
Abstract
Introduction
Middle-aged women experience several changes that can affect their biological and psychosocial health. A healthy lifestyle is a fundamental requirement for achieving optimal health.
Objectives
To examine the impact of psychosocial factors on health promotion behaviors among middle-aged women in Saudi Arabia.
Methods
A cross-sectional, descriptive, correlational study design was used. One hundred and eighteen middle-aged women completed the demographic questionnaire, Stunkard Figure Rating Scale, Perceived Stress Scale, and Health-Promoting Lifestyle Profile-II from September 2, 2020 to February 15, 2021. Multiple regression analysis was performed to estimate the impact of psychosocial factors on health promotion behaviors.
Results
Participants “sometimes” engaged in health promotion behaviors. Spiritual growth scored the highest, whereas physical exercise scored the lowest. Most of the participants were dissatisfied with their body image and reported moderate levels of perceived stress. The participants were more likely to report a preferred body image that was smaller than their perceived body image. Perceived stress and body image were significantly correlated with the total score for health promotion behaviors. Perceived stress level, age, and menopause status were significant predictors of health promotion behaviors. The model significantly predicted all the health promotion behavior subscales, excluding nutrition.
Conclusion
There were relationships between certain psychosocial predictors and health-promoting behaviors. This study can guide healthcare professionals in promoting middle adult women's adoption of health-promoting behaviors. More research can be conducted in Saudi Arabia to understand the health promotion behaviors of middle-aged women.
Introduction
The most frequently used definition of a “middle-aged adult” describes adults aged between 40 and 65 years. During this period, women experience various physiological, psychological, and social changes that may affect their biological and psychosocial health (Polan & Taylor, 2007). For example, they may experience increased vulnerability toward chronic diseases, including but not limited to cardiovascular diseases, cancers, osteoporosis, diabetes, and obesity. Although these diseases are the main cause of mortality and morbidity globally (World Health Organization [WHO], 2018a), approximately 80% of chronic diseases can be prevented by changing lifestyles and adopting health-promoting behaviors such as regular physical activity and a healthy diet (Enjezab et al., 2012).
In Saudi Arabia (SA), chronic diseases are the main cause of death, accounting for approximately 73% of all deaths (WHO, 2018b). The incidence of these diseases increases with age and is more prevalent in women (16.7%) than in men (15.3%) (General Authority for Statistics, 2018). According to the General Authority for Statistics (2018), women constitute a majority of the population (49%). Therefore, the health system outlines most policies based on family health, with particular attention to women's health. Saudi middle-aged women engage in various roles and responsibilities to fulfill the needs of their families, including the management of financial demands and family health. Therefore, practicing a healthy lifestyle is crucial for their well-being, as well as that of the entire family and community.
Review of Literature
Adopting healthy behaviors is a fundamental requirement for achieving optimal wellness for all age groups, particularly middle-aged women. The World Health Organization (WHO, 1986) describes health promotion as the “process of enabling people to increase control over and to improve their health.” Pender and Pender (1996) described health promotion behaviors as a compound pattern that includes six dimensions: nutrition, physical activity, stress management, health responsibility, interpersonal relationships, and spiritual growth.
Previous research has described health promotion behaviors among middle-aged women of different nationalities and ethnic groups, such as African American women (Smith et al., 2017), American women in Michigan (Fisher & Kridli, 2014), and Iranian women (Enjezab et al., 2012; Sehhatie et al., 2015). Other studies have also reported similar findings—middle-aged women sometimes engaged in health promotion behaviors. However, Saudi women have not been the focus of this research. Among Saudi adults, Ashgar (2021) reported moderate adoption of health promotion behaviors during the COVID-19 pandemic. However, no study has specifically investigated middle-aged Saudi women to describe and understand their health promotion behaviors.
