
Abstract
Introduction
Breast cancer (BC) is a most common and frequently occurring malignancy of women worldwide. Breast self-examination (BSE) is important for the early detection and prevention of BC and to limit the morbidity and mortality. Young students are ideal people to understand and motivate other women to perform BSE.
Objective
BSE behavior of undergraduate students was predicted using Champion's Health Belief Model Scale (CHBMS).
Methods
A descriptive cross-sectional design was adopted. This study was conducted in all nine colleges of Sultan Qaboos University, , Oman. Three-hundred eighty-one female undergraduate students were selected through convenient sampling technique. The health belief towards BSE was predicted using CHBMS.
Results
The mean and SD of beliefs about the benefits of performing BSE showed 10.84 and 3.2, respectively. Mean and SD of confidence in performing BSE indicated 56.24 and 10.8. Likewise, the mean and SD of barriers in performing BSE are 13.58 and 4.2. Source of information is found to be a statistically significant predictor of barrier in performing BSE at p < .05.
Conclusion
If the self- confidence of women in performing BSE improves, the women will uptake BSE more frequently thereby they can be prevented from developing the adverse consequences of advanced stages of breast cancer.
Keywords
Introduction/Background
Breast cancer (BC) is a major disease that affects women worldwide and is considered the second leading cause of mortality among this population (Birhane et al., 2015). In 2020, the World Health Organization announced that 2.3 million women were diagnosed with BC, and 685,000 died globally. In 2012, the Global Cancer Project (GLOBOCAN) publicized that BC is the most common cancer in women, accounting for 25.1% of all cancers. In addition, the incidence of BC is higher in developed countries, while the rate of mortality is higher in less developed countries (Ghoncheh et al., 2016; Marzouni et al., 2015). By the end of 2020, 7.8 million women diagnosed with BC were alive in the last 5 years, making BC the most prevalent cancer worldwide (Ginsburg et al., 2020).
More recently, the incidence of BC has increased owing to the increased presence of risk factors such as family history, obesity, smoking, inactivity, hormonal replacement therapy, and early menstruation (Rabbani et al., 2017). In the United States, one out of eight American women is diagnosed with BC (Guilford et al., 2017). In Africa, BC affects 1.16 per 1,000 women annually (Adegbenro et al., 2014). It is also reported that 52 per 100,000 women in Japan and South Korea and 34.86 per 100,000 women in Malaysia have BC (Akhtari-Zavare et al., 2015). Available literature from the Middle East shows that the incidence of BC is 21.3 per 100,000 women in Jordan, 21.4 per 100,000 women in Iran, and 24.1 per 100,000 women in Turkey. Among Gulf countries, Qatar has the highest incidence of BC after Bahrein and Kuwait (Donnelly et al., 2014).
Review of the Literature
In Arabic countries, younger women tend to be diagnosed with BC in advanced stages (Donnelly et al., 2014). In Oman, Omani women are mostly diagnosed with BC in advanced stages, accompanied with poor prognosis. Despite breast-conserving surgery and chemotherapy, the 5-year survival rate is only 64%, which is lower than that in other countries (Al-Moundhri et al., 2004). The American Cancer Society has announced that the survival rate for BC is 93–100% if the disease is detected at an early stage but 22–72% if it is detected at an advanced stage (Akhtari-Zavare et al., 2015). Therefore, screening to detect this disease using methods such as mammogram, breast clinical examination, and breast self-examination (BSE) is essential.
Early diagnosis of BC is associated with a higher tendency for survival and, consequently, a good quality of life (Marzouni et al., 2015). Accordingly, BSE should be performed every month regularly by women to detect any abnormal changes in the breast (Ayed et al., 2015). This technique is safe, non-invasive, inexpensive, and easy to perform (Birhane et al., 2015). According to the American Cancer Society, BSE should be practiced from the age of 20 years (Nemenqani et al., 2014) to detect abnormalities in the breast (Ameer et al., 2014). Regular BSE leads to enhanced awareness of the normal breast structure and easy recognition of any abnormalities; thus, changes can be reported to health services at an early stage (Birhane et al., 2015; Chowdhury et al., 2016).
