
Abstract
Introduction
In order to promote self-care maintenance behavior in patients with heart failure (HF), it is necessary to identify the direct and indirect effects of major latent variables.
Objective
This study aimed to identify structural relationships between different domains of cognitive function, depression and self-care confidence, and self-care maintenance.
Methods
This descriptive study involved a secondary analysis using data of 201 patients with HF from two observational studies in three hospitals in Korea. The structural equation model using AMOS version 24.0 was constructed to assess the relationships among the variables. The Seoul Neuropsychological Screening Battery was used to assess global cognition, immediate/delayed memory, and executive function, and the Self-Care of HF Index v.6.2. was used for self-care confidence and maintenance.
Results
Self-care maintenance was affected by memory function with a significant direct effect (β=.43, p = .006), as well as self-care confidence (β=.70, p < .001). Memory function and global function indirectly affected self-care maintenance through self-care confidence (β = −.37, p = .002; β = .14, p = .030). Depressive symptoms also had an indirect effect through self-care confidence on self-care maintenance (β = −.21, p = .005).
Conclusion
This study confirmed that it is important to increase self-care confidence through supportive care and to maintain memory function for maintaining self-care in the chronic course of HF patients. In particular, this study suggests that it is necessary to perform periodic memory check-ups for chronic HF patients on an outpatient basis, and counseling and education are needed to improve memory and increase confidence in self-care.
Introduction
Self-care for patients with heart failure (HF) is a multidimensional process involving maintenance and management behaviors. Self-care maintenance requires a patient's participation to maintain one's physiological stability, while self-care management requires a patient's decision-making for monitoring and managing symptoms accordingly as they occur (Riegel et al., 2017). Also, self-care confidence is a critically important factor that consistently influenced the effectiveness of self-care behaviors (Riegel et al., 2017). Adequate self-care in patients with HF has been shown to be associated with better health outcomes, such as fewer clinical adverse events and symptom response behaviors (Lee et al., 2018), fewer rehospitalization (Ma, 2019; Vellone et al., 2017), and better quality of life (Vellone et al., 2017). Thus, to reduce major adverse events for patients with HF, it is essential to regularly assess their level of self-care and identify factors that influence it.
One of the important individual barriers to self-care behaviors was poor cognitive function which was prevalent in approximately 30%–40% patients with HF who had a substantial impairment (Cannon et al., 2017; Gharzeddine et al., 2021). Poor outcomes associated with cognitive impairment have been well-documented, particularly its impairment directly associated with poor self-care behaviors in patients with HF (Jaarsma et al., 2017; Zou et al., 2017). Thus, screening for cognitive impairment was critical to prevent potential self-care deficits in patients with HF (Ampadu & Morley, 2015; Cameron et al., 2016; Dardiotis et al., 2012; Faulkner et al., 2021).
Self-care confidence and depressive symptoms were also often reported with reference to self-care. Self-care confidence totally mediated the relationships between cognition function and self-care behaviors (Vellone et al., 2016) and the relationships between knowledge, health literacy, social support, and self-care behaviors in patients with HF (Zou et al., 2017). Adverse impacts associated with depressive symptoms are well documented, such as high morbidity and/or mortality (Dardiotis et al., 2012; Ma, 2019; Vellone et al., 2016) and poor quality of life (Dardiotis et al., 2012). These negative influences on self-care were also reported in patients with HF, and those with depressive symptoms were more likely to have lower levels of self-care behaviors (Ma, 2019).
Review of Literature
According to a systematic review of 26 cohort studies, cognitive impairment was reported in approximately 43% of chronic HF patients, suggesting that the patient's cognitive function level should be considered in treatment planning (Cannon et al., 2017). In addition, systematic reviews reported that cognitive impairment is a common complication of HF, and HF diagnosis increased the odds of cognitive impairment more than 2.6 times, compared to non-HF controls (Ampadu & Morley, 2015; Cannon et al., 2017). Multiple domains of cognitive function include four types of global cognition, attention, executive function, and memory (Dolansky et al., 2016), but there is still a lack of interest in specific domains of cognitive function related to self-care maintenance.