Previous research has identified psychosocial factors as predictors of health-promoting behaviors among middle-aged women. However, these findings have been inconsistent. For example, employment was found to be negatively associated with health promotion behaviors in one study (Enjezab et al., 2012) and positively associated with health promotion behaviors in another (Kim et al., 2011). Furthermore, being married and having a higher education were found to be positively correlated with health promotion behaviors in one study (Sehhatie et al., 2015) and not significantly correlated in another study (Cho et al., 2014). Similarly, having children was negatively associated with health promotion behaviors in two studies (Enjezab et al., 2012; Sehhatie et al., 2015), but not significantly correlated in another study (Kim et al., 2011). In contrast, stress level, health literacy, body image, perceived benefits, health-related quality of life, health education programs, chronic diseases, interpersonal support, spiritual well-being, and self-efficacy were all significantly correlated with health promotion behaviors among middle-aged women (Cho et al., 2014; Hurlbut et al., 2011; Nazari et al., 2016; Tsai et al., 2014).
Although the current literature has described health promotion behaviors among middle-aged women of various ethnicities and their associated factors, the existing conclusions may not apply to Saudi middle-aged women, owing to cultural differences. Therefore, understanding health promotion behaviors among middle-aged women and their associated psychosocial factors would help healthcare providers and policymakers develop appropriate and tailored programs to enhance health promotion behaviors and, subsequently, overall health among Saudi Arabian women. This study aimed to describe health promotion behaviors among middle-aged women in SA and examine the impact of psychosocial factors on health promotion behaviors.
Methods
Design
This study employed a cross-sectional, correlational, and descriptive design.
Research Questions
There were two main research questions: Is there a relationship between psychosocial factors (age, years of education, employment status, family roles, menstruation status, chronic disease, body image dissatisfaction, and perceived stress) and health promotion behaviors among middle-aged Saudi women? Do psychosocial factors predict health promotion behaviors in this sample?
Sample
Through convenience sampling, 118 middle-aged women were recruited in this study to detect a medium effect size (ES = 0.15) at a power of 0.80 and statistical significance set at .05. The sample size was determined using G-Power software.
Inclusion and Exclusion Criteria
The inclusion criteria were women aged 40–65 years who lived in SA. Data were collected from September 02, 2020 to February 15, 2021. A 15 to 25 min survey was conducted online by distributing the link through the WhatsApp social networking site and was available in Arabic.
Assessment Tool
The survey included four sections: demographic data, Stunkard Figure Rating Scale (FRS), Perceived Stress Scale (PSS), and Health-Promoting Lifestyle Profile-II (HPLP-II). Psychosocial factors included age, menstrual status, family roles, job status, years of education, chronic disease, body image satisfaction, and perceived stress level. Six variables were measured using categorical scales, while age and years of education were measured using an interval scale.
Menstrual status was defined as having the last menstrual period at least within the last 3 months or more than 3 months ago. To evaluate the stressfulness of family roles, women were asked to identify their roles within their families from six listed roles. Women were classified as having stressful family roles if they selected three or more roles from the six listed roles or if they had to provide care for two different generations (e.g., adolescent children and elderly parents). Job status was measured as a dichotomous variable, with yes or no responses. For chronic diseases, women were asked to identify all chronic diseases that they were diagnosed with. They were then classified as having at least one chronic disease or not having any chronic disease.
Body image satisfaction is defined as the perceived actual body size minus the perceived ideal body size (Lynch et al., 2009). The FRS was used to measure body image perception (Figure 1). The FRS is a rating scale comprising nine silhouettes of women ranging from extremely underweight silhouettes (1) to extremely obese silhouettes (9). Previous research has indicated preferable test–retest reliability and moderate associations of the FRS with other measures of body image dissatisfaction; therefore, it is an appropriate assessment to investigate it (Thompson & Altabe, 1991). Participants were asked to identify the figure that represented their current body image and then identify the figures that they would prefer for themselves. A score of 0 or ±1 was considered body image satisfaction, and a score of ±2 or more was considered body image dissatisfaction.
