
Abstract
Background
Identifying, reporting, measuring, and tracking events provide an opportunity to study system issues, motivate learning, measure the frequency and severity of events, and manage high-risk ones which refer to a safety culture that is focused on valuing the input of working staff and improving the quality of care.
Aim
Enhance the implementation of the occurrence variance reporting (OVR) system at the Obstetrics and Gynecological Hospital in Port Said Governorate, Egypt.
Design
A quasi-experimental research design for one group (pre–posttest) and a mixed-methods approach was conducted in this study.
Method
This study was carried out at an Obstetrics and Gynecological Hospital in Port Said Governorate, Egypt. Study subjects included a convenient sample of 100 doctors and nurses. The study used three tools: OVR Knowledge, Attitude, and Practice (KAP) questionnaire, the OVR trend analysis clinical audit checklist, and barriers that hinder staff to report patient safety events through two open-ended questions.
Results
Significant improvements were detected in the OVR system post-program implementation than pre-program implementation phase. A statistically significant increase in nurses’ and doctors’ total knowledge score from 0.74 to 3.39 and a statistically significant decrease in nurses’ and doctors’ total negative attitude score from 3.87 to 3.27. Also, a statistically significant increase in total practice score from 2.35 to 2.45.
Conclusion
There were significant improvements in the hospital OVR system postprogram implementation than preprogram implementation.
Relevance to clinical practice
To maintain performance and make sure that the original result is not lost, the health care facilities should emphasize the ongoing monthly and quarterly monitoring and analysis of data. Meetings, lectures, and training sessions are used for ongoing education.
Keywords
Introduction
Health care is a complicated industry with numerous risky procedures that demand a lot of work from professionals. The main goal of patient safety is to avoid and reduce the likelihood of danger, mistakes, and injury while receiving medical care. Patient safety is enhanced by strong leadership, commitment, documentation, and a system for staff to report any mistakes (Albarrak et al., 2020). Major reports and studies from Institute of Medicine (US) Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, editors. Washington (DC): National Academies Press (US); 2000. PMID: 25077248.
In Egypt, new universal health insurance (UHI) system was applied to cover all Egyptians by 2032 in line with the UHI law (Ahram Online, 2019). The implementation of the first phase started in Port Said in 2019 with gradual geographic expansion to follow. The Egyptian UHI system emphasizes quality health services and patient safety as a major concern for all modern health care organizations, enhancing the culture of patient safety in all medical facilities, and constructing a system for reporting incidents to be made more adaptable. Additionally, hospitals work to support the creation of quality improvement strategies as necessary taking into account the key concerns influencing the occurrence variance reporting (OVR) system to minimize medical errors and their negative effects on patients, employees, and hospital reputation through continuous monitoring and data collection for analysis (Mathauer et al., 2019).
An occurrence was defined as an unforeseen event that causes or could potentially cause harm to a patient, visitor, and/or employee, including but not limited to: patient or visitor fall or injury, medication occurrences/ medication near misses, adverse drug events, blood and body fluid exposure, mishandling of narcotics, needlestick, and sharp injury, specimen related issues, surgery/invasive procedure-related issues, pressure ulcers or other skin integrity issues, system issues that affect the efficient/ safe delivery of care, equipment malfunction resulting in injury or having the potential to injure, employee work-related injuries and illnesses, unexpected complications or death (Tatum & Kumar, 2021; Tariq et al., 2022).
Significance of the Study
Health care is a dangerous industry because it brings together sick and vulnerable patients with medical services and often complex technology, and necessitates the proper coordination of many workers (Rosen et al., 2018). Human mistake is a risk in any industry with complex processes. One of the most critical difficulties facing health care today is ensuring the safety of everyone who interacts with health services. Patient safety incidents have emotional, psychological, social, and economic effects on families and health care workers; therefore, reducing their frequency and severity is critical (Shaikh, 2018).
Al-Reshidi (2014) advocated for ongoing monthly and quarterly data collection and monitoring to maintain performance and make sure that the original result is not lost due to complacency or failure to adhere to modifications that have been made. Continuing education can be achieved in this way, he continued, through meetings, lectures, patient safety walkarounds, rewards, and commendations given to the highest reporting department, creation of an ideal process flowchart, and distribution of the ideal process flowchart following team member approval. As a result, reporting on occurrence variances is a crucial part of health care management. Underreporting can be caused by several things, such as a blaming culture and unclear information about what and where to report. So, working on strategies to improve occurrence variance report implementation is an important goal for health care organizations that consider quality abases their health care services.