Knowledge about BSE is considered a cornerstone for the early detection and effective management of BC. Akhtari-Zavare et al. (2015) presented the lack of knowledge as the major barrier toward practicing BSE. Previously, 16 studies with 5,743 participants estimated the pooled prevalence of BSE practice to range from 0% to 26.4%. This finding shows a low uptake of BSE (Kassie et al., 2021). Moreover, there is a positive correlation between the performance of BSE and diagnosis of BC (Nde et al., 2015). Women either poorly perform BSE or do not perform it at all (Akhtari-Zavare et al., 2015). When women do not have adequate knowledge on BC, including its screening methods, BC may not be detected and treated at an early stage. Therefore, BSE must be encouraged for early detection and management of BC (Abolfotouh et al., 2015).
Although BSE is inexpensive, safe, and easy to perform, there are some obstacles women face while performing it (Ameer et al., 2014). Available literature shows the lack of privacy, long procedure duration, fear of being diagnosed with BC, and feeling of embarrassment in performing BSE as the barriers to performing BSE (Abolfotouh et al., 2015; Akhtari-Zavare et al., 2015; Ameer et al., 2014). Other studies in the Middle East have reported that the performance of BSE can be affected by the lack of knowledge and absence of BC symptoms (Akhtari-Zavare et al., 2015; Marzouni et al., 2015). Cultural barriers also play a role in BC diagnosis among older Chinese-American women: Cultural factors influence the initiation of cancer screening behavior (Tang et al., 2000). Additionally, Vietnamese women, who have been reported to have the lowest health literacy level, are not likely to perform BSE regularly (Armin et al., 2014).
The overall knowledge of the risk factors, symptoms, and screening methods of BC, including BSE is low among female Omani teachers (Al-Ismaili et al., 2020). Another study revealed that there was a lack of awareness and knowledge on BC symptoms among Omani women (Renganathan et al., 2014). Considering the increased prevalence of BC and lack of knowledge on BC in young Omani women, it is important to assess the health beliefs on BSE to understand the need for enhancing awareness and self-care and preventive practices. Therefore, this study aimed at predicting BSE behavior among Omani undergraduate students using Champion's Health Belief Model Scale (CHBMS).
Methods
Design
A descriptive cross
Research Question
Can the BSE behavior of Omani undergraduate students be predicted using CHBMS?
Population
The population of this study consisted of female undergraduate students aged 18 years and above studying in Sultan Qaboos University, Oman. This population was targeted because students come from different regions of the Sultanate of Oman and are thus representative of all social and cultural diversities in the country.
Setting
This study was conducted in all nine colleges of Sultan Qaboos University. The university is located in the Muscat governorate in the Sultanate of Oman. Sultan Qaboos University was established in 1986 and currently runs the following nine colleges: Colleges of Medicine; Engineering; Agriculture; Education; Science; Art; Law; Nursing; and Commerce and Economics. The total number of female undergraduate students studying from 2018 to 2019 at Sultan Qaboos University was 8,151. The participants were recruited from all nine colleges.
Inclusion and Exclusion Criteria
Students who met the following inclusion criteria were included in the study: female sex; undergraduate education at Sultan Qaboos University; age of 18 years and above; active registration in the current semester; and ability to read and write in Arabic or English. Students who had been previously diagnosed with BC were excluded from the study.
Sample Size and Sampling Technique
The sample size was calculated using Slovin's formula: n = N/(1 + N.e2). The calculated sample size for the study was 381 female undergraduate students. Convenience sampling was used to select the students from January to December 2019.
Data Collection Instruments
Section 1: Demographic Variables
The following demographic variables were evaluated: age, college, academic year, region, marital status, family history of BC, previous exposure to information on BC, and sources of information about BSE.