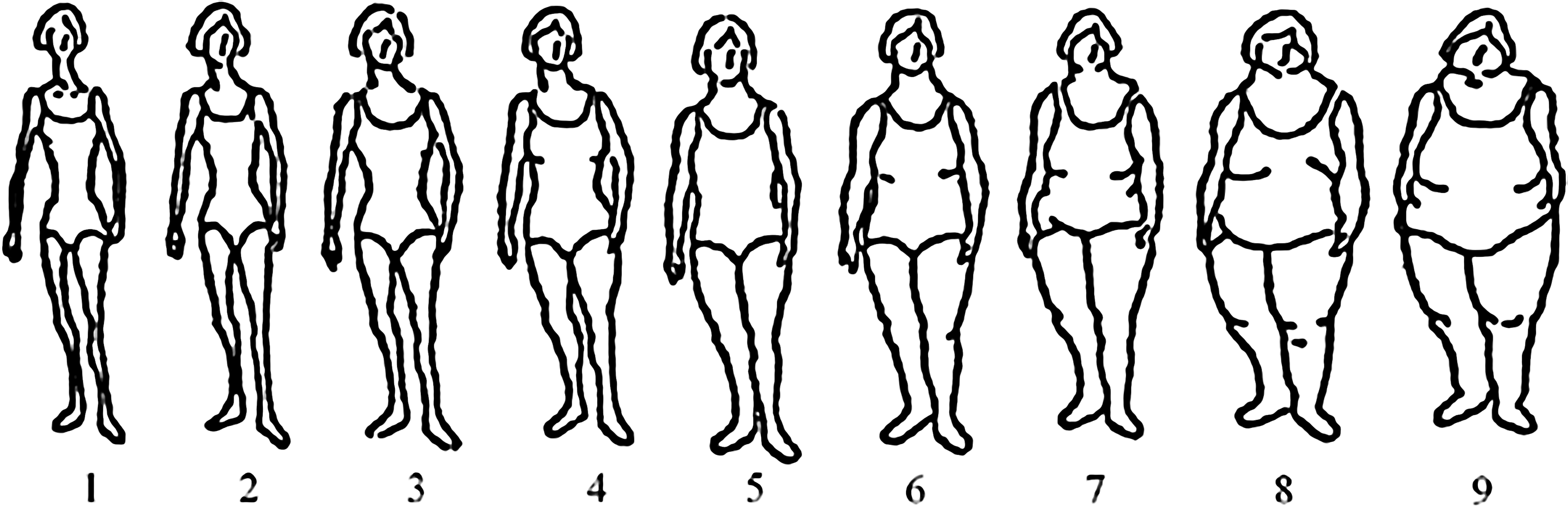
Stunkard figure rating scale (FRS).
Perceived stress was measured using the PSS. It measures the personal perception of stress (Cohen et al., 1983). This scale asks participants about their feelings during the previous month. In each question, the participants were asked how often they felt a certain way. Total scores were calculated by reverse-scoring the responses to the four positively stated items (items 4, 5, 7, and 8) and then summing all the scale items.
Health promotion behaviors were the outcome of this study and measured using the HPLP-II. The HPLP-II includes a total scale and six subscales to measure health behaviors in the theorized definition of health promotion (Walker et al., 1987). The total scores were calculated using the mean of 52 items. Higher scores indicate greater participation in health-promoting behaviors.
Statistical Analysis
Data analysis was conducted using the IBM SPSS Statistics (V25.0). A one-sample t-test was used to estimate the 95% confidence interval and population means, and a paired-sample t-test was used to compare the perceived body image and preferred body image means. The two-tailed Pearson's r correlation test was used at an α of .05, to assess the magnitude and direction of the association between health promotion behaviors and psychosocial factors (Hypothesis 1). Multiple regression analysis was performed to estimate the impact of psychosocial factors on health promotion behaviors (Hypothesis 2).
The reliability and validity of the scales used in this study have been established in the literature. Thompson and Altabe (1991) reported preferable test–retest reliability and moderate associations with other related measures of the FRS. For the PSS, Cronbach's α for the Arabic version was found to be 0.74 among women (Chaaya et al., 2010). Additionally, it was found to be significantly correlated with both the Edinburgh Postpartum Depression Scale and General Health Questionnaire-12 (Chaaya et al., 2010). For the HPLP-II, the Cronbach's α for the total scale was 0.92 (Alkhawaldeh, 2014), while it was between .70 and .88 for the subscales (Alkhawaldeh, 2014). The internal consistency reliability of the scales for this sample was evaluated using Cronbach's α and was shown to be acceptable (0.85 for PSS, and 0.94 for HPLP-II).