Aim of the Study
This study aimed to enhance the implementation of the OVR system at the Obstetrics and Gynecological Hospital in Port Said Governorate, Egypt through,
Assess nurses’ and doctors’ Knowledge, Attitude, and Practice (KAP) regarding OVRs. Assess barriers that hinder nurses’ and doctors’ willingness to report patient safety events. Analyze hospital OVR data through a retrospective clinical audit. Develop and implement an educational training program on the OVR system based on the preassessment. Investigate the effect of the educational training program on nurses’ and physicians’ KAP regarding OVRs. Evaluate the improvement of the hospital OVR system after program implementation through a prospective clinical audit.
Research Hypotheses
The hypotheses of the study were postulated as follows:
Doctors’ and nurses’ KAP regarding OVRs will be significantly improved by their participation in the educational training program.
There is a significant improvement in the hospital OVR system after program implementation.
Methodology
Research Design
This study used a quasi-experimental research design for one group (pre–posttest). A mixed-methods strategy was employed, in which the researchers combined the collection and analysis of both quantitative and qualitative data. To gain a thorough knowledge of the research problem and the obstacles that prevent nurses and doctors from reporting patient safety events, both quantitative and qualitative data were gathered (Creswell & Plano Clark, 2011).
Doctors and nurses completed self-administered questionnaires about their KAP regarding OVRs, and retrospective and prospective clinical audits used an auditing sheet to review data from OVR forms a year before and after the study to collect quantitative data. Two open-ended questions were used to collect qualitative data about the obstacles that staff members face when reporting patient safety events. The conclusions from the qualitative descriptive portion may be especially pertinent to practitioners and leaders as they create strategies to solve interpersonal and workplace problems that improve the OVR system's implementation.
Setting
This study was conducted at the Obstetrics and Gynecological hospital in Port Said Governorate, Egypt. The hospital follows the Egyptian new UHI system and is one of the main hospitals in the Port Said Governorate which provide specific health services for women and children; the hospital’s bed capacity of 79 beds; includes different departments such as operating theaters, neonatal departments, intensive care units, and intermediate care units, in addition to two departments for natural delivery and sonar and X-ray departments.
Study Participants
For the investigation, a convenient sample was used. The number of nurses and doctors employed by the aforementioned hospital is 95 nurses and 20 doctors in total. Eighty nurses and 20 doctors with at least 6 months of experience and who were willing to engage in the study were eligible and invited to participate. The Raosoft sample size calculator was used to calculate the sample size using the following criteria: There are 20 doctors and 95 nurses in the population, with a margin of error of 5 and a 95% confidence interval, respectively. Therefore, 76 nurses and 19 doctors were the minimum recommended sample size. All 95 questionnaires for nurses and 20 for doctors were given to study participants to guarantee that we got the recommended sample size and to prevent missing data.
Study Instruments
Three tools were used in the following current study:
To achieve the aim of this study, a structured questionnaire was adapted from Alboliteeh and Almughim, 2017. The questionnaire was developed based on the policies, procedures, and manuals of the National Guard Health Affairs NGHA, 2010. It is a self-administered structured and anonymous questionnaire comprising two parts:
Trend analysis is the continuous evaluation of data to find trends that are important for law or medicine (Richard, 1995). Because any occurrence occurs in any hospital department through inspection and analysis of OVR forms using a checklist, the quality department is doing a retrospective and prospective clinical audit analysis of all OVRs submitted. The analysis, is made up of incidents relating to 10 different areas of health care (clinical practice/procedure, medication/wrong, family/visitor/watcher, staff/employee, equipment/supplies, safety, fire/security, behavioral, patient care, and occupational), include the number of reported OVRs, the type of incident, and the reporting department.
Qualitative data were collected through a structured interview using two open-ended questions asking about the barriers that hinder staff to report patient safety events from their perspectives.