Despite a large body of empirical evidence influencing factors for self-care of patients with HF (Jaarsma et al., 2017), particular domains of concern in cognitive function associated with self-care maintenance are still lacking. In addition, results related to cognitive domains that affected self-care maintenance were inconsistent across previous studies. Among the cognitive domains, poor memory significantly lowered the level of medication adherence (Dolansky et al., 2016), and a study using structural equation modeling showed that short-term memory directly affected self-care maintenance (Vellone et al., 2016). However, another study found that only slow psychomotor speed had a negative impact on self-care behavior in patients with HF (Hjelm et al., 2015). In a previous study of patients with HF in Korea, who had a relatively low level of self-care behavior compared to Western countries, memory function among the three cognitive domains affected only self-care confidence, and none of the three domains had a significant relationship with self-care maintenance behavior (Kim et al., 2015). These study results suggest that it is necessary to identify the factors that affect the maintenance of self-care in patients with HF, among the domains of cognitive function.
Therefore, the purpose of this study was to identify direct and indirect effects by identifying the structural relationships among cognitive function, depressive symptoms, self-care confidence, and self-care maintenance in patients with HF.
Methods
Study Design
In this cross-sectional descriptive study, data for this secondary analysis were obtained from two observational studies conducted on patients with HF.
Setting and Participants
Each of the two parent studies was approved by research ethics, and written consent was obtained from all HF patients. One parent study was a study that confirmed the relationship with the onset of major cardiac events after 2 years in 91 patients who had been diagnosed with HF by a physician for more than 6 months and were under follow-up (Kim et al., 2015). The other parent study was to assess the validity and reliability of the Korean version of the self-care HF index (SCHFI) and included 110 Korean patients with confirmed diagnosis of HF (Kim et al., 2018). All patients are chronic HF patients who have been diagnosed with HF by a physician and are being followed up on an outpatient basis. Subjects were recruited from three cardiology outpatient departments of university-affiliated hospitals located in a metropolitan city and two provinces in South Korea. Patients with HF who visited the outpatient clinic for treatment and had not received self-care training or intervention were potential subjects of this study. Specifically, patients were eligible to participate in this study if they were 30 years of age or older with an HF diagnosis of 3 months or more and they were able to understand and follow the study protocol instructions. Exclusion criteria for the study subjects were those who were diagnosed with chronic diseases involving clinical depression and cognitive impairment, such as dementia, stroke, or terminal cancers.
Since the minimum sample size required for the analysis of the structural equation model for parameter estimation is 15 times the number of the observed variables (Hair et al., 2006), 195 subjects were needed in this analysis given the 13 observed variables included in this study.
Thus, the data from 201 subjects was sufficient for analysis in this case.
Measurement Tools
Cognitive Function
To measure the degree of cognitive function of the research subjects, the Korea Mini-Mental State Exam (K-MMSE), which checks global cognition, and SNSB (Seoul Neuropsychological Screening Battery)-II, which is widely used as a more comprehensive neuropsychological test, were used. The K-MMSE consists of a total of 30 questions, and the possible score range is 0–30, with higher scores indicating better cognitive function. The K-MMSE judged the degree of cognitive impairment using a total score of 23 points or less.
However, in the validity study of K-MMSE, even if the subject belongs to the normal category, the possibility of memory and executive dysfunction is high, so it is recommended to perform the memory and executive function test together with the K-MMSE test (Oh et al., 2010).
Therefore, in this study, among SNSB-II, memory (Seoul Language Learning Test [SVLT]) and executive function (Controlled Oral Word Association [COWA]) were included, and scores for each domain were calculated based on professional manual guidelines (Kang et al., 2012). This was verified for reliability through the test–retest method targeting various population groups (Kang et al., 2012).