Results
Sample Characteristics
The participants’ average age was 44.64 (5.12) years. Most of the women were from Jazan city (33.1%), married (70.3%), employed (55.1%), and lived in their own house (73.73%), with the average years of education being 13.52 (6.78) years. Most participants reported having children (72.9%), with an average of 4.28 (2.92) children. The average number of people in the household was 5.97 (3.54). Table 1 presents the complete demographic characteristics of the participants.
Demographic Characteristics (N = 118).

Most participants had undergone their latest menstruation cycle within the previous 3 months (76.3%) and reported having a family history of chronic disease (71.2%). Less than half of the participants (44.1%) had at least one chronic disease, with the most common being diabetes (16.9%), rheumatoid arthritis (12.7%), and hypertension (11.9%). Most of the participants were dissatisfied with their body image (74.6%) and reported moderate levels of perceived stress (M = 17.90, SD = 6.87). Additionally, a paired-sample t-test indicated that middle-aged women in this study were more likely to have a preferred body image that was thinner than their actual body image (t = 13.581, p ≤ .0001).
Less than one-third of the participants (30.5%) had stressful family roles, with most of them being homemakers (57.6%). This was followed by caregiving for children (37.3%). Women were more likely to report participating in health promotion behaviors “sometimes” (M = 2.31, range = 1–4). Further, the health promotion behavior subscales were analyzed to determine the most practiced dimension of such behaviors among middle-aged Saudi women. Spiritual growth (M = 2.84, SD = 0.65) was the most practiced dimension, whereas physical exercise (M = 1.78, SD = 0.64) was the least practiced dimension. Tables 2 and 3 provide more detailed information on psychosocial factors and health-promoting behaviors.
Psychosocial Factors (N = 118).

Descriptive Statistics for Perceived Stress, Health Promotion Behaviors, Perceived Body Image, and Preferred Body Image (N = 118).

Research Question Results
Pearson's r correlation coefficient was computed to examine the association between psychosocial factors and health-promoting behaviors. Table 4 presents the correlations between the key variables. Among the selected psychosocial factors, only perceived stress level (r = −.46, p ≤ .0001) and perceived body image (r = −.18, p = .046) were significantly correlated with the total scale of health promotion behaviors. The perceived stress levels were negatively correlated with health responsibility (r = −.23, p = .013), physical activity (r = −.28, p = .002), nutrition (r = −.19, p = .042), spiritual growth (r = −.55, p ≤ .0001), interpersonal relationships (r = −.46, p ≤ .0001), and stress management subscales (r = −.48, p ≤ .0001).
Correlations Between Key Variables (N = 118).