From your point of view, what works- or organization-related hurdles prevent you from reporting patient safety events? From your perspective, what other impediments or challenges prevent the reporting of patient safety events?
The hurdles were displayed in frequency and percentages based on the replies’ content analysis.
Fieldwork
This study took 29 months from the beginning of November 2019 to the end of March 2022. The study was implemented in four phases:
Based on the analysis of the results of the assessment phase,
The participants were split up into five groups, each with 20 people. Each group received the intervention throughout four sessions, which included two theoretical lectures and two practical sessions. Each session lasted around 2 h. To accommodate all participant groups, a total of 20 sessions for nurses and doctors were held, with each session lasting about 40 h (a total of 20 h of theoretical lectures and 20 h of practice). The following teaching techniques were used: debate, brainstorming, and interactive lectures. Flip charts, PowerPoint slides, and handouts were used as instructional tools. Lastly, posttest knowledge was completed right away (a multiple-choice knowledge test that was used at the beginning of the program was given again to nurses and physicians at the end of the program; to evaluate the gained knowledge in comparison with the pretest)
Validity and Reliability
Five subject-matter experts evaluated the study materials for translation, face validity, and applicability to the Egyptian culture after they were created in English, translated into Arabic, and reviewed for relevance to the Egyptian culture. Thus, the tools underwent minimal rewording. To assess the tools’ clarity and applicability, as well as to identify potential roadblocks and issues that might arise during data collection without causing a change, pilot research was conducted on 5% of participants and also with hospital employees from various units. With a Cronbach's coefficient alpha of 0.902 for the KAP of doctors and nurses about the OVRs questionnaire and 0.887 for the OVR trend and analysis clinical audit checklist, the tools’ internal reliability was also evaluated, and the results showed that the tool was reliable.
Statistical Analysis and Data Interpretation
Using 2013 released IBM SPSS Corp. (Version 22.0; IBM SPSS Statistics for Windows; IBM Corp., Armonk, New York) software, data were entered into the computer and examined. After ensuring normality with the Kolmogorov–Smirnov test, parametric data were described using the mean and SD. The (0.05) level was used to determine the significance of the data obtained. The authors used content analysis to examine participant replies to the open-ended questions to gather qualitative data. The categories of the responses were then ordered based on the frequency and percentage of each. Fischer’s exact test, Monte Carlo, and chi-square were used for comparing two or more groups of qualitative variables. Wilcoxon signed-rank test was used to compare pre- and postmedian scores and the McNemar's test was used to compare pre and postchange in qualitative variables
Results
The present study is carried out on 100 health care workers (doctors and nurses) to study the effect of the OVR training program in enhancing their application of the OVR system. Eighty nurses and 20 doctors responded to the study questionnaire, with a response rate of 84.2% for nurses and 100% for doctors. The mean age of participants is 35.98 years ranging from 21 to 57 years. Eighty-four percent are females, 53% are working in inpatient departments, and 74% have a diploma degree with a mean experience duration in a hospital is 5.32 years ranging from 2 to 8 years. The mean experience duration in the department is 4.73 years ranging from 1 to 7 years, as shown in Table 1.
Participants’ Demographic and Work-Related Data of the Studied Sample.

Following the training programme, there was a statistically significant rise in overall knowledge scores from 0.74 to 3.39, a statistically significant fall in overall unfavourable attitude scores from 3.87 to 3.27, and a statistically significant rise in overall practise scores from 2.35 to 2.45, as shown in Table 2.
Total Knowledge, Attitude, and Practice (KAP) of Physicians and Nurses Regarding Occurrence Variance Reporting (OVR) System’s pre- and Postintervention.

Table 3 illustrates that the total multiple-choice knowledge test score shows a statistically significant increase after the implementation of the training program from 4.73 preintervention to 7.56 postintervention (p < .001*).
Total Knowledge Scores of pre-and Posttest of Educational Training Program Regarding Occurrence Variance Reporting (OVR) system Among the Studied Sample.

Figure 1 shows the frequency of OVR data in the pre- and postprogram implementation phases. According to the figure, the highest number of incidents had been reported related to most OVR dimensions (equipment/ supplies, safety, fire/ security, clinical practice/ procedures, behavioral, patient care, occupational, and infection control issues) while a low reporting of incidents related to OVR dimensions (medication/wrong, family/visitor/ watcher, and staff/ employee) were significant improvements in the OVR system postintervention.