The SVLT was used to measure immediate and delayed recall, where after first speaking a list of up to 12 words, subjects were asked to recall the word list in any order, then recalled twice more consecutively for immediate recall, followed by a delay after 20 min. The degree of recall was measured. Possible scores range from 0 to 36 for immediate recall and 0 to 12 for delayed recall, with higher scores indicating better memory.
The COWA test was used together with the ability to have verbal fluency to measure the executive memory function of words. All subjects were asked to generate a word starting with a given letter within 60 s, and a score was calculated by summing the three tests, with higher scores indicating better executive function. Each subcomponent of SNSB-II was validated for various elderly groups (Kang et al., 2016; Oh et al., 2010).
Depressive Symptoms
Depressive symptoms were measured with the validated Korean version of the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001). It consists of nine items on a four-point Likert scale (0–3), with possible scores ranging from 0 to 27 points and five or more points indicating a depressive disorder (Kroenke et al., 2001). Higher scores indicated more severe depressive symptoms. For structural equation modeling, an exploratory factor analysis was performed and classified into three subareas. The reliability and validity of this instrument were verified in a Korean study of HF patients (Song & Kang, 2017). Cronbach's alpha in this study was .85.
Self-Care Confidence and Self-Care Maintenance
The Confidence and Maintenance Subscales of the SCHFI v.6 were used to assess self-care confidence and maintenance (Riegel et al., 2009). It consisted of 10 items for self-care maintenance and six items for self-care confidence. Each item was constructed originally on a four-point Likert scale, and each subscale score was transformed to a 0∼100-point scale. Higher scores indicated better self-care confidence and maintenance. Exploratory factor analysis for the structural equation modeling showed that the confidence subscale was classified into two subareas, and the maintenance was classified into four subareas. The psychometric test of SCHFI v.6.2 showed Cronbach's alpha coefficients ranging from .71 to .96 in each subscale, indicating appropriate reliability and sound model fit (Kim et al., 2018). Cronbach's alphas in this study were .83 for the confidence subscale and .82 for the maintenance subscale.
Data Collection
This study complied with the Declaration of Helsinki, and approval from the institutional review board of the university was obtained. The data collection period for primary research was from September 2017 to April 2018. Data were collected from three university-affiliated hospitals in Seoul and two provinces in Korea with cooperation from the cardiology department of each hospital. Before data collection, the first author of the study and a trained research nurse of each hospital received informed consent from each participant after explaining the purpose and protocol of the study in face-to-face interviews. It was also explained to the patients that they were free to withdraw at any time during the interview.
Data Analysis
We conducted analyses using SPSS ver. 23.0 and AMOS ver. 24.0 to verify descriptive statistics of the study parameters and to determine the model fit with structural equation modeling. Cronbach's alpha was used to test the reliability of depressive symptoms, self-care confidence, and maintenance variables. Pearson's correlation coefficient was used to confirm the correlation between the continuously measured variables.
To establish the structural equation model, confirmatory factor analysis was performed using AMOS ver. 24.0 to verify the validity of the measured variables constituting each latent variable. Convergent validity and discriminant validity were checked for construct validity of the hypothetical model. To check the multicollinearity between the measured variables used in the hypothetical model, the tolerance limit, the variance expansion factor, and Pearson's correlation coefficient were tested. To estimate the parameters of the model analysis, the model was first estimated using the maximum likelihood method, and then, the predictive model was estimated. Structural equation modeling was performed to calculate the direct and indirect path coefficients between the factors. Age and duration of HF, which were found to be influencing factors for self-care of HF patients, were included in the model as control variables. The model's goodness of fit was determined using χ2, goodness of fit index (GFI), comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). We used the bootstrapping method to test the statistical significance of indirect effects and total effects of the modified model on the endogenous variables (number of bootstrap samples = 1,000).