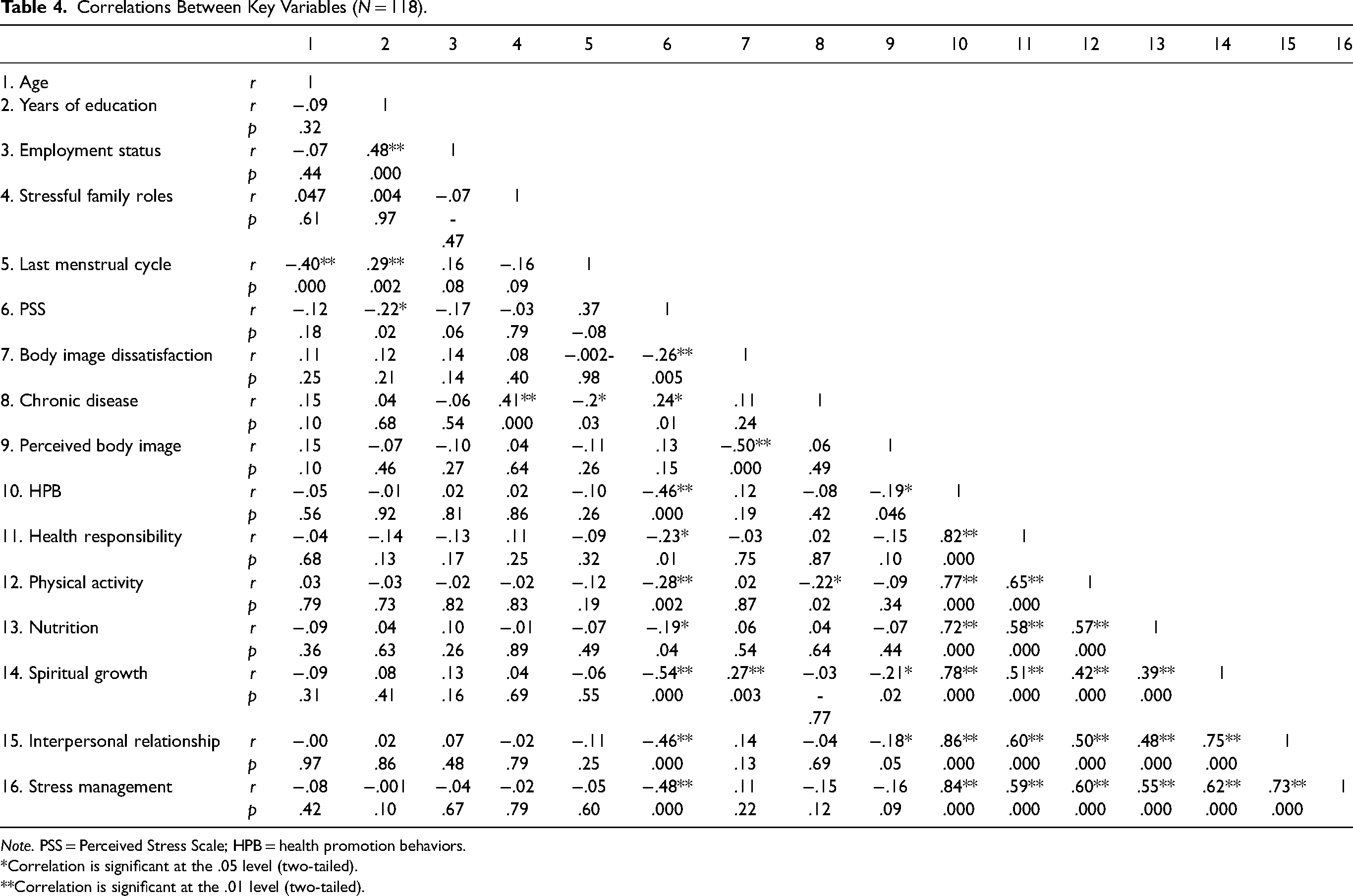
Note. PSS = Perceived Stress Scale; HPB = health promotion behaviors.
*Correlation is significant at the .05 level (two-tailed).
**Correlation is significant at the .01 level (two-tailed).
Body image dissatisfaction was associated with the spiritual growth subscale (r = .27, p = .003), whereas perceived body image was associated with spiritual growth (r = −.209, p = .023) and interpersonal relationships (r = −.18, p = .048). A previous history of chronic disease was only correlated with the physical exercise subscale (r = −.22, p = .015).
Multiple regression analyses were conducted to evaluate the impact of psychosocial factors on health promotion behaviors among middle-aged women (see Table 5). For the total scale, the model revealed a 28% variation (F = 5.193, p < .001), with only the perceived stress level (t = −5.812, p < .001), age (t = −2.413, p = .018), and menstruation status (t = −2.168, p = .032) having a significant partial impact on health promotion behaviors. Furthermore, the model significantly predicted all health promotion behavior subscales, excluding the nutrition subscale.
Regression Analysis Predicting Health Promotion Behaviors (N = 118).

Note. B = unstandardized regression coefficient; SE B = coefficient standard error; Beta = standardized regression coefficient.