Section 2: Health Beliefs Toward BSE
The health beliefs toward BSE were predicted using CHBMS. CHBMS is a commonly used instrument for measuring susceptibility, seriousness, benefits, barriers, confidence, and motivation associated with BC and BSE. This tool consists of six concepts: perceived susceptibility to illness, perceived seriousness of illness, perceived benefits for the presumed action, perceived barriers for the presumed action, confidence in one's ability, and health motivation. Herein, perceived benefits for the presumed action (six items), perceived barriers for the presumed action (six items), and confidence in one's ability (11 items) were used. All items have five response choices, ranging from strong disagreement (1 point) to strong agreement (5 points). The Cronbach's alpha for CHBMS ranges from 0.75 to 0.93. The Cronbach's alpha for the concepts used in our study was as follows: 0.80 for benefits, 0.88 for barriers, and 0.88 for confidence (Champion, 1999). Permission to use CHBMS was sought and granted by the original authors.
Pilot Testing of the Study Instrument
The instrument was pilot tested in 40 participants (10% of the sample size) who met the inclusion criteria. This pilot testing helped in understanding the clarity of the instrument and the time required for conducting the study. The participants in the pilot testing did not participate in the main study.
Ethical Considerations
The study proposal was submitted for review and approval to the Research and Ethics Committee of College of Nursing, Sultan Qaboos University. The consent form, which included an explanation of the study purpose, procedures, risk, rights, and benefits, was signed by the participants. The study did not collect any personal identifying information. The participants were given the freedom to ask any questions before participating and informed that they could withdraw from the study without any coercion. Moreover, the study posed no major risks to the participants. The data were kept confidential under lock and key by the principal investigator of the study.
Data Collection
After obtaining approval to conduct the study, permission was sought from the deans of all nine colleges of Sultan Qaboos University. The investigators pre-visited the colleges to meet the accountable person and arrange for the data collection. During data collection, the investigators visited the colleges and collected data from the available participants who met the inclusion criteria. Students who agreed to participate in the study signed the informed consent form after the explanation on the study procedures and participant rights. After the participants returned the questionnaire, the investigators ensured that the questionnaire was completely filled in and that there were no missing data. The completed questionnaire was then stored, and the data were entered into a password-locked Statistical Packages for the Social Sciences (SPSS) data file.
Data Analysis
The SPSS software program version 24 was used to manage and analyze the data. The computerized data were compared with the original data to ensure that the data were entered accurately. During data cleaning, the investigators ensured consistency, eliminated errors, and checked the values of the variables. Missing data and outliers were monitored using a frequency table. Descriptive statistics such as frequencies, percentages, means, and standard deviations (SDs) were used to describe the participant characteristics and health beliefs on BSE.
Results
Sample Characteristics
Table 1 shows the frequency and percentage distributions of the demographic variables of the Omani undergraduate students. A major proportion (48.6%) of the students were aged 20–21 years. Most (27%) students were enrolled in the College of Science. Approximately 20.2% and 19.7% were from Al Dakhiliyah and Muscat governorate in the Sultanate of Oman, respectively. For the academic year, 26.8% of the participants were in their fourth year of study. Approximately 93.7% were married, and 15.5% reported that they had a family history of BC. Among them, 4.5% and 11% indicated that BC was diagnosed in their first- and second-degree relatives, respectively. A large proportion (87.9%) of the students indicated that they had heard about BSE. Approximately 36.7% acknowledged that they had performed BSE; in particular, 22.83% confirmed that they performed BSE 1 month prior to the study. Approximately 33.1% and 24.4% of the students mentioned that they had heard about BSE through mass media and medical teams, respectively.
Frequency and Percentage Distribution of Demographic Variables of Omani Undergraduate Students.

