
Abstract
Introduction
Colorectal cancer is classified as the second most prevalent type of cancer among males and females in Jordan; approximately 1260 (10.9%) out of 11559 cases were diagnosed with colorectal cancer in 2020. According to American statistics, colorectal cancer is the third leading cause of cancer-related deaths among both males and females, as well as the second leading cause when combining both numbers .
Objective
The current study aimed to assess the effectiveness of chewing gum in reducing postoperative ileus in patients with cancer after colorectal surgeries and evaluate the length of hospital stay (LOS) after colorectal resection, complications, and costs.
Methods
One-hundred twenty-nine patients who underwent colorectal surgeries at a specialized cancer center in Jordan from April 2019 to May 2020 were recruited. After colorectal surgeries, patients were randomized into two groups. The control group (69 patients) received conventional postoperative care; the experimental group (60 patients) was asked to chew free sugar gum over one hour in the morning, noon, and evening until the first flatus.
Result
The passage of the first flatus was significantly shorter in the experimental group (mean 48.02 h) than in the control group (116.45); p = .001. Also, there was a significant difference between both groups according to gender and age.
Conclusion
Chewing free sugar gum after colorectal surgeries can significantly improve the recovery of bowel motion by accelerating the time to first auscultation to bowel sounds, the first passage of flatus, and reduction in the LOS, which went in agreement with many studies. However, chewing gum is considered a safe, cheap, and practical method to reduce ileus.
Introduction
Colorectal cancer is classified as the second most prevalent type of cancer among males and females in Jordan; approximately 1260 (10.9%) out of 11,559 cases were diagnosed with colorectal cancer in 2020 (World Health Organization, 2020). According to American statistics, colorectal cancer is the third leading cause of cancer-related deaths among both males and females, as well as the second leading cause when combining both numbers (American Cancer Society, 2022).
Colorectal surgery is one of the treatment options for colon cancer; the number of colorectal surgery has also been elevated, regardless of laparoscopic or open resections. It is associated with paralytic ileus, a temporary cessation of bowel movement after a surgical procedure, including abdominal or colorectal procedures (Lee, 2009), Ileus occurs in 10–20 percent of patients undergoing elective gastrointestinal surgery, Chapman and Thorpe (2019) and commonly occurs after abdominal surgery (Short et al., 2015). Cessation of bowel movement leads to disturbing constipation and may lead to nausea, loss of appetite, and food intolerance (Hasan et al., 2021).
Paralytic ileus spontaneously resolves within two to three days postoperative after sigmoid motility returns to normal. An ileus that persists for more than three days following surgery is termed a dynamic ileus or paralytic ileus (Kalyanwat et al., 2018). Postoperative ileus (POI) is the temporary inhibition of gastrointestinal motility due to non-mechanical causes occurring after abdominal surgery, particularly after handling the bowel; it may result in nausea, vomiting, and anorexia (Roslan et al., 2020).
Review of Literature
Despite the lack of standard clinical definitions, the incidence of POI is reported to occur in up to 1 in 4 patients who have undergone gastrointestinal surgery, making POI arguably the most frequent complication following digestive surgery (Roslan et al., 2020). Moreover, POI can cause abdominal distension, abdominal pain, nausea, vomiting, and delayed return of gastrointestinal motility (Zhang et al., 2017). These problems can delay postoperative recovery, prolong the length of hospital stay (LOS), and increase financial burden (Zhang et al., 2017).
There is a lack of effective interventions to prevent paralytic ileus in clinical practice. Several interventions have been applicable to prevent paralytic ileus, including inserting a nasogastric tube, early ambulation, adequate hydration, and pharmacological therapies such as non-steroidal anti-inflammatory drugs (Shaban & Dieb, 2019). Many researchers following colorectal surgeries studied sham feeding using chewing gum to stimulate intestinal movements through increased vagal stimulation that leads to a release of gastrointestinal hormones and increased pancreatic and duodenal secretions; it was proven safe, easy, and beneficial (Sammut et al., 2021; Shaban & Dieb, 2019).
