
Abstract
Introduction
This project explored the feasibility of implementing an innovative cross-curricular framework using an adaptive learning (AL) platform and telehealth simulations.
Objective
To determine the feasibility of implementing an innovative cross-curricular framework using an AL platform and telehealth simulations.
Methods
A mixed-method pilot study was conducted using novel AL modules, adaptive case studies, and telehealth simulation.
Results
Quantitative data analysis demonstrated significant correlations within and across demographics using the Technology Acceptance Model (TAM) and Simulation Effectiveness Tool-Modified (SET-M). Specifically, significant correlations are evident between TAM ease of use items 1–6, 8, and 10 and TAM usefulness 1, 3, and 9, with SET-M items 3 and 5–15. Thematic analysis revealed that participants felt that the overall project was worthwhile and increased confidence in telehealth.
Conclusion
Participants found the technology used in this study was easy and useful, and they indicated a positive experience with telehealth simulation. Overall, this study demonstrated that implementation of AL using our paradigm is feasible and supports further investigation into implementing a cross-curricular framework using an AL platform and telehealth simulations.
Introduction/Background
A new psychiatric mental health nurse practitioner (PMHNP) program was being launched at our university to meet the needs of our region for more access to mental health providers. We knew that providing education about telehealth was one potential key to improving patient access (McLean et al., 2013; Shigekawa et al., 2018). We also thought it was essential to integrate critical concepts, including telehealth competencies, throughout this curriculum because the National Organization of Nurse Practitioner Faculties states this is a core competency for nurse practitioners (NPs) (NOMPF, 2022). Since this was a new program, an innovative approach was proposed which connected concepts taught in multiple core courses across the curriculum with telehealth competency modules and telesimulations by integrating those two modalities using an adaptive learning (AL) platform (Realizeit©).
This project's goal was to determine the feasibility of implementing an innovative cross-curricular framework using an AL platform and telehealth simulations. Researchers wanted to examine how an AL platform could be used to support the learning of nursing care concepts related to patients experiencing psychiatric/mental health conditions across multiple courses and to connect lessons on telehealth competencies that can be accessed across these courses. Researchers also wanted to examine the utility of telehealth simulations to support the learning of nursing care concepts and to help students integrate the use of telehealth competencies in practice.
Review of Literature
Delivering learning materials to students in ways that maximize learning is vital (Carroll, 1989; Dziuban et al., 2016). Adaptive learning platforms enable faculty to personalize content and deliver content based on individual differences (Flores et al., 2012). Machine-learning algorithms on AL platforms use continuously assessed data on a student's behavior and progress through content to adjust or “adapt” the student's learning path to help the student achieve maximal learning (Howlin, 2014). Course content can be delivered to a group of students that allows them to progress through concepts in a way that meets their individual needs (Hinkle et al., 2020). Adaptive cases are cases offered in a dynamic versus static fashion using an AL platform. Each case scenario is delivered using embedded variables within the case. Case questions and concept-level question pools allow for a unique experience for each student and for each student's repetition of the case (Hinkle & Moskal, 2018). Simulation has been an integral part of the nursing curriculum for decades, and telehealth simulations are essential in preparing future advanced providers in pandemic and post-pandemic times (Kuszajewski et al., 2021).
Methods
Design
Prior to participant recruitment for the study, two meetings were held with the research team and three expert community mental health providers to determine what telehealth content and case scenario information would be most beneficial to students. Telehealth competency educational materials were then developed by two faculty certified in telehealth using current national telehealth competencies developed by Rutledge and colleagues (Rutledge et al., 2021). The telehealth simulations were written by two faculties who are also PMHNPs and simulation experts who maintain clinical practice, and the simulations were verified by the three community mental health providers. The educational modules and telehealth simulation cases were refined based on their feedback. Introductory PMHNP course modules, telehealth modules, and an adaptive case study based on one of the simulations were then designed within an AL platform (Realizeit©).
Participants were directed to progress through content from the Introductory PMHNP course modules and the telehealth instructional modules before they would be directed to the adaptive case study. Students followed an individualized path through this learning content before proceeding to the adaptive case, but if a student demonstrated a lack of knowledge about critical content, the adaptive platform redirected them back to review this needed content again before the student could proceed to the adaptive case. The adaptive case could be repeated as often as a participant wished in order to practice skills and assess their knowledge, similar to methodology used by Hinkle and Moskal (2018), until a scheduled final “assessment” occurred in a simulated learning environment. The goal was to use the AL platform to prepare students well for the telehealth simulation mental health case assessment.