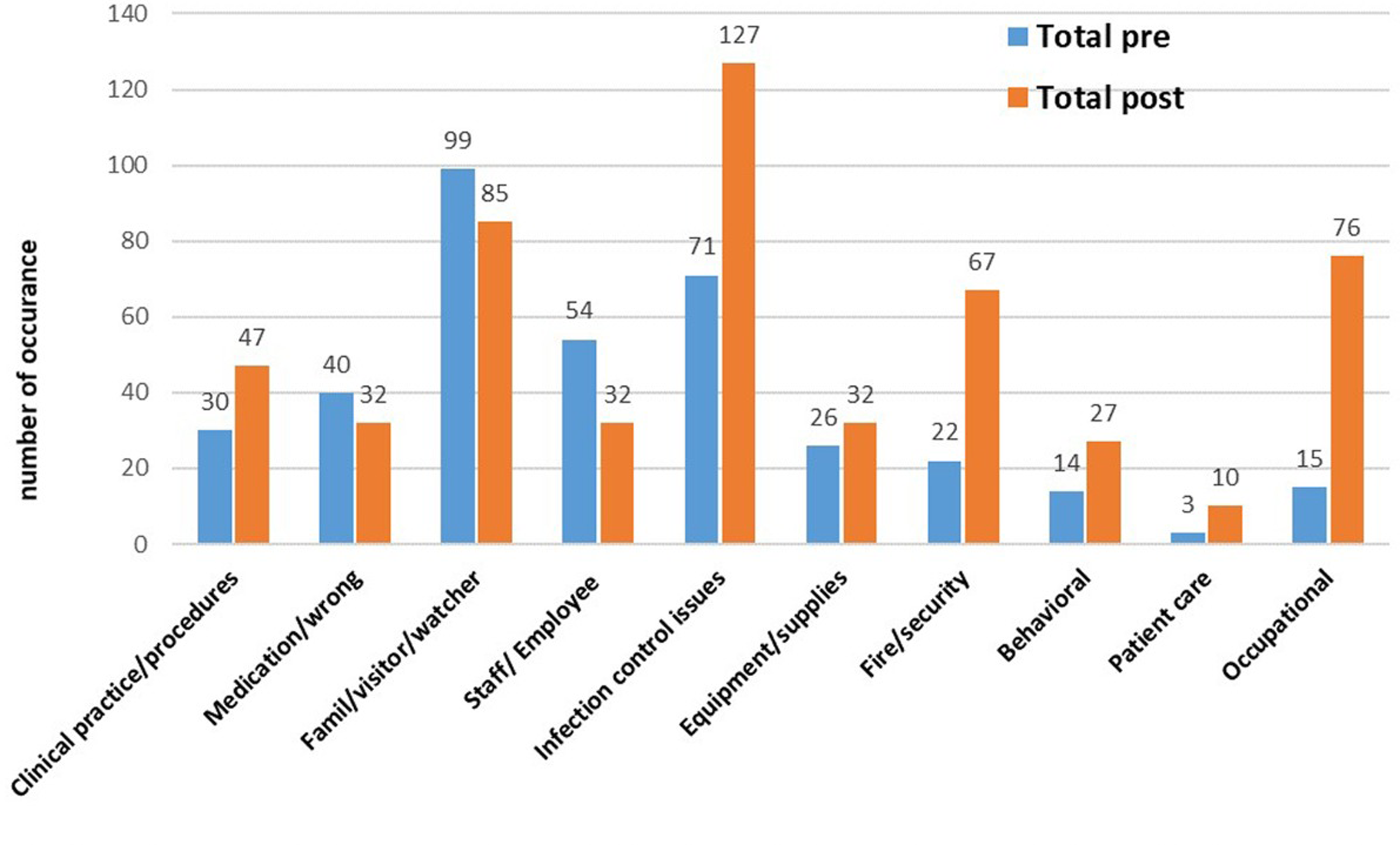
Occurrence variance reporting (OVR) system reported by hospital departments throughout program phases.