An analysis of all randomized controlled trials (RCTs) in Medline and Embase between 2000 and 2019 was performed by Roslan et al. (2020). Chewing gum therapy was compared with standard care in treating POI in adults undergoing colorectal surgery. POI incidence was the primary outcome assessed. A secondary outcome included the amount of time spent in the hospital, the length of stay, and the number of deaths. The systematic review included 16 RCTs, of which ten (970 patients) were included in the meta-analysis. Patients using chewing gum had a significantly lower incidence of POI in comparison to those receiving standard care (RR 0.55, 95% CI 0.39, 0.79, p = .0009)). Furthermore, these patients improved significantly in the time to pass flatus and in time to defecate (WMD − 0.47, 95% CI − 0.60, − 0.34, p < .00001). However, neither mortality nor length of hospitalization was insignificantly different (Roslan et al., 2020).
In the second meta-analysis, multiple databases were searched. They included ten meta-analyses that investigated the effectiveness of chewing gum for POI after colorectal resection. The methodological quality of meta-analyses was assessed independently by two investigators using the Assessment of Multiple Systematic Reviews (AMSTAR) tools and Oxford Levels of Evidence, followed by the Jadad decision algorithm for each step. The results showed that The AMSTAR scores varied from 5 to 9, with a median of 7.7. Several studies have demonstrated that gum chewing reduces the time to first flatus, first bowel movement, first bowel sounds, and LOS (Zhang et al., 2017).
In a randomized control trial (RCT), chewing gum was studied in 89 patients with rectal cancer following elective open proctectomy. Chewing gum was administered three times a day to patients in the intervention arm after surgery. The first flatus sound, first defecation sound, and peristalsis sound were the primary outcomes. The time to the first flatus was 49.20 ± 1.42 h in the control group and 42.33 ± 3.46 h in the intervention group (p < .05). Moreover, compared with the control group, the intervention group had a significantly shorter time to defecation (p < .05) (Yang et al., 2018).
Kalyanwat et al. (2018) examined the efficacy of chewing gum in resolving POI in patients who underwent exploratory laparotomy and any intestinal anastomosis as part of an emergency or elective surgery. The patients were placed into two groups of 25 each. In the study group, participants were asked to chew one stick of chewing gum for 30 min four times a day till passing flatus. Between the experimental and control groups, there was no significant change in the appearance of bowel motion, the mean time required to pass flatus, stool passage, or sense of hunger. The study group had a shorter time span in all of these characteristics. In all these variables, the meantime was shorter in the study group (Kalyanwat et al., 2018).
Aim
The current study aimed to assess the effectiveness of chewing gum in reducing POI in patients after colorectal surgeries as an inexpensive and easy intervention to prevent paralytic ileus.
The primary outcome of this study includes the first time of passage flatus post colorectal surgeries. The secondary outcome was to decrease the LOS, postoperative complications, and cost.
Methods
Design
An evidence-based practice project using a RCT design was used to examine the impact of chewing sugar-free gum on bowel movement following colorectal surgery and the development of ileus in patients following colorectal surgery. This type of study prevents selection and allocation bias as well as controls over any confounding variables (Simkus, 2022).
Setting
This study was conducted in the surgical department of a specialized cancer center in Jordan. This center provides comprehensive cancer care in Jordan and receives cancer cases from all over the Hashemite Kingdom of Jordan and the region.
Sampling and Procedure
Study enrollment was done continuously with screening and enlisting patients one day before the operation. The primary investigator obtained informed consent from the participants after accepting the invitation to participate in the study. The study aims, design, benefits, and risks were explained to all participants. After collecting the clinical data, including age, gender, and type of colorectal cancer, the researcher used a computer-based tool to randomly allocate the patients on a 1:1 basis to either standard care plus chewing gum or standard care alone. The principal investigator had special training in data collection procedures to ensure the study's reliability and validity.