For the health responsibility subscale, the model revealed a significant 14% variation (F = 2.158, p = .036), with only perceived stress level having a significant partial impact (t = −3.433, p < .001). For the physical activity subscale, the model revealed only a 14% variation (F = 2.271, p = .028), and only perceived stress level had a significant partial impact (t = −2.676, p = .009). For spiritual growth, the model revealed a 40% variation (F = 8.881, p < .001). Age (t = −3.321, p = .001), menstruation status (t = −2.174, p = .032), and perceived stress level (t = −7.072, p < .001) had significant partial effects on spiritual growth. For interpersonal relationships, the model revealed a 27% variation (F = 4.988, p < .001) with only menstruation status (t = −2.046, p = .43) and perceived stress level (t = −5.755, p < .001), with a significant partial impact. For the stress management subscale, the model revealed 29% variation (F = 5.659, p < .001) with age (t = −2.407, p = .018) and perceived stress level (t = −5.984, p < .001) having a significant partial impact.
Discussion
Although previous studies have investigated health promotion behaviors among middle-aged women, no study has focused on women in SA. Thus, this study examined the impact of psychosocial factors on health promotion behaviors among middle-aged Saudi women. The mean score for health promotion behaviors was 2.31 (0.49), indicating moderate adoption of health promotion behaviors. Similar results of 2.05 (0.22) and 2.73 (0.36) have been reported by Shaahmadi et al. (2019) and Enjezab et al. (2012) among middle-aged Iranian women, respectively. Similarly, Cho et al. (2014) reported a mean score of health promotion behaviors of 2.1 (0.5) among Korean women. Health behaviors are influenced by several psychosocial factors such as social norms, culture, health policies, and physical and social environments (Hawks et al., 2002). Additionally, a qualitative study (Enjezab et al., 2014) demonstrated that the barriers to a healthy lifestyle among middle-aged women are both psychological and social.
Further analysis of the six subscales of health promotion behaviors found that spirituality growth scored the highest and physical activity scored the lowest compared to the other dimensions of health promotion behaviors, consistent with previous work (Aqtash & van Servellen, 2013; Ashgar, 2021; Cho et al., 2014; Enjezab et al., 2012; Shaahmadi et al., 2019). SA is an Islamic country that places prime importance on spirituality, which may explain its higher score in this dimension. Comparatively, the low score for physical activity is inconsistent with a study conducted by Pender et al. (1990) in America, where participants reported a higher score for physical activities. This inconsistency could pertain to the social and environmental factors in SA. For example, Almaqhawi (2022) reported that reduced availability of women-only gyms and open spaces, non-engaging fitness instructors, reduced attention to different age groups, and hot climate in SA are main barriers for Saudi women to engage in regular physical exercise.
Physical activity is expected to prevent chronic diseases in middle-aged women, which are the main causes of mortality in SA. These include cardiovascular diseases, hypertension, diabetes, dyslipidemia, and obesity, which are partly driven by rapid lifestyle changes that increased sedentary behaviors (Mabry et al., 2016). A systematic review of physical inactivity in SA revealed that females are more inactive than males (Al-Hazzaa, 2018), which could be primarily attributed to having limited access to engage in physical activity, especially outdoor leisure-type activities (Al-Hazzaa, 2018), because there are fewer and more expensive fitness centers available to females than to males (Al-Eisa & Al-Sobayel, 2012), and because of greater dependence on cars rather than walking for short distances (Faulkner et al., 2009).
Most participants reported dissatisfaction with their current body image, perceived themselves as overweight, and preferred to have normal body weight. This is consistent with a study on women's health across the United States (Jackson et al., 2014), which revealed that middle-aged American women were more likely to report a smaller perceived body image than their actual body image. Additionally, a cross-sectional survey of 1,081 participants conducted by de Morais et al. (2017) showed that most participants reported body image dissatisfaction. Therefore, the prevalence of body image dissatisfaction was higher in middle-aged women. Similarly, Khalaf et al. (2015), Benkeser et al. (2012), and Runfola et al. (2013) found that most middle-aged women were dissatisfied with their body image.
