and effective administration of CPR.
We found a statistically significant correlation between the departments in which nurses were employed and their practice of CPR (χ2 = 35.482; P = .001). These findings contrast with previous studies that reported no significant relationship between where nurses work and their CPR practice (Guteta, 2022; Ihunanya et al., 2020; Nasri & Bulushi, 2020). In terms of qualifications, a significant association was found between a nurse's qualifications, years of experience, and poor practice (P = .05). These findings support previous studies that indicated a significant relationship between qualification, experience, and good CPR practice [AOR = 1.54, 95% CI: 0.93–2.54] (Guteta, 2022) but contradict Hendy et al. (2023) and Rajeswaran et al. (2018) who found no significant relationship between CPR practice and years of experience. Additionally, the findings support prior studies that show safe CPR practice increase with the possession of a diploma qualification (63.2% to 78.4%) as compared to degree qualifications (Hendy et al., 2023; Nasri & Bulushi, 2020). This could be explained by the difference in sample sizes of diploma holders in the study, as well as differences in sample sizes between studies. There is a general consensus that increasing a sample size is likely to increase the significance in a relationship if it exists (Lakens, 2022; Makowski et al., 2019). The idea of balancing diploma and degree holders in nursing may seem like a good solution, but it may not be effective in the long run. As more nurses with advanced degrees move into non-inpatient care roles, i.e., management posts, the balance between diploma and degree holders could become even more skewed (Bordignon & Monteiro, 2019; White et al., 2019). Therefore, it is important for healthcare organizations to provide incentives and opportunities for nurses to continue their education while still working in direct patient care roles. Further research is needed to fully understand the impact of this trend across multiple settings and to identify strategies to help retain experienced nurses at the bedside.
Strengths and Limitations
The study provides valuable data on the knowledge, attitudes, and practice of nurses at the selected training hospital in Namibia, including a correlation between the three, which is important information for behavior modification. Nevertheless, it is important to acknowledge that there might exist significant disparities between what is expressed and the actual implementation of CPR among nurses. The present study uncovered a notable limitation in the original data collection tool (Ihunanya et al., 2020) that we adapted in this study as it lacked information regarding its validity and reliability. Consequently, doubts were cast upon the trustworthiness of the tool. In order to address this limitation, a reliability test was performed that yielded a higher score than the acceptable threshold of α = 0.70 (Barbera et al., 2020). Measuring nurses’ CPR practices using declarative statements rather than employing the widely recognized direct observational methods (Munezero et al., 2018; Rajeswaran et al., 2018) seems to have affected the effectiveness of assessing the practices of nurses in performing CPR. While the sample size of 158 students is relatively large compared to some studies conducted among nurses (Chaudhary et al., 2023; Limbu et al., 2020), it is still smaller than the sample size in other studies (Abebe et al., 2021; Adal & Emishaw, 2023). Future studies utilizing validated tools and larger sample sizes across diverse settings are thus recommended.
Implications on Nursing Practice
The study discovered that there is poor knowledge, negative attitudes, and poor practice among nurses when it comes to cardiopulmonary resuscitation (CPR), at a training hospital in Namibia. These findings have important implications for patient safety and outcomes and underscore the urgent need for policy-makers and hospital managers to implement mandatory CPR training and education among nurses in this particular setting. The implementation of comprehensive and ongoing training programs, as well as regular competency assessments, will be crucial in addressing these deficiencies and ensuring that nurses are equipped with the necessary skills and knowledge to effectively respond to cardiac emergencies.
Conclusion
The findings of this study indicate that the poor practice of CPR among registered nurses at a teaching hospital in Namibia are associated with insufficient knowledge, inadequate academic qualification, and a lack of experience. These findings are supported by a significant correlation between poor knowledge and poor practice (χ2 = 9,162, P = .002). The practice of CPR among nurses were found to be strongly and significantly related to the departments in which they worked, indicating that the nature of the work environment plays a critical role in shaping their approach to emergency care. However, a significant relationship exists between the qualifications that these nurses possess, their years of experience, and their level of comfort when facing unsafe situations. This suggests that while expertise and experience are important, they may not always be sufficient to ensure optimal performance during an emergency. It is highly recommended that hospital managers and policy-makers implement additional refresher courses and create policies that require nurses to submit evidence of their CPR training renewal at specific intervals. This will ensure that all nurses are consistently up-to-date with the necessary skills and knowledge to effectively administer CPR.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the Ministry of Health and Social Services for granting the permission to conduct the study. Equally the authors would like to thank all the nurses who took time to participate in this study.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on request.
Authors’ Contributions
ZAK: study conception, design, data collection, data analysis, and interpretation. NT: study conception, design, supervision, data analysis, drafting of article, validation, and writing review and editing. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.