Based on the power of 0.8 with a medium effect size and α of 0.05, the sample size obtained was 129 patients who were assigned randomly into two groups. Sixty patients in the experimental group were asked to chew free sugar gum starting 6 h after the surgery, over 1 h, every 8h daily, till the passage of the first flatus. The research team dispensed the gum to the participants, and the assigned nurse and the physician assessed the presence of bowel sounds.
To assure patients’ compliance with free sugar gum, the researchers checked the patients’ compliance at the time of free sugar gum administration. Acceptability of chewing gum was assessed via a brief interview with the patients in the experimental group one day post-operation. They asked about their feelings about chewing gum and whether they had any problems or difficulties chewing it. Researchers assessed compliance by asking participants to record when and how long they chewed each piece of gum. We tested chewing gum post-colorectal surgery as a non-pharmacological strategy to reduce the incidence of the ileus. Sixty-nine patients in the control group received traditional postoperative care. In conventional practice care, there is a lack the effective interventions for the prevention and treatment of postoperative colorectal surgery to prevent ileus.
Inclusion and Exclusion Criteria
The inclusion criteria were adult patients who underwent colorectal surgery, regardless of laparoscopic or open surgery for a benign or malignant tumor. The consent form was obtained from the patients.
The exclusion criteria excluded patients under 18 years old, patients unable to chew gum for any reason such as required mechanical ventilation postoperative or intensive care unit, patients with dentures, etc. Patients were also excluded from the study if they finished the surgery after 4 pm to prevent chewing gum at night because they may feel sleepy.
Ethical Consideration
The Institutional Review Board approval was obtained before conducting this study, patients’ confidentiality was assured, and anonymity was assured for the participants by numerically coding the data collection sheets to identify the participants. A locked file cabinet to store all data was used.
Statistical Analysis
Statistical analysis was conducted using Statistical Package for Social Science (SPSS) version 26. The frequency produced summary measures for categorical variables. One-way ANOVA and t-test were used to compare the mean time of pass flatus per hour based on age, gender, and diagnosis. F-test compares the variance in each group mean from the overall group variance.
Results
Sample charactristtics
Participants in both groups had similar features and demographic, including age, gender, cancer type distribution, and duration of the surgeries. This study looked for the groups from different aspects, such as gender distribution among the two groups but did not have significant differences. The mean age in the chewing gum group was 54.18 and in the control group was 50.68. However, the age distribution and type of colorectal tumor taken into consideration, the mean age for the whole sample was 52 years, so the participants divided, either above or below 52 years, to find other factors affecting the time to pass flatus.
Research Question Result
The pass flatus in the participant in the chewing gum groups was more efficient in the interventional group compared with the control groups. The control and experimental groups were comparable according to their demographic data, as shown in Table 1. Paralytic ileus showed a reduction favor to the experimental group and accelerated the time of pass flatus (Table 1). The most efficacy parameter at the end included the first-time pass flatus per hour compared between both groups. The experimental group showed an accelerated time of pass flatus and a reduction in paralytic ileus.
The Time of Passage Flatus Per Hour in the Two Groups.

Table 2 shows a statistical significance difference between both groups regarding the presence of first bowel sounds and the first passage of flatus between both groups according to age divided into below 52 years old and above 52 years old (p < .001).
Comparing the Age of the Chewing Gum Group and the Control Group.

Table 3 shows the differences between male and female distribution in both groups, the male participant was 68 in the whole sample, and the female was 61 with p = .62. In Table 4, the mean time to pass flatus among males in the interventional group (46 h) was less than males in the control group (113.57 h) (p < .001). Similarly, the mean time to pass flatus among females in the interventional group (50.48 h) was less than females in the control group (119.41 h) (p < .001). So, when comparing the male to the female participants in the interventional group, the time for pass flatus per hour was 46 h among males. For the female participant, it was 50 h, so the difference was still in favor of males who chewed gum after surgery.