This was a mixed methods feasibility study conducted at a public university in the southeastern United States. Participants were recruited by email. Eligibility included school of nursing faculty and undergraduate nursing students who had, at minimum, completed their mental health course. After consent, participants were asked to answer questions via Qualtrics® version XM about demographics, telehealth experience, ease of use, and usability from Davis’ Technology Acceptance Model (TAM) (Davis, 1989). Participants were then provided access to the AL platform and asked to go through the content as if they were students. Sign-up times for the telehealth simulation final assessment activity and information regarding focus group activity were provided to the participants. Participants completed a presurvey and modules in the AL platform before the telehealth simulation activity. After the telehealth simulation activity, participants completed a postsurvey with questions from the TAM and Simulation Effectiveness Tool-Modified (SET-M) instruments (Leighton et al., 2018). The TAM postulates that the two primary constructs, perceived usefulness, and ease of use, determine technology acceptance and are critical to the meaningful use of information technology (Davis, 1989). The SET-M survey was developed to evaluate the effectiveness of simulation training (Leighton et al., 2018).
The telehealth simulation took place on an online platform (Zoom©) with standardized patients (SPs) hired from our theater department trained to portray specific mental health characteristics of depressive disorder. One of the research team's PMHNP and simulation experts prepared the SPs. Two researchers were present for every simulated experience. One was a board-certified PMHNP to assist the “student” with resources such as the Patient Health Questionnaire-9 (PHQ-9) screening instrument. The other was an observer checking for the fidelity of the simulated telehealth experience.
Two researchers and one research assistant conducted focus groups via Zoom© a week after the conclusion of the simulations. One focus group was with student participants, and the other was with faculty participants. One researcher facilitated each group with structured interview questions. The other researcher and research assistant took field notes. The focus groups were recorded, and research assistants transcribed the focus groups verbatim. Participants were given a $50.00 gift card after completing all study activities.
Research Questions
What are participants’ perceptions of investigator-developed adaptive cases and telehealth simulations?
What is the perceived ease of use and usability of investigator-developed cross-curriculum adaptive cases and telehealth simulations?
Is implementation of our curricular strategy feasible in a PMHNP program?
Sample
Participants were undergraduate nursing students and school of nursing faculty at the investigator's university. All 13 subjects participated in all aspects of the study. See Table 1 for a demographic summary.
Sample Characteristics.

Total number of participants: n = 13.
aAll participants in this group are faculty.
bAll participants in this group are students.
Inclusion/Exclusion Criteria
Inclusion criteria: Participants were either undergraduate nursing students at the investigator's university or school of nursing faculty at the same institution.
Exclusion criteria: Any potential undergraduate nursing student participants were excluded if they had not successfully completed their undergraduate mental health course in the School of Nursing curriculum. No participants were excluded due to race, sex, or any other background information other than the mental health course completion requirement for undergraduate student participants.
Institutional Review Board
University Institutional Review Board approval was obtained before starting the project, and participants’ consent was obtained in accordance with our university's human subject rights policies at the beginning of the project.
Statistical Analysis
Paired t-tests and correlation analysis were used to assess significant findings related to the TAM and SET-M survey data that were collected with Qualtrics®. Thematic qualitative analysis was used to analyze the post-study focus group results.
Results
Sample Characteristics
A total of 13 (n = 13) participants completed all aspects of this feasibility pilot project. Table 1 shows that six (46.2%) participants were faculty, and seven (53.8%) were students. All participants were female, and most (n = 12, 93.2%) were White and Non-Hispanic. Eleven of the thirteen participants (84.6%) had previous experience with simulation; however, only 4 (30.8%) participants had previous experience with telehealth.
Quantitative Results
Demographic characteristics were correlated with several variables from the TAM and SET-M, as seen in Table 2. The highest level of education showed a strong correlation with the SET-M item about feeling that the prebriefing of the simulation was beneficial to learning, r = .595, p = 0.04, and that telehealth helps to accomplish tasks more quickly, r = .593, p = 0.04. This suggests that the higher level of education one has, the more one feels that prebriefing is helpful to learning. Before the simulation, the TAM item “It is easy for me to remember how to perform tasks using telehealth” correlated with faculty (vs. student) status, r = .590, p < 0.05, and age, r = .689, p < 0.01. That implies that those with faculty status and increasing age found it easier to perform telehealth tasks. Interestingly, post-simulation, this correlation was no longer significant. Lastly, faculty status was positively associated with the SET-M item “pre-briefing increased my confidence,” r = .617, p = 0.02.