Results
General Characteristics of the Subjects and Descriptive Statistics of Variables
The mean age of the patients was 62.5 ± 11.4 years, and 63.2% were men. The mean duration of the HF was 37.40 ± 40.90 months, and the mean number of rehospitalization was 1.42 ± 1.54 times. Of the patients, 41.8% had a left ventricular ejection fraction rate of less than 40%, and 43.3% accounted for less than the New York Heart Association (NYHA) Class II (Table 1).
General Characteristics of the Participants (N = 201).
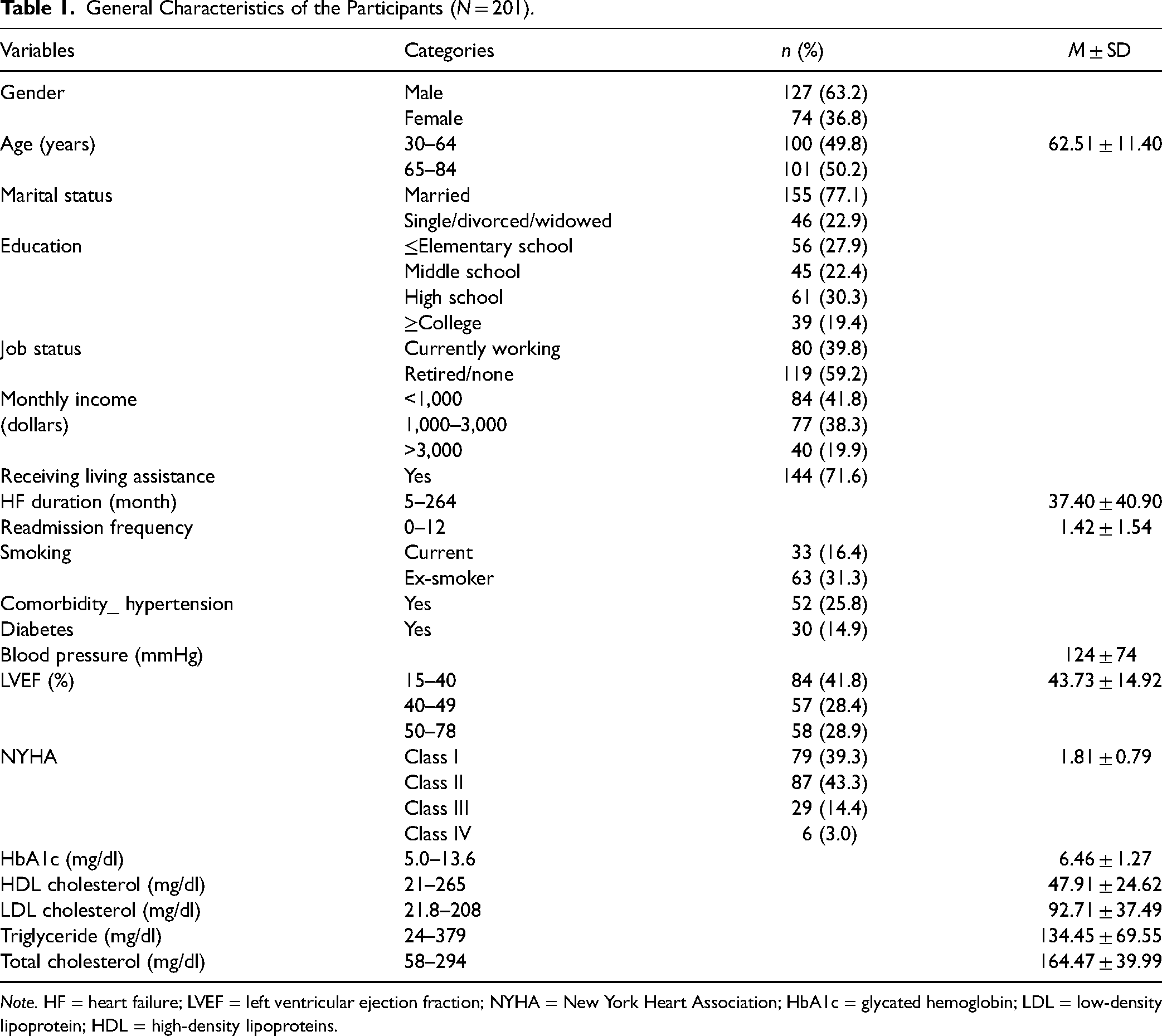
Note. HF = heart failure; LVEF = left ventricular ejection fraction; NYHA = New York Heart Association; HbA1c = glycated hemoglobin; LDL = low-density lipoprotein; HDL = high-density lipoproteins.