Gender Differences Between Control Group and Interventional Group.

Time of Pass Flatus Per Hour Based on the Gender of Both Groups.
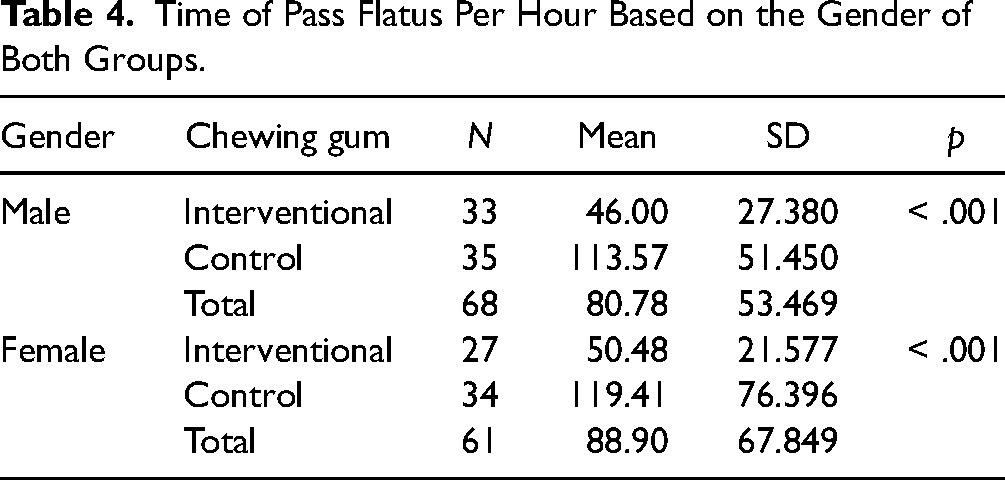
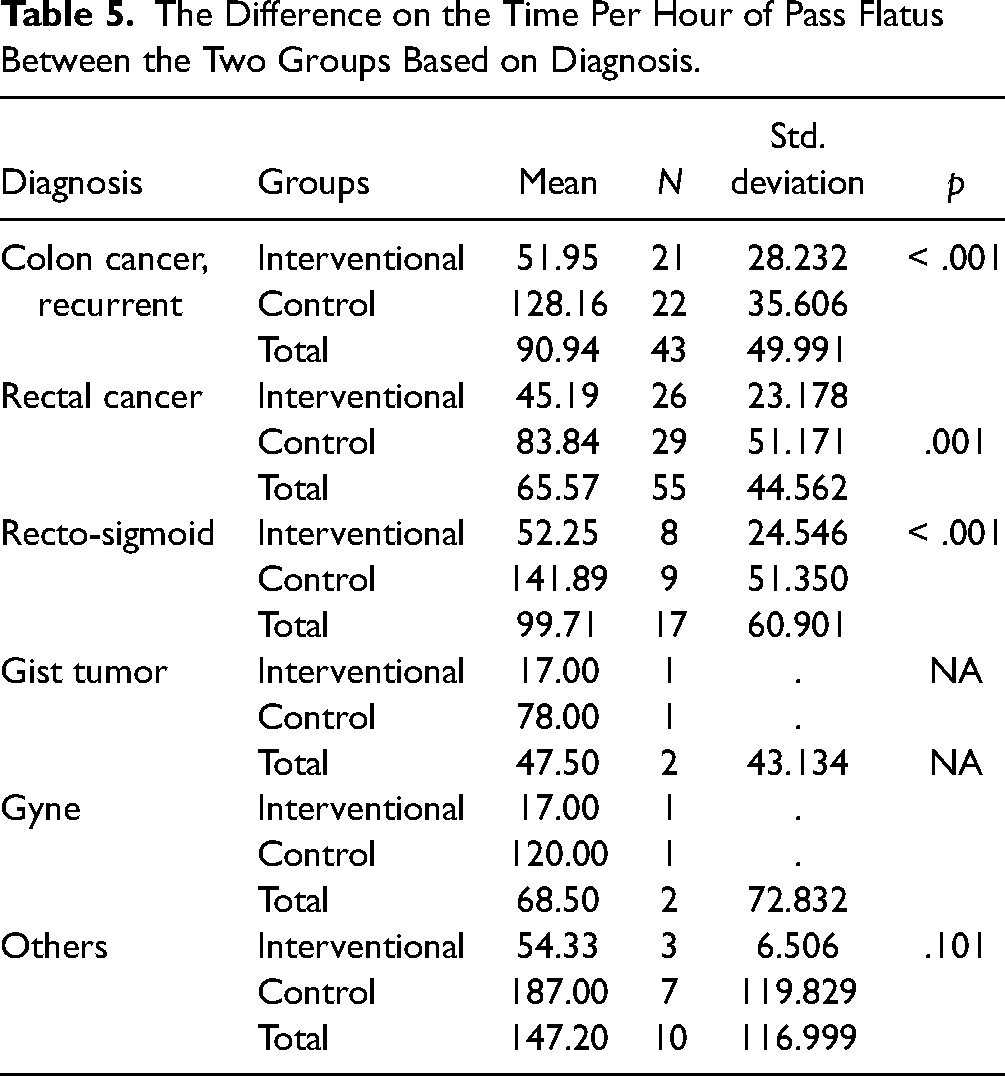
Table 5 shows the sample distribution based on the patient's diagnosis. Based on the diagnosis, there is a significant difference in the time per hour of passing flatus between the two groups. The passed flatus mean among patients with colon cancer, rectal cancer, and recto-sigmoid in the interventional group was 51.95, 45.19, and 52.25 h, respectively, versus 128.16, 83.84, and 141.89 h in the control group (p < .001).
The Difference on the Time Per Hour of Pass Flatus Between the Two Groups Based on Diagnosis.
Discussion
The current study aimed to assess the effectiveness of chewing gum in reducing POI in patients after colorectal surgeries to prevent paralytic ileus. Ileus is one of the most severe complications of colorectal surgery on the surgical floor. It can extend hospital stays, increase medical costs, raise the risk of nosocomial infection, and irritate patients and surgeons.
The results showed that chewing-free sugar gum post-colorectal surgeries were associated with improved bowel movement, decreased ileus incidence rate, and accelerated first flatus time. The flutes are usually the sign of the presence of bowel function that leads to accelerating the start of oral feeding. These findings lead to faster discharge to home and decreased nosocomial infection incidence. Chewing gum is a safe, cheap, and practical method to improve bowel function.