SET-M Means Based on Responses on a 1–3 Scale.

Significant correlations are seen between TAM ease of use items 1–6, 8, & 10 and TAM usefulness items 1, 3 & 9 with SET-M items 3, & 5–14 (Table 3). This would imply that individuals who found technology easy and useful felt positive about this telehealth simulation. There is one contradictory correlation to this. TAM Ease of use item 3, “I find telehealth cumbersome to use,” correlated with some of these same SET-M items (above) implying that individuals experiencing this negative feeling about technology felt positive about the telehealth simulation. It is possible that individuals could have both positive and negative opinions about telehealth technology and still find a telehealth simulation to be a positive experience.
SET-M & TAM Correlations.
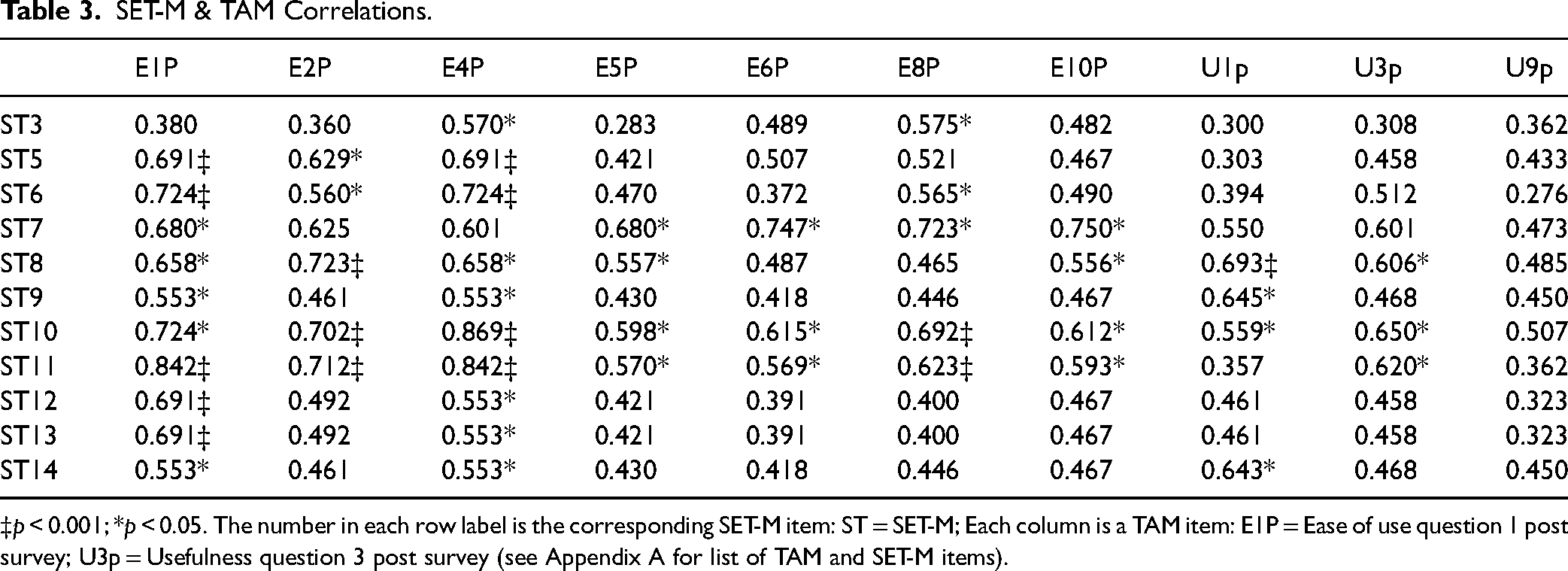
‡p < 0.001; *p < 0.05. The number in each row label is the corresponding SET-M item: ST = SET-M; Each column is a TAM item: E1P = Ease of use question 1 post survey; U3p = Usefulness question 3 post survey (see Appendix A for list of TAM and SET-M items).
The “debriefing contributed to my learning” survey question indicated a mean of 3 (max mean) in the SET-M, which spoke to the impact of debriefing on learning. Both prebriefing and debriefing questions had higher means overall, with prebriefing means of 2.5 and 2.6 on two items and the remainder of the SET-M debriefing questions with means of 3.0 and 2.9. Average TAM scores were compared pre and post-telehealth simulation. While most variables did not show any significant difference, average ease of use and usefulness scores improved post-survey (Table 4). Having found significant correlations in this study using SET-M and TAM demonstrates that we were able to efficiently collect and analyze data with usable results. This indicates that using these instruments to evaluate usefulness and ease of use is feasible going forward with larger studies and eventually the entire curriculum.