The cognitive function of the patients was 64.17 ± 18.65 points out of 144 points, and depression was 4.69 ± 4.82 points out of 24 points. The average self-care confidence score was 37.73 ± 16.80 points out of 100 points, and the self-care maintenance score was 37.73 ± 16.80 points out of 100 points. The basic assumption of the multivariate analysis for the normal distribution of all measured variables of the hypothetical model was verified that the absolute value of skewness (0.01–2.81) was less than 3 and the absolute value of kurtosis (0.13–9.52) was less than 10 (Yu, 2012) (Table 2).
Descriptive Statistics of Variables (N = 201).

Note. MMSE = Mini-Mental State Examination.
Correlations Among Variables and Validity of Latent Variables
Convergent validity and discriminant validity are subtypes of construct validity. Convergent validity can be established if two similar constructs match each other, whereas discriminant validity applies to two different constructs that are easily distinguished. The convergent validity of the latent variables was satisfied in that the construct reliability (CR) was higher than .70 and the average variance extracted (AVE) was higher than .50, and it was confirmed that the observational variables were highly related to the latent variables (Yu, 2012). As a result of the discriminant validity test, it was confirmed that the AVE values of the potential variables were larger than the square of the correlation coefficient (R2) among the latent variables. As a result of the correlation analysis between variables, global cognition showed a negative correlation with depressive symptoms (r = −.24, p = .001) and a positive correlation with self-care maintenance (r = .17, p = .016), but it was not significantly related to self-care confidence. Immediate and delayed recall memory showed a negative correlation with depressive symptoms and a positive correlation with self-care confidence (p < .05). Executive function also showed a negative correlation with depressive symptoms (r = −.21, p = .003). Depressive symptoms showed a negative correlation with self-care confidence (r = −.19, p = .007) and self-care maintenance (r = −.18, p = .013). Self-care confidence showed a statistically significant positive correlation with self-care maintenance (r = .40, p < .001; Table 3).
Correlations Among Variables and Validity of Measured Variables.