Research Question Results
The health beliefs of the undergraduate students about the benefits of performing BSE are shown in Table 2. Most (44.6%) participants agreed to the statement “When I do BSE, I feel good about myself.” Furthermore, 39.1% of the participants agreed to the following statement: “When I complete monthly BSE, I don’t worry as much about BC.” Strong agreement was expressed by 53% of the participants for the statement “Completing BSE each month will allow me to find lumps early.” The majority (41.7%) agreed that if they complete BSE monthly during the next year, their risk of dying from BC would decrease. Similarly, 44.4% of the students agreed that if they complete BSE monthly, their risk of requiring radical or disfiguring surgery when BC occurs would decrease. Finally, 45.7% of the participants agreed that completing monthly BSE would help them find lumps that might be cancerous before they are detected by a doctor or nurse.
Beliefs of Omani Undergraduate Students About the Benefits of Performing Breast Self-Examination.

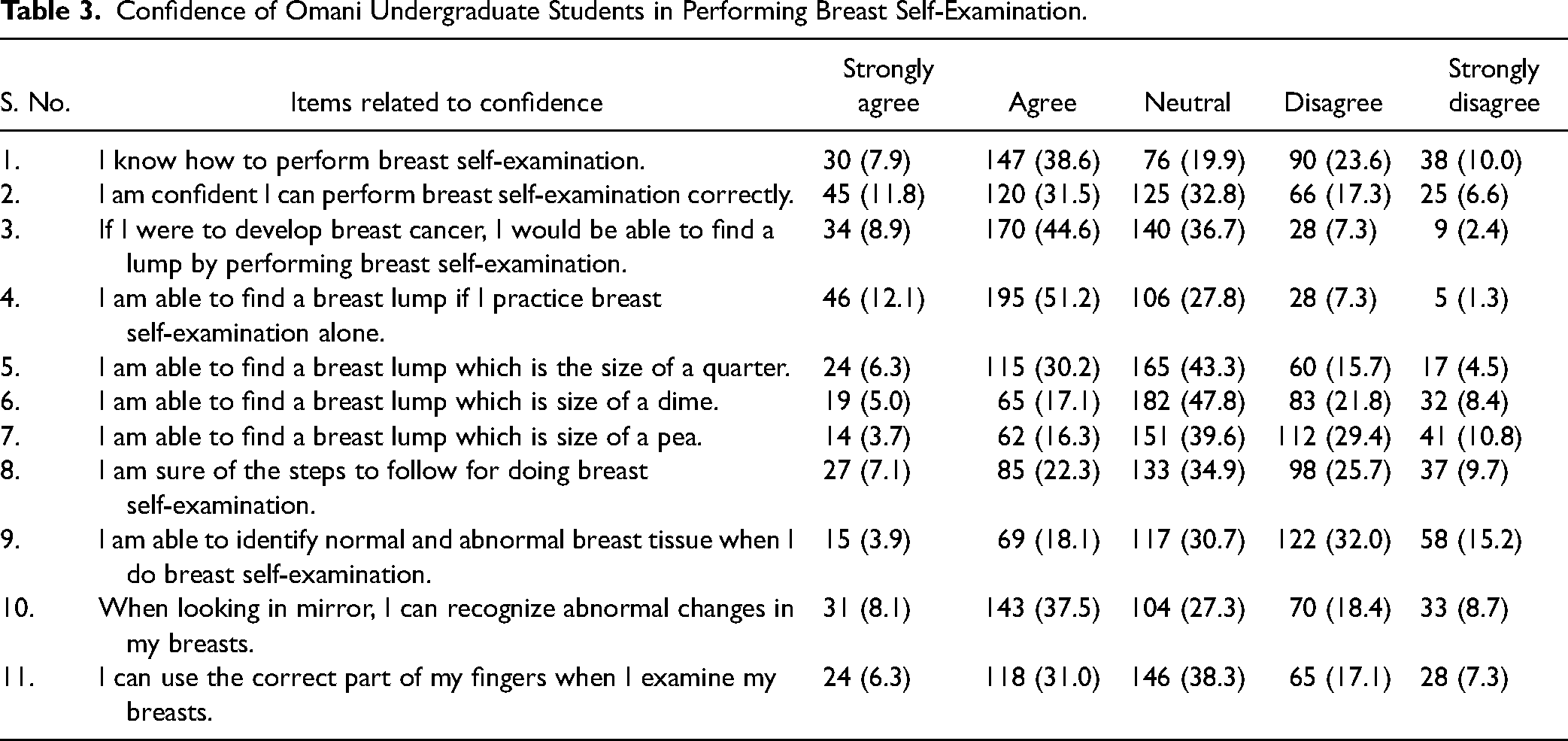
Table 3 outlines the confidence of the undergraduate students in performing BSE. The majority (38.6%) of the students agreed that they know how to perform BSE. Most (31.5%) students indicated that they were confident that they could perform BSE correctly. Furthermore, 44.6% reported that if they were to develop BC, they would be able to find a lump by performing BSE. Approximately 51.2% agreed that they will be able to find a breast lump if they practice BSE alone. A large proportion (43.3%) of the students had a neutral level of confidence and reported that they will be able to find a breast lump that is the size of a quarter. Similarly, a neutral agreement was shown for the statement “I am able to find a breast lump that is the size of a dime” by 47.8% of the students. In addition, 39.6% and 34.9% showed a neutral agreement for the statements “I am able to find a breast lump that is the size of a pea” and “I am sure of the steps to follow for doing BSE,” respectively. Most (32%) students disagreed to the statement “I am able to identify normal and abnormal breast tissues when I do BSE.” In particular, 37.5% of the students agreed to the following statement: “When looking in the mirror, I can recognize abnormal changes in my breasts.” Lastly, 38.3% of the students showed a neutral agreement for the statement “I can use the correct part of my fingers when I examine my breasts.”