Barriers That Hinder Staff Reporting Patient Safety Events From Their Perspectives
The number of participants who answered the open-ended questions about barriers that hinder staff reporting patient safety events was 85 (85%) out of the quantitative sample (N = 100). Two major categories were derived from qualitative content analysis. Participants reported that barriers related to organization/work and barriers related to an individual could hinder reporting patient safety events. Barriers were derived through the content analysis and classified into these two categories. The majority of respondents (n = 78, 91;76.0%) reported barriers related to organization/work including the culture of shame and blame, lack of corrective actions and feedback, high workload, lack of education and training, and lack of management support. In addition, 73 of the respondents (85.88%) identified barriers related to an individual such as worry and fear of blame, stress, insufficient knowledge, skills, and experiences related to OVRs, time consumption, and reports consider as an indicator of incompetence from their perspective (Figure 2).
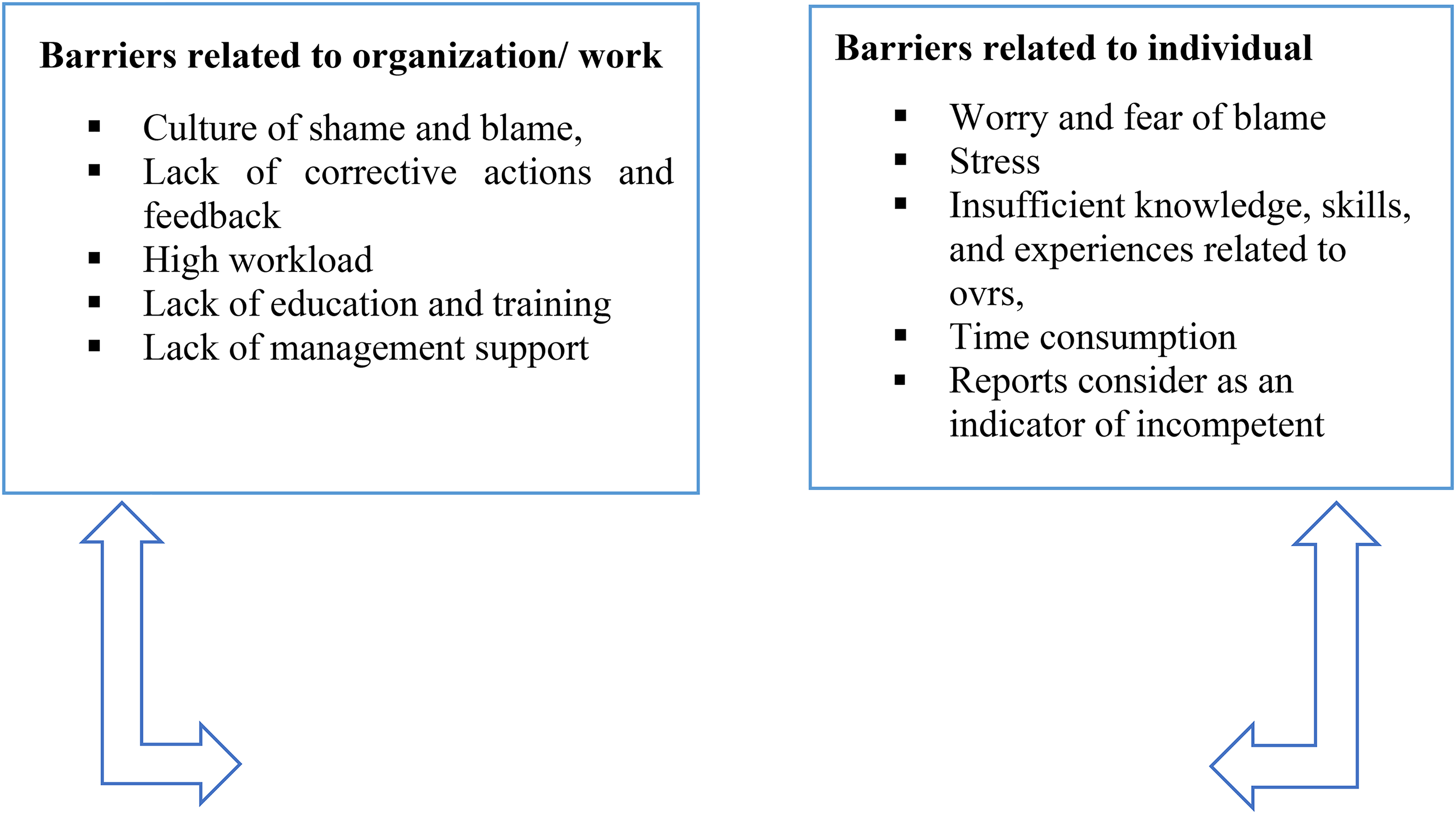
Barriers that hinder staff reporting patient safety events from their perspectives.