Technology Acceptance Model (TAM) Results.

Qualitative Results
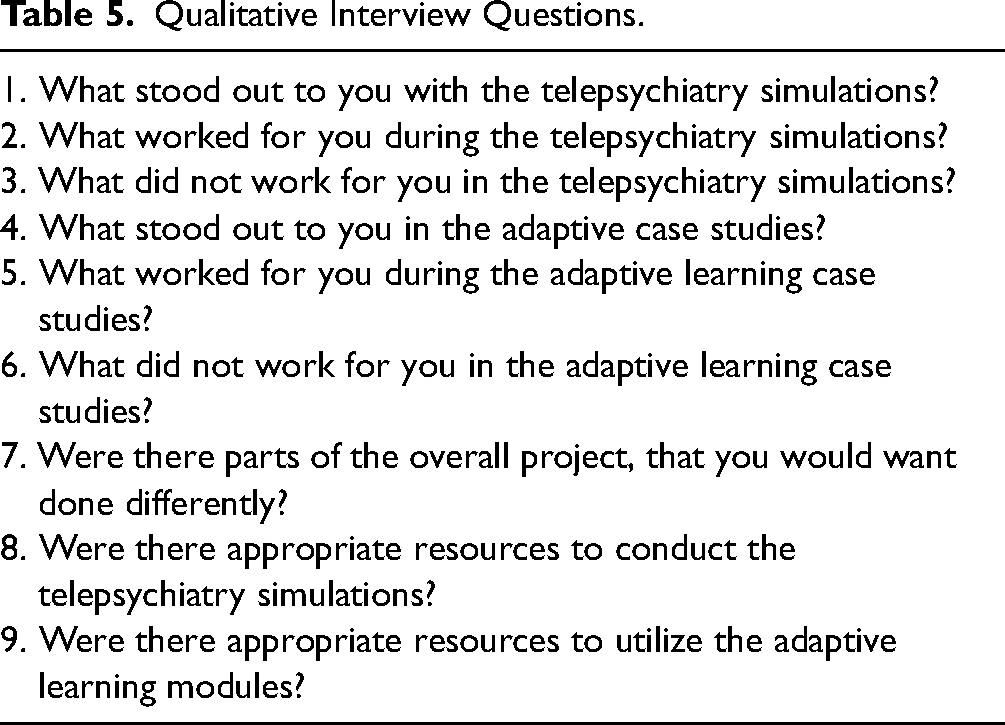
Three research team members independently analyzed the verbatim transcripts, observation/field notes, and memos created by our research graduate assistants and researchers. Using a grounded theory-based analysis, each researcher thoroughly reviewed the data via reading and rereading the data multiple times, coding the emergent themes with keywords/phrases. Codes were then grouped into concepts and categories as the basis of the analysis with a constant comparative method (Kolb, 2012). The rigor of the qualitative design of this study included many aspects to improve trustworthiness of the data. Firstly, participants were asked the same questions in focus groups, and data were collected from a variety of sources including students and faculty. Secondly, researchers had prolonged engagement with data in reading and rereading the responses to questions and focus group content data. Member checking was also included as researchers and graduate research assistants provided checks to confirm the accuracy and interpretation of the data. Students (n = 7) and faculty (n = 6) were interviewed in separate focus groups conducted in a video conference. Questions asked are included in Table 5.
Qualitative Interview Questions.
The coding process created order from the data as each researcher assigned codes using initial open coding to name and develop principles as they emerged from the data and then refined during the subsequent review process with the other researchers. Selective coding took place as the three researchers further defined and highlighted the significant codes. Relationships among the codes were discussed among the researchers, organized, and sorted. As noted in Charmaz and Bryant (2012), data and qualitative analysis inform each other in an iterative process. A grounded theory approach can add evidence within the mixed-method study to better understand data and make operations explicit.
Thematic analysis. The overall project was felt to be worthwhile by the participants and built confidence in telehealth. Some participants felt the project could have included a better overview of the steps in each phase of the project. Although participants were given information via email, there seemed to be disconnect in understanding the project's actual actions. Some stated, “I feel like if there were a little more guidance of how to get started and understanding the whole point of the project, it would have been helpful.” Themes are from students and faculty and then common themes from students and faculty together. Each set of themes has positive and negative codes.