Perceived stress level was moderate among Saudi Arabian women in this study. Similar results have been noted in previous studies of middle-aged women of various ethnicities and nationalities. Cho et al. (2014) reported a higher level of perceived stress among middle-aged women, indicating that middle-aged women face unique stressors and challenges in their lives. These stressors could be due to work demands, parenting roles, or other family related roles (Dennerstein et al., 2007).
Psychosocial factors were found to influence the health promotion behaviors of middle-aged women. Correlation analysis revealed that, among the selected psychosocial factors, only perceived stress level and perceived body image were significantly correlated with the total scale of health promotion behaviors. These findings clearly explain the inverse relationship between perceived stress and body image dissatisfaction when engaging in health-promoting behaviors. The same finding was noted in a study by Cho et al. (2014), in which levels of perceived stress were negatively correlated with health promotion behaviors. Furthermore, a prospective cohort study reported that individuals with high levels of stress were less likely to adopt healthy behaviors than those with low stress levels (Rod et al., 2009).
Perceived stress level was also negatively associated with the health responsibility, physical activity, nutrition, spiritual growth, interpersonal relationships, and stress management subscales. These findings support the effect of perceived stress on every subsection of health promotion behaviors. Body image dissatisfaction was positively associated with the spiritual growth subscale, whereas perceived body image was positively associated with spiritual growth and interpersonal relationships. However, the available literature to support these findings is limited.
Furthermore, the multiple regression model showed that the perceived stress level, age, and menstruation status had a significant partial impact on health promotion behaviors. The model significantly predicted all the health promotion behavior subscales, excluding the nutrition subscale. As women had higher perceived stress level, age, and being menopaused, health promotion behaviors reduced. These findings are consistent with those of previous studies (Cho et al., 2014; Rod et al., 2009) that support the impact of the biopsychosocial changes on health promotion behaviors among middle-aged women.
Strengths and Limitations
These findings should be considered with respect to the following limitations. First, the use of cross-sectional data collection and convenience sampling may have limited the generalizability of the findings to other middle-aged women in SA. Additionally, utilizing social networking sites to recruit participants and self-report surveys may increase the chances of bias as social networks can reveal other characteristics of the participants, and participants may report inaccurate information. However, using social networks helped overcome recruitment challenges to approach the required sample size. Moreover, the paucity of studies examining health promotion behaviors among adults in SA has limited the ability of the authors to compare these findings. However, the study was evaluated using the Strengthening the Reporting of Observational Studies in Epidemiology Statement: Guidelines for Reporting Observational Studies to enhance its validity (Von Elm et al., 2007), and the reliability of this dataset was examined and found to be acceptable. Irrespective of these limitations, these findings provide several important insights for promoting health in middle-aged women in SA.
Implications for Practice
The findings of this study have implications for health promotion programs and initiatives. Stress levels and body image dissatisfaction were associated with participation in healthy behaviors among middle-aged women. Developmental changes that occur during this period make it essential for nurses to develop comprehensive-culturally appropriate preventive programs that consider all biopsychosocial changes they undergo. Therefore, psychological and emotional support must be embedded in health promotion programs. There is also a need to perform periodic checks for stress levels and body image satisfaction in middle-aged women through primary care centers for early detection and prevention.
Conclusion
To the best of our knowledge, this is the first study to examine the impact of psychosocial predictors on health promotion behaviors among middle-aged women in SA. The study findings revealed that among the psychosocial factors, only perceived stress and perceived body image were significantly correlated with the total score for health promotion behaviors. Whereas, perceived stress level, age, and menopause status were significant predictors of health promotion behaviors. These findings can guide healthcare providers in developing and implementing health programs aimed at enhancing health promotion behaviors among middle-aged women in SA. To overcome the inability to generalize these findings, future research should benefit from experimental studies and the inclusion of comparative groups. Additionally, future research can use these findings as a foundation for further studies on this topic in SA to better understand the health-promoting behaviors of middle-aged women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Approval
Ethical approval was obtained from Jazan University before the recruitment process began in April 2020. A brief introduction to the study was provided in the covering letter of the survey, and informed consent was required to answer the survey questions. Participation in the study was optional and anonymous.