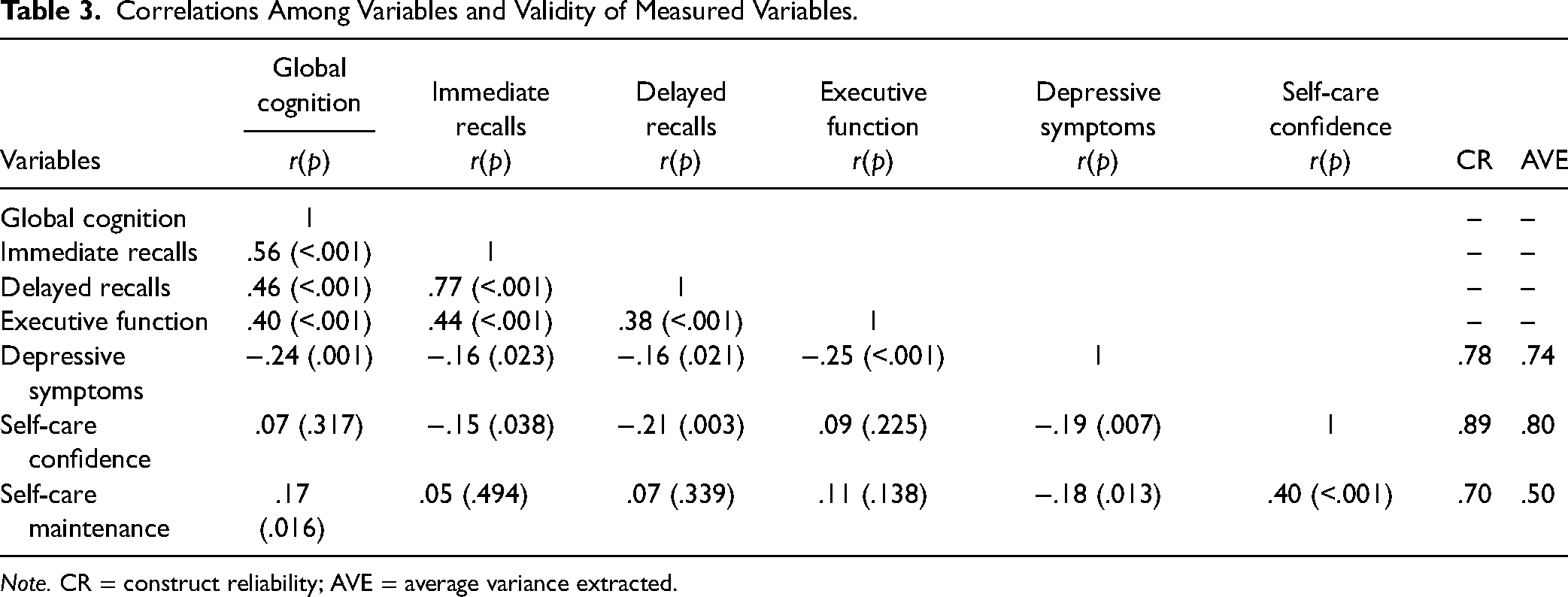
Note. CR = construct reliability; AVE = average variance extracted.
Standardized Direct, Indirect, and Total Effects of the Model
The linear regression analysis showed that the tolerance was .68–.89 and that the variance inflation factor (VIF) was 1.86–2.72, a result of less than 10, thereby indicating that there was no multicollinearity. This study measured χ2 = 95.28 (df = 66, p = .011), GFI = .94, TLI = .94, CFI = .96, RMSEA = .05 (.02–.07), and SRMR = .05, thereby indicating a good level of fitness. The fitness index of the confirmatory factor analysis showed that the fit index was χ2 = 87.85 (df = 56, p = .004), GFI = .94, TLI = .93, CFI = .95, RMSEA = .06 (.04–.08), and SRMR = .06, thus indicating a good level of fitness (Yu, 2012). Age and duration of HF were included in the model as adjusted measured variables.
Memory function including immediate and delayed recall had a direct effect on self-care maintenance (β = .43, p = .006) and an indirect effect through self-care confidence on self-care maintenance (β = −.37, p = .002). Self-care confidence also had a direct effect on self-care maintenance with a significant total effect (β = .70, p < .001). Global cognition (β = .14, p = .030) and depressive symptoms (β = −.21, p = .005) showed indirect effects through self-care confidence on self-care maintenance. Memory function, depressive symptoms, and self-care confidence explained 50% of self-care maintenance (R2 = .53). For self-care confidence, global function had a positive direct effect (β = .20, p = .043). However, memory function (β = −.53, p < .001) and depressive symptoms (β = −.30, p = .002) showed negative direct effects on self-care confidence (Table 4). The parameter estimates are shown in Figure 1.

Results of final model analysis with age and heart failure duration controlled. X1 = immediate memory function; X2 = delayed memory function; X3 = depressive mood; X4 = physical symptoms; X5 = negative thinking; Y1 = symptom appraisal; Y2 = symptom management; Y3 = diet control; Y4 = exercise; Y5 = symptom monitoring and medication; Y6 = medical follow-up; e1∼e11 = measurement error; D1–D2 = structural error. Note. The values on the line refer to standardized regression coefficients; rectangle = measurement variables; circle = exogenous and endogenous latent variables. *p < .05, **p < .01.