Confidence of Omani Undergraduate Students in Performing Breast Self-Examination.
The barriers perceived by the undergraduate students in performing BSE are indicated in Table 4. A vast majority (40.7%) of the students disagreed that they feel funny doing BSE. Moreover, 42.8% and 42.8% disagreed that doing BSE during the next year will make them worry about BC and that BSE will be embarrassing to them, respectively. Most (47.2% and 39.6%, respectively) students did not agree to the statements “Doing BSE will take too much time” and “Doing BSE will be unpleasant.” Finally, 38.8% disagreed that they do not have enough privacy to do BSE.
Barriers Perceived by Omani Undergraduate Students in Performing Breast Self-Examination.

The mean and SD values for the health beliefs of the undergraduate students about the benefits of performing BSE are shown in Table 5. The highest mean (2.09) and SD (0.9) were noted for the item “When I complete monthly BSE, I don’t worry as much about BC.” Following this, a mean of 1.87 and an SD of 0.8 were obtained for the item “When I do BSE, I feel good about myself.” The lowest mean (1.60) and SD (0.7) were noted for the item “Completing BSE each month will allow me to find lumps early.”
Mean and SD of Beliefs of Omani Undergraduate Students About the Benefits of Performing Breast Self-Examination.

Table 6 presents the mean and SD values for the confidence of the undergraduate students in performing BSE. The highest mean (3.36) and SD (1.1) were noted for the statement “I am able to identify normal and abnormal breast tissues when I do BSE.” A mean of 3.27 and an SD of 1.0 were obtained for the item “I am able to find a breast lump that is the size of a pea.” Following this, a mean of 3.12 and an SD of 0.9 were noted for the item “I am able to find a breast lump that is the size of a dime.” The highest mean (3.09) and SD (1.1) were also noted for the item “I am sure of the steps to follow for doing BSE.” The lowest mean (2.34) and SD (0.834) were obtained for the statement “I am able to find a breast lump if I practice BSE alone.”