Positive themes. The theme of realism was noted throughout. Participants spoke about the authenticity of the SPs and the case presentation. One stated, “The actor did an efficient job portraying the diagnosis.” Research faculty used the time-out method for participants during the telehealth simulations, which allowed participants to pause for an opportunity to ask clarifying questions or for the faculty researcher to redirect the participant. This debriefing technique could have been related to the theme of liking the deliberate use of debriefing through the simulated experience. One participant stated, “It kind of led me to the right direction to talk to the patient about and actually figure out where to go from there.” Accessibility of resources was noted as one participant stated, “having the PHQ-9/depression scale helped to guide me what to ask,” and another, “the tools really helped me guide the assessment to make sure I was on the right track.” Several participants spoke about how user-friendly the adaptive case study platform was for them. One participant stated, “we were able to go in on our own time and progress through the material, which kept us on track, and we found it easy to use.” Other themes included positive reinforcements throughout the platform and feeling like their learning was enhanced. One participant stated, “liking when the platform told me how I was doing and when I mastered a concept.”
Negative themes. Participants spoke about role confusion and lack of personal feelings during the telesimulation. Non-NP faculty members were uncomfortable playing the role of a PMHNP student. Students verbalized having challenges establishing rapport due to their experience with previous simulations, where previous simulations were very scripted. A few participants spoke about difficulties engaging via video teleconference instead of in person. One stated they “felt it was hard to create a relationship with the patient,” and another participant said that she was “used to using physical touch during therapeutic communication, making it hard for her to find the words to be comforting.”
Some participants noted that learning yet another product for education felt overwhelming. One participant stated, “It was difficult understanding how it worked at first,” and felt like “it would have been helpful to have a tutorial because, for the first 20 min, I was trying to figure out how it worked.” Another theme to note was that participants felt that some material in the adaptive cases did not match the simulation well. Interestingly, negative themes were voiced by the faculty participants more than by student participants.
Discussion
This study aimed to assess the feasibility of implementing an innovative cross-curricular framework using an AL platform and telehealth simulations.
Perceptions of AL Cases and Telehealth Simulations
During our focus groups, all participants answered our query about their perceptions of AL cases and telehealth simulations. Student participants expressed enjoyment in using AL technology and found it reinforced motivation to keep learning. However, faculty participants found the AL platform to be difficult to navigate. The generational gap of faculty participants could have played a role in this discrepancy, as Chica and colleagues speak to this barrier in online nursing programs nationwide (Chicca & Shellenbarger, 2018). Realism in the AL platform and cases was also appealing to participants, as has also been seen in many studies that utilized Association of Standardized Patient Educators best practices in the delivery of simulations using SPs (Hofman & Lobaton, 2016; Jeong et al., 2017; Jones, 2019). Participants reported prebriefing and debriefing of the simulation cases to be most helpful, as well as time outs during the simulations both on the SET-M scores and in their focus groups. Many simulation experts and researchers speak to the importance of prebriefing (Mohamed et al., 2021) and debriefing (Alhaj Ali & Musallam, 2018) as the most integral components of successful simulations. Prebriefing, an essential step in successfully implementing simulated experiences (McDermott et al., 2021), was helpful in this study. Similarly, Kuszajewski et al. (2021) collected SET-M data that showed that prebriefing increased confidence and benefited learning related to telehealth simulations in a NP curriculum. By design, the AL platform used here worked as a quasi-prebriefing tool to better prepare participants for the simulation. As participants worked through the AL case study, they gained essential content necessary to succeed in the telehealth simulation. As evidenced by this study's participant response to the SET-M question indicating that prebriefing increased their confidence, one can assume both the AL platform and discussion with simulation faculty before the start of the simulation were useful. The time-out method utilized in the intraoperative environment to refocus clinicians’ clinical judgment and patient safety can be useful in a telehealth simulation like the one used in this feasibility study (Hofman & Lobaton, 2016; Jeong et al., 2017; Jones, 2019; Kuszajewski et al., 2021; Sarmasoglu et al., 2016).
Perceived Ease of Use and Usability of Telehealth Simulations
Participants who believed telehealth enabled them to accomplish tasks more quickly felt that telehealth was easy to use. Participants who thought they had developed a better understanding of medications (learned in the AL course module and adaptive case) also felt more confident in nursing assessment skills, empowered to make clinical decisions, more able to respond to changes in patient condition, more confident in their ability to prioritize care and interventions that foster safety, more able to communicate with their patient, improvement in ability in teaching patients, more able to use evidence-based practice, and more confident in their ability to report information to the healthcare team.