Effects of Variables in a Structural Equation Model.

Note. SE = standard error; CR = critical ratio; SMC = squared multiple correlations.
Included immediate and delayed recall memory.
Discussion
The main findings of this study confirmed the structural relationship between cognitive function domains, depressive symptoms, and self-care confidence, all of which were found to be important factors in maintaining self-care behaviors in patients with chronic HF. Among the cognitive domains, the memory function had a significant direct effect on self-care maintenance, and this memory function, as well as global cognition, had an indirect effect on self-care maintenance through the mediation of self-care confidence.
Specifically, memory function including immediate and delayed recalls showed a positive direct effect on self-care maintenance, and it had an indirect effect through self-care confidence on self-care maintenance in this study. These findings are consistent with the results of a structural equation modeling study in that memory among cognitive domains had a direct effect on self-care maintenance in patients with HF (Vellone et al., 2016). In addition, the results support the findings that in a prospective observational study of patients with HF who had not previously been diagnosed with dementia, only memory function among the cognitive functions of the patients was a significant predictor of medication adherence even after adjusting for depression, social support, and disease severity (Dolansky et al., 2016). A systematic review and meta-analysis study also supported the finding that recall testing was the most effective way to detect mild cognitive impairment (Tsoi et al., 2017). However, this differs from previous studies in which regression analysis reported that psychomotor speed was the only cognitive dimension to self-care behavior (Hjelm et al., 2015). In addition, global cognition as measured by the K-MMSE in this study was found to be a factor with an indirect effect on self-care maintenance. This finding is consistent with a previous study of Italian patients with HF that reported on global cognition indirectly influencing self-care behaviors only through self-care confidence (Vellone et al., 2015). The results of the current and prior studies recommend cognitive functional performance should be considered for enhanced self-care maintenance, particularly global cognition, memory, or psychomotor speed. Furthermore, in this study, considering that there is a difference in cognitive function with increasing age, factors affecting self-care maintenance were identified through regression analysis by dividing them into the adult group and the elderly group. As a result, delayed memory function was confirmed as a predictor in adult patients under the age of 65, so it is necessary to regularly monitor the memory function of middle-aged HF patients and to check the degree of self-care among those with low memory function.
Self-care confidence had the greatest direct effect on self-care maintenance in this study, and it was also found to be a mediator in the relationships between global and memory function and self-care maintenance. This result is similar to results of past studies in which self-care confidence was a critical factor influencing self-care behaviors (Zou et al., 2017) and mediated the relationship between cognitive function and self-care behaviors (Vellone et al., 2016). However, a longitudinal study reported that self-care behaviors in daily life, such as poor medication compliance, are not easily improved (Pancani et al., 2018) and require special intervention for patients with HF with low self-care. Interventions can include the development of the patients’ behavioral skills for self-care (Harkness et al., 2015) and social support for increased self-care confidence (Davis et al., 2015; Fivecoat et al., 2018). Therefore, self-care confidence must be increased by providing counseling and education from healthcare professionals to patients, especially for those with low cognitive function, and by assessing their self-confidence as early as possible after the initial HF diagnosis.
As for self-care confidence, global cognition had a positive direct effect, whereas memory function had a negative direct effect on self-care confidence in this study. This result is not consistent with a previous study in which the relationship between self-care confidence and cognitive function was positively associated (Fivecoat et al., 2018). One reason for the dissimilar results may be that the level of self-care confidence of Korean patients is low, compared to those of patients with HF in other countries (Vellone et al., 2016). The majority of subjects in this study showed self-care maintenance and self-care confidence levels below the cut-off point of 70, with average scores of self-care confidence and maintenance being 50.4 and 53.9 points, respectively. These are significantly lower than the average scores of 75.8 and 66.8 points in the US study (Vellone et al., 2016), despite the subjects having the same average age of 62 years. Possible reasons for having a low score and an inverse relationship with the cognitive score may be the result of differences among the items included in the measurement tool. The items in the self-care confidence tool included evaluating their symptoms, alleviating those symptoms, and evaluating the effectiveness of the treatment. In Korea, most patients remain dependent on their physicians and follow their treatment instructions; therefore, their confidence in practicing self-assessment of the effects of symptoms and medication in daily life is predictably low. This suggests that Korean patients with HF lack active attention to treatment and their symptoms.