Mean and SD of Confidence of Omani Undergraduate Students in Performing Breast Self-Examination.

The mean and SD values for the barriers perceived by the undergraduate students in performing BSE are shown in Table 7. The highest mean (4.08) and SD (0.9) were noted in the item “Doing BSE will take too much time,” while the lowest mean (3.48) and SD (1.0) were obtained for the item “Doing BSE during the next year will make me worry about BC.” The overall mean and SD values for the benefits, barriers, and confidence among the undergraduate students in performing BSE were 10.84 and 3.2; 13.58 and 4.2; and 56.24 and 10.8, respectively. In general, the mean and SD values for the confidence in performing BSE were higher than those for the benefits and barriers perceived.
Mean and SD of Barriers Perceived by Omani Undergraduate Students in Performing Breast Self-Examination.

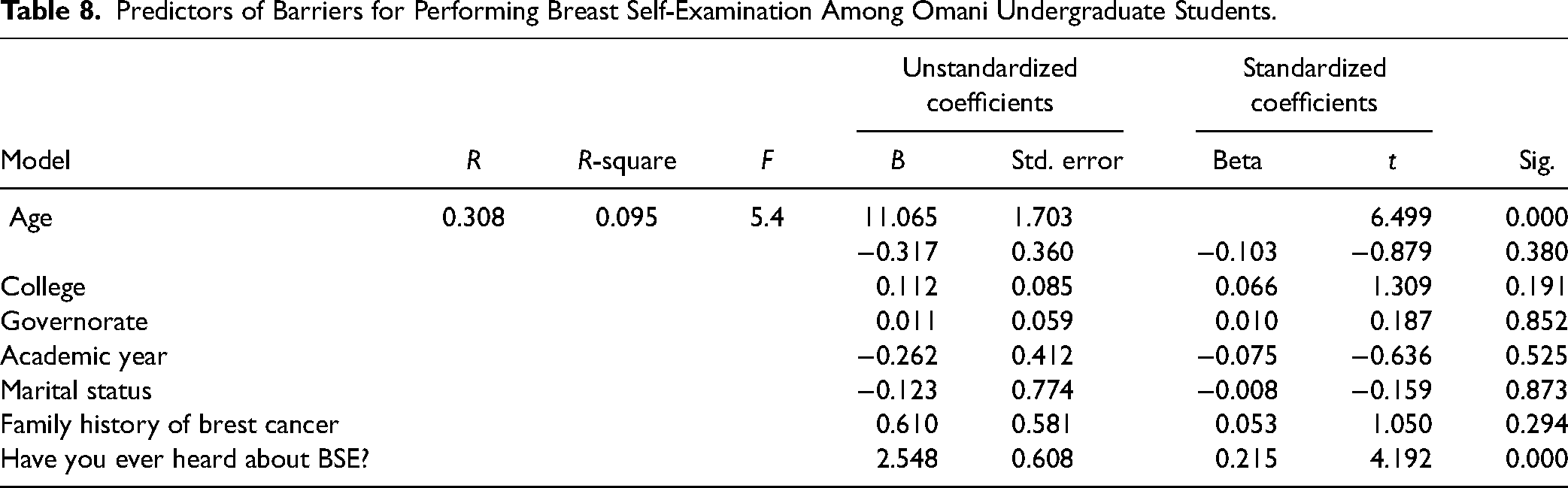
The predictors of the barriers to BSE among the undergraduate students are outlined in Table 8. A multiple regression analysis was performed to predict these barriers. Age, college, governorate, academic year, marital status, family history of BC, and source of information about BSE were identified as the barriers to BSE [F(7, 362) = 5.4, p < .05, R2 = .09]. In contrast, the source of information was found to be a significant predictor of BSE practice (p < .05).
Predictors of Barriers for Performing Breast Self-Examination Among Omani Undergraduate Students.