Discussion
The present study aimed to enhance the OVR system implementation at obstetrics and gynecological hospital in Port Said Governorate, Egypt. Assessing nurses' and doctors' knowledge, attitudes, practices, and barriers in relation to OVR through the analysis of OVR data, based on the pre-assessment, creating and conducting a training program for hospital staff on the OVR system, and assessing the training program's impact.
The findings of the current study indicated that the OVR system postintervention exhibited considerable improvements in terms of OVR data and analysis. Most incidents had been reported about the majority of OVR dimensions (equipment/supplies, safety, fire/security, clinical practice/ procedures, behavioral, patient care, occupational, and infection control issues), according to the frequency of OVR reporting data in the postprogram implementation phase. While there has been a decline in the reporting of incidents involving (6) compared to preintervention, these improvements may be attributable to the training program's impact on raising hospital staff awareness of the OVR system and its significance for patient, staff, and hospital safety. These findings are consistent with those of Qassim and Al-Reshidi, 2014, who noted a considerable improvement in the OVR system following the implementation of the instructional program. Eldeeb (2010) said that compared to before the educational program was implemented, improvements had taken place. In their study on improving job performance in hospitals, Salem et al. (2022) found that the prevalence variance reporting machine significantly improved after an academic OVR software was implemented in the bodies of staff members and directors. They emphasized that continuous OVR is highly recommended for ongoing monthly and quarterly information gathering and tracking to maintain performance.
About, nurses’ and doctors’ KAP regarding OVR, the findings of the study revealed a statistically significant increase in total knowledge score postapplication of the training program, a statistically significant decrease in total negative attitude score, and a statistically significant increase in total practice score. Also, findings illustrated that the total multiple-choice knowledge test score shows a statistically significant increase after the implementation of the training program from 4.73 preintervention to 7.56 postintervention (p < .001*). This can be understood as the hospital staff being encouraged to report incidents throughout the program because they are not penalized for reporting others, realizing that having an OVR against them won't harm their reputation with coworkers or their annual evaluation and that people who use OVR are not troublemakers. Moreover, they learn to follow the process after filling out an OVR form, starting with their supervisor. According to Althobaiti et al., 2022 study, OVR is important for attaining patient and staff safety, enhancing care quality, and lowering medical mistakes or accidents suggested that medical workers, especially nurses, need to be more aware of the significance of reporting all incidences. Findings from a study by Albarrak et al. (2020) showed that although participants thought reporting took a lot of time, most felt that training-related OVR knowledge and skills were sufficient. Comparatively speaking to nurses, doctors acknowledged having less information about how to access and use OVR. Less than 25% of the staff members didn’t get timely feedback after reporting. Only a quarter of doctors and nearly half of the nurses reported being generally happy with their OVR. This finding is consistent with research by Engeda (2016), who discovered a substantial relationship between training and nurses’ incident-reporting behavior. This result is consistent with Nakamura et al., 2014 study, which showed that after a 6-month educational intervention, the rate of reporting unfavorable incidents increased and that nurses who got the intervention gained greater knowledge and optimism about incident reporting. Robertson and Long (2018) found that failing to disclose increases the risk of serious patient damage. There are strict regulations in place at many health care organizations, which also fosters conflict. Staff may become reluctant to report errors, downplay issues, or even neglect to record them altogether as a result. A cycle of medical errors might develop as a result of these actions or inactions. The reputation of the health care facility and the staff may be damaged if these mistakes are discovered.