Depressive symptoms showed a negative direct effect on self-care confidence with the significance of the total effect, and they also affected self-care maintenance indirectly through self-care confidence in the current study. These findings are consistent with a literature review wherein a depressive symptom was identified as a factor that negatively affected self-care behaviors (Riegel et al., 2017). This also supports a study that patients with HF with depressive symptoms were more likely to have lower levels of self-care and higher rehospitalization rates (Jaarsma et al., 2017). According to another literature review, the prevalence of depression reportedly ranged from 24% to 68% in Korean patients with HF (Hwang & Choi, 2016). Further, patients with HF with a combination of depressive symptoms and physical frailty had 3.5 times higher risk of cognitive impairments compared to those without those factors (Lee et al., 2018). One randomized experimental study reported that cognitive behavioral therapy was effective in lowering depression (Freedland et al., 2015). Therefore, it is necessary to increase self-care confidence through counseling and education for depressed patients with HF.
Limitation of the Study
First, the study subjects were recruited by convenient sampling from three hospitals in Korea, so it is difficult to generalize the results to all chronic HF patients in Korea. Second, many patients with HF have common comorbid conditions, such as diabetes mellitus and hypertension that could affect cognitive function, which was not controlled in this study. Although statistically corrected, latent variables according to age and HF duration were not considered, which is a limitation of this study. Further, the sources of the cognitive function in patients with HF were secondary data obtained from previous research projects conducted for different research purposes. Thus, some data may not fit in the same for this secondary analysis; that is, accuracy and sufficiency of data could possibly weaken the study results. Last, the dimension of self-care management was not included in the model because the percentage of respondents who self-managed when they had symptoms was found to be too low, and we did not consider other factors that affected self-care together in the model. In addition, this study was conducted using SCHIFI v.6.2, and in the future, it is necessary to use v.7.2, which has recently been validated for Korean patients.
Strengths and Clinical Implication
These study results imply that periodic memory function screening among cognitive function tests is recommended during the HF patients’ outpatient visits for regular check-ups, and to enhance their self-care behaviors, memory training could be beneficial. Patient education about self-care is also critical to successfully manage the care of HF in which telemonitoring is a useful method for an evaluation of the adherence and ability of self-care of patients with HF. We also suggest further qualitative research on the relationship between memory function and self-care maintenance and confidence, as well as its feasibility.
Conclusions
Self-care confidence and memory function among cognitive domains were found to have a direct effect on self-care maintenance in Korean HF patients. Confidence in self-care was found to play a mediating role in the relationship between cognitive function, depressive symptoms, and self-care maintenance. This study suggests that it is necessary to regularly screen the memory of chronic HF patients who visit outpatients and pay attention to their memory decline and to increase their confidence in self-care through counseling and education.
Footnotes
Acknowledgments
We are grateful to the cardiologists and nurses at Hanyang University Hospital, Chonnam National University Hospital, and Seoul Asan Hospital for helping us with the survey. In addition, we are grateful to all participants in this study.
Author Contributions
Conceptualization, writing—original draft, and formal analysis: JK and SYH; investigation and supervision: JK and SYH; methodology and software: SHK and JLS; resources and data curation: SHK and JLS; funding acquisition: SYH. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Hanyang University Medical Center Ethics Committee (HY-16-05-14). Ethical issues including plagiarism, informed consent, data fabrication and falsification, and double publication have been completely observed by the four authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Research Foundation of Korea (Grant #: NRF-2020R1A2C1013497).