Discussion
Our study was conducted to predict the BSE behavior among undergraduate students using CHBMS in Oman. A total of 381 female undergraduate students participated in our study. Among them, a few mentioned that they had a family history of BC. Similarly, Brewer et al. (2017) confirmed that the BC risk increases significantly with a higher family history score. Women who have two or more relatives with BC have a 2.5-fold increased risk of developing BC. Therefore, BSE should be encouraged during adolescence to direct younger girls to identify any early symptoms of BC, so that it can be appropriately managed.
Our participants reported that some of their first-degree relatives had BC. Previous studies have confirmed a twofold increased risk of developing BC among women if they have a first-degree relative with BC diagnosed before the age of 50 years (Barnard et al., 2015; Beral et al., 2004; Hemminki et al., 2002; Zipprich et al., 2010). Although family history is a non-modifiable factor, screening programs and counseling services could be utilized by women who are at risk of developing BC.
A large number of the students in our study agreed that they had heard about BSE. Many other studies have also reported enhanced awareness of BC among women (Abo Al-Shiekh et al., 2021; Alam, 2006; Godfrey et al., 2016; Heena et al., 2019; Prusty et al., 2020). Although many studies have confirmed that women typically have adequate knowledge about BC and BSE, two studies (Gebresillassie et al., 2018; Ng’ida et al., 2019) reported that women in Ethiopia and Tanzania had a very low knowledge level on BC and clinical BSE guidelines. Knowledge and socio-cultural and environmental factors were identified as barriers in performing BSE (Akhtari-Zavare et al., 2015). These findings indicate that enhancing the knowledge of women on BC and BSE is highly essential across the world, including developed and developing countries. Efforts to improve the knowledge and practice of BSE are warranted.
Most participants in our study had heard about BSE through mass media and medical teams. Similarly, female university students in other studies have learned about BSE from the internet and social media (Abo Al-Shiekh et al., 2021; Ng’ida et al., 2019). These findings confirm that women learn about BC and BSE from social media, enriching their knowledge and health-seeking behavior.
In our study, less than half of the students confirmed that they had performed BSE and that some of them performed BSE 1 month prior to the study. Similarly, in few other studies, one third of female students and women performed BSE; however, all participants did not practice BSE regularly (Alam, 2006; Aghamolaei et al., 2011; Kim et al., 2019; Lechner et al., 2004; Mousavi et al., 2018; Tavafian et al., 2009). Therefore, our study calls for advocacy and nurse-led educational interventions to improve the knowledge of adolescent girls and women on the importance of performing BSE.
With regard to the health beliefs of the undergraduate students about the benefits of performing BSE, the majority agreed to most statements in our study. Additionally, the participants expressed a strong agreement for the statement “Completing BSE each month will allow me to find lumps early.” The highest mean and SD were noted for the item “When I complete monthly BSE, I don’t worry as much about BC” and “When I do BSE, I feel good about myself.” Previous studies have reported that the perceived benefits and perceived self-efficacy of women who performed BSE are significantly greater than those of women who did not practice BSE (Aghamolaei et al., 2011; Tavafian et al., 2009). Likewise, greater knowledge about BC, greater confidence in performing BSE, and regular visits to a physician are considered significant predictors of practicing BSE (Parsa et al., 2011). Thus, having sufficient knowledge on BC and the benefits of performing BSE will lead to better self-efficacy of women in performing BSE.
Regarding the confidence of the undergraduate students in performing BSE in our study, the majority agreed that they know how to perform BSE; they were confident that they can perform BSE correctly; they would be able to find a lump by performing BSE if they were to develop BC; they will be able to find a breast lump if they practice BSE alone; and they can recognize abnormal changes in their breasts when looking in the mirror. The highest mean and SD were noted for the statements “I am able to identify normal and abnormal breast tissues when I do BSE,” “I am able to find a breast lump that is the size of a pea,” “I am able to find a breast lump that is the size of a dime,” and “I am sure of the steps to follow for doing BSE.”