Similar to this study's results, Davis’ original analysis of the TAM found that technology perceived to be easier to use than other technology and that can address users’ needs is more likely to be adopted (Davis, 1989). Su et al. (2020) used the TAM2 to measure the perceived ease of use and perceived usefulness of telehealth for chronic disease patients and found that the perceived ease of use positively affected the perceived usefulness. They found that both factors positively impacted intention to use (acceptance), although perceived usefulness had a more significant impact. Tsai and colleagues (2019) used the TAM to measure acceptance of telehealth and identify enablers and inhibitors. They found telehealth adoption was enabled mostly through availability and perceived usefulness, whereas it was inhibited mostly due to cost and user anxiety (Tsai et al., 2019). Acceptance also increased when telehealth matched current practices. An et al. (2021) analyzed the acceptance of telehealth while factoring in COVID concerns and found that perceived ease of use, usefulness, and accessibility, increased acceptance, while fear of COVID was not a significant variable.
Technology anxiety may interfere with the adoption of this paradigm, as participants in this study noted in focus groups. Student participants who were accustomed to AL and simulation found the exercise easier to use and more functional. As a group, faculty reported discomfort with the technology, including the AL platform and the telehealth simulations. Kamal et al. (2020) used the TAM to assess the acceptance of telehealth. Using TAM, they found that the more users viewed telehealth as easy to use and valuable, the more likely they were to adopt it in clinical practice.
Strengths and Limitations
Feasibility and usability of the experimental paradigm used in this study were demonstrated. This study was limited by small sample size and the use of only one course, telehealth module, adaptive case, and telesimulation. Further study using a larger number of participants and connected courses with the telehealth modules, as well as multiple adaptive cases and telesimulations, will allow multi-endpoint analyses and greater statistical power.
Implications for Practice
If successfully implemented, our integrated curriculum AL strategy will enhance and reinforce student and practitioner understanding of fundamental telehealth and other clinical competencies. This will result in NP graduates more well-equipped for clinical practice and thus improve the quality of community clinical care and patient health.
Conclusions
Implementation of our integrated curriculum model in the PMHNP program is feasible and practical. While some faculty who participated in this study expressed some discomfort with the technology, students expressed positive reactions to the AL platform, AL case studies, and the telehealth simulations. Logistically, the researchers did not encounter any difficulties with students or faculty accessing the AL platform or lessons/cases within the platform. All participants could also access the telehealth simulations without any significant problems. The next steps will be to fully develop critical courses in the first year of the PMHNP program and apply and evaluate this innovative curricular design using current students within the PMHNP program.
Footnotes
Acknowledgements
The authors would like to acknowledge the invaluable help from our community mental health consultants, Beth Deaton, Julie Fredrickson, and John Nielsen in the initial design of our learning materials and their validation after creation. The authors want to thank our theater student actors, Cierra, Addison, and Elizabeth for their wonderful acting as well as their faculty, Robin Post, for helping connect us with them. The authors also wish to thank our graduate research assistants, Anna Susol and Alexandra Caselman for their work on the focus groups, observations, and transcription. Finally, the authors thank Rachel Kantor, their PhD candidate in statistics at UNCW who provided us statistical help while writing this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a grant from the University of North Carolina School of Nursing.
Appendix A. TAM and SET-M Items from Table 3 correlations.

| TAM Items | SET-M Items |
|---|---|
| Usefulness Items | 3. I am more confident of my nursing assessment skills |
| 1. Using telehealth improves the quality of the work I do | 5. I developed a better understanding of medications. |
| 3. Telehealth enables me to accomplish tasks more quickly | 6. I had the opportunity to practice my clinical decision-making skills |
| 9. Using telehealth makes it easier to do my job | 7. I am more confident in my ability to prioritize care and interventions |
| 8. I am more confident in communicating with my patient | |
| Ease of Use Items | 9. I am more confident in my ability to teach patients about their illness and interventions |
| 1. I find telehealth cumbersome to use | 10. I am more confident in my ability to report information to health care team |
| 2. Learning to operate telehealth was easy for me | 11. I am more confident in providing interventions that foster patient safety |
| 4. I find it easy to get telehealth to do what I want it to do | 12. I am more confident in using evidence-based practice to provide nursing care |
| 10. Overall, I feel that telehealth is easy to use. | |
| 13. Debriefing contributed to my learning | |
| 14. Debriefing allowed me to verbalize my feelings before focusing on the scenario |