When comparing all previous studies with the current study's findings, this study's results indicated that chewing free sugar gum after colorectal surgery is helpful for the patient's recovery, which was associated with the decrease of the time to first passage of flatus, first bowel movement, early feeding, and the LOS; this is consistent with the most study. Roslan et al. (2020) found that the incidence of POI was significantly reduced in patients utilizing chewing gum compared to those having standard care, without significant differences in the total LOS or mortality. Also, Yang et al. (2018) found that the time of the first flatus and the time to the first defecation was significantly shorter in the experimental group than in the control group. Moreover, according to Shum et al. (2016), chewing gum was not linked to adverse outcomes.
Also, our findings showed that younger patients were more likely to score less time in general, especially in the experimental group, and this finding may be due to several factors, such as the digestive process in older people sometimes slowing down (Charleston, 2022).
Limitation
The primary limitation of the current study was the intervention type. It was challenging for blind participants, and this constraint was identical to that of the majority of prior investigations (Yang et al., 2018). A larger sample is recommended in future studies to generalize the result.
Conclusion
Chewing free sugar gum after colorectal surgeries can significantly improve the recovery of bowel motion by accelerating the time to first auscultation to bowel sounds, the first passage of flatus, and reduction in the LOS, which went in agreement with many studies.
Implication of Practice
Chewing gum is considered as a safe, cheap, and practical method to reduce ileus.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.