Previous literature states that women who perceived more benefits of BSE in reducing the severity of BC were likely to report frequent BSE practice. Additionally, women who perceived scarcer barriers in performing BSE and who had enhanced motivation were likely to report BSE practice every month (Dewi et al., 2019; Gray, 1990). Moreover, the frequency of BSE was predicted with professional training on BSE (Kenney et al., 1989; Norman & Tudiver, 1986). Therefore, educational programs that emphasize the perceived benefits of BSE, strategies that enhance the self-efficacy of women, and measures that overcome the barriers in performing BSE are suggested.
In our study, most students disagreed to the statement “I am able to identify normal and abnormal breast tissues when I do BSE.” In contrast, another study reported that participants were able to identify breast pain, nipple discharge, and change in the shape of the breast as symptoms of BC. Moreover, the majority of them had correct beliefs about the management of BC (Gebresillassie et al., 2018). The perceived self-efficacy is the strongest predictor of BSE practice (Noroozi & Tahmasebi, 2016). Therefore, strategies that promote BSE practice are suggested (Nemcek, 1989). However, recent studies are limited in this regard. Further studies are recommended to predict the confidence of women in performing BSE.
Regarding the barriers perceived by the undergraduate students in performing BSE in our study, the majority disagreed that they feel funny doing BSE; doing BSE during the next year will make them worry about BC; BSE will be embarrassing to them; doing BSE will take too much time; doing BSE will be unpleasant; and they do not have enough privacy to do BSE. The highest mean and SD were noted in the item “Doing BSE will take too much time” and the lowest mean and SD in the item “Doing BSE during the next year will make me worry about BC.” Our participants disagreed to most statements regarding the barriers in performing BSE. In contrast, previous studies have reported various other factors as barriers to BSE, including lack of knowledge, absence of any symptoms (Al-Naggar et al., 2011; Hanson et al., 2019; Ng’ida et al., 2019; Tabari et al., 2017), low knowledge level of how to do BSE, busyness (Abo Al-Shiekh et al., 2021), leaving the condition to God (Mousavi et al., 2018), fear of being diagnosed with BC (Al-Naggar et al., 2011; Hanson et al., 2019), and socio-cultural and environmental factors (Akhtari-Zavare et al., 2015). BSE training programs are strongly recommended to reduce these barriers.
Herein, we adopted the following components of CHBMS: perceived benefits, perceived barriers, and confidence in one's ability. The overall mean and SD values for the confidence in performing BSE were higher than those for the benefits and barriers perceived. In general, self-efficacy is important to initiate behavioral change. Therefore, if adolescents are made aware of the benefits of performing BSE, the practice of BSE will be enhanced from adolescence to their lifetime (Anggraini & Gerhanawati, 2021). In our study, the source of information about BSE was a significant predictor of BSE practice. Therefore, various methodologies, including behavioral modification strategies, should be adopted to improve the knowledge on BSE, including the skills in performing such.
Strengths, Limitations, and Recommendations
The generalizability of the present findings is limited, as the study was conducted in only one public university in Oman. Future national-based studies are recommended. The recent literature pertaining to the predictors of BSE is limited. Therefore, further studies are recommended to explore more on the predictors of BSE using the Health Belief Model.
Implications for Practice
Analyzing the BSE behavior of young students in Oman helped in identifying the beliefs, confidence, and barriers in performing BSE. The findings could direct university policy makers in initiating mass educational programs for students on the importance of performing BSE to further facilitate the prevention and early detection of BC.
Conclusion
If the self-confidence of women in performing BSE improves, they will practice BSE more frequently, thereby contributing to the prevention of adverse consequences of advanced stages of BC.
Footnotes
Acknowledgments
The authors acknowledge all the participants of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study proposal was submitted for review and approval by the Research and Ethics Committee of the College of Nursing, Sultan Qaboos University (REC/2018-2019/02).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.