A statistically significant relation was detected between poor knowledge score preintervention and lower experience duration in the hospital and lower experience duration in the department; participants with less experience have poor knowledge. The poor practice was statistically significantly higher among the following; males, doctors, and participants with a bachelor's degree. According to the results of Alboliteeh and Almughim, 2017, the knowledge levels of nurses were found to be greater than those of physicians; 57% of both professions acquired their information via the orientation program. More than half of nurses expressed good sentiments about the OVR system compared to virtually all physicians who had negative attitudes. The study of Al Ma’Mari et al., 2022 emphasizes the importance of feedback and communication regarding errors, communication openness, and staff accomplishments since these factors directly affected how frequently events were reported. It emphasizes how urgent it is to discover ways to get rid of the blame culture that develops when mistakes are reported. The study's findings suggest that efforts should be made to improve patient safety and identify additional variables that could have an impact on the frequency of incident reporting. In the same line, Wang et al., 2018 reported that nurses who have more experience perceive higher levels of knowledge related to the importance of OVR.
Concerning barriers that prevent workers from reporting patient safety incidents. The findings of the present study showed two major categories were derived from qualitative content analysis. Participants reported barriers related to organization/work and barriers related to an individual could hinder reporting patient safety events. Where the majority of respondents reported that barriers related to organization/work include the culture of shame and blame, lack of corrective actions and feedback, high workload, lack of education and training, and lack of management support. In addition, 85.88%of the respondents identified barriers related to an individual such as worry and fear of blame, stress, insufficient knowledge, skills, and experiences related to OVRs, time consumption, and reports consider as an indicator of incompetence from their perspective. Kingston et al., 2004 found that lack of time among employees was one of the major problems. Additionally, Banakhar et al., 2017 indicated that barriers included fear of punishment and losing one's job were noted in Saudi Arabia, while fear of penalty was a barrier to reporting in Jordan. Evans et al., 2006 noted several major obstacles that prohibited employees from adopting OVR, such as lack of or delayed feedback and the necessary forms being complicated and requiring mental effort. Alzahrani et al., 2019 claim that several variables, such as resource constraints, teamwork, communication, and incident reporting, hamper the reporting system. Their findings imply that it would be advantageous to put this knowledge to use given the significance of safety atmosphere attitudes for improving favorable patient outcomes. Findings from Ali (2018) suggested that several factors, the most frequent of which is a lack of clarity regarding what to report, how to report it, and where to report it, as well as the presence of a blame culture, may contribute to the underreporting of incidents. It was suggested that working on strategies to improve reporting on patient safety-related incidents is the ultimate goal for health care institutions that considered quality to be the core of their services.
Conclusion
Results showed that the OVR system had significantly improved following the intervention. According to data from OVR reporting that was collected frequently during the pre-and postprogram implementation phases, a significant number of incidents involving (equipment/supplies, safety, fire/ security, clinical practice/ procedures, behavioral, patient care, occupational, and infection control issues) had been reported after the intervention. In contrast to pre-intervention, there has been a low reporting of occurrences involving (medication/wrong, family/ visitor/ watcher, and staff/ employee). Additionally, a statistically significant improvement in overall knowledge score, a statistically significant drop in total negative attitude score, and a total practice score following the execution of the training program.
Relevance to Clinical Practice
Because of the main study findings, the health care facility should provide:
■ Continues monitoring and gathering of data to maintain the performance and ensure that the initial result is not lost through complacency and failure to comply with the implemented changes monthly and quarterly. ■ Continuous education regarding OVR KPA through meetings, lectures, and training programs. ■ Emphasis on the persistency of the integration of OVR into the daily clinical plan of care, and covering the gap between scientific research and plan of care. ■ Empowerment of the culture of reporting, no blame, and the availability of resources for continuity of implementation. ■ Development of OVR practice champions and mentors through rewards and commendations given to the highest reporting department.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Research Ethics Committee at the Faculty of Nursing, Port Said University approved the research with the ethical code (18) (October 2, 2022). Written consent was secured from the director of the Port Said Universal Health Insurance organization with which the hospital is affiliated. And then from the hospital's medical and nursing directors. Written informed consent was obtained from each participant. All of them had the right to refuse to participate or withdraw from the study at any time with no consequences. Additionally, they were informed about their anonymity and the collected information's confidentiality, and it would be used to fulfill the aim of this scientific study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.