
Abstract
Introduction
Nursing personnel are always at risk for work-related musculoskeletal disorders, and patient transportation is one of the major risk factor for these disorders.
Objective
The aim of this study was to evaluate the ergonomic belt to improve patient transferring conditions.
Methods
The subjects included 60 health care workers (HCW) of a hospital with patient transfer experience. The ergonomic belt was examined to help move the patient from one bed to another. The prevalence of musculoskeletal disorders was assessed through the Nordic questionnaire, the degree of perceived exertion through the Borg criterion, and the patient's movement through the MAPO index before and after the intervention.
Results
The results showed a significant decrease in Borg scale scores and MAPO index in two factors of education and auxiliary tools and overall scores of this index. We also saw a significant reduction in musculoskeletal disorders in the neck, shoulders and arms, waist, hands and wrists, thighs, knees and legs. There were no significant differences in the elbow and forearm before and after using the ergonomic belt.
Conclusion
In general, it can be concluded that the use of ergonomic belt had helped to reduce the risk of musculoskeletal disorders, as well as reducing the perceived exertion of nurses and other relevant personnel.
Introduction
Musculoskeletal disorders, or MSDs, are often identified as the biggest health problem faced by industrial workers (Punnett et al., 2004), especially in developing Asian countries (Choi et al., 2005). According to the Occupational Safety & Health Administration (OSHA), most injuries and illnesses among health care workers, including nursing professionals (Alexopoulos et al., 2003; Tinubu et al., 2010), can cause pain in their back and shoulders (Occupational Safety & personal care facilities, 2014). Even the findings suggest that health care workers are at greater risk of developing musculoskeletal disorders than workers in manufacturing, construction, and mining industries (Daraiseh et al., 2010). Injuries due to musculoskeletal disorders cause lost work time and excessive costs; as a result, labor productivity decreases (Ando et al., 2000; Singh, 2018). Patient handling is recognized as the most important risk factor related to work in nursing profession (Caruso and Waters, 2008; Davis and Kotowski, 2015; Marcum and Adams, 2017; Oranye, 2018; Yassi et al., 2013).
An epidemiological study conducted in 2015 in the United States showed a higher incidence of low back pain in nurses compared to different general populations (Davis and Kotowski, 2015). The study of Azizpour et al. (2017) showed that the rate of low back pain in Iran is higher in women than men. In a study conducted by Saberipour et al. (2019), they estimated a lifetime prevalence rate of 82% among Iranian nurses working in hospitals. Factors contributing to the prevalence of these disorders include individual factors, such as high BMI, number of pregnancies and osteoarthritis, and work-related factors including daily frequency of patient transporting and awkward body posture (Boughattas et al., 2017). The high prevalence of musculoskeletal disorders in the nursing profession and their direct and indirect costs indicate the importance of the problem.
Review of Literature
Prolonged standing; awkward posture; use of medical equipment that forces a person to perform movements, such as pulling, pushing and lifting the device; and patient care tasks can all cause discomfort and disorders in musculoskeletal system (Choobineh et al., 2010). The tasks of caring for the patient that can lead to back pain are as follows: changing the patient's position in bed (Smedley et al., 1995), moving the patient between the bed and the wheelchair (Smedley et al., 1995), and helping the patient to change position from lying to sitting on the bed (Freiberg et al., 2016; Karahan et al., 2009). Manual patient handling can generally be defined whenever a patient care provider is directly involved in the patient's transfer, placement, or lifting (Anyan et al., 2013). Studies have shown that in specialized wards of hospitals, the risk of musculoskeletal disorders appears to increase due to the physical load on the lower spine (Nabe-Nielsen et al., 2008). In conclusion, it can be said that the amount of mechanical load on the lower back is very high (Jordan et al., 2011; Skotte, 2001) and the use of ergonomic interventions to reduce this mechanical load is recommended (Koppelaar et al., 2013).
The effect of musculoskeletal disorders, such as low back pain, may be reduced by considering the principles of ergonomics in the workplace, conducting regular individual examinations, identifying risk factors for the development of musculoskeletal disorders and then trying to eliminate them (Azizpour et al., 2017). Identifying nurses and their jobs, identifying the primary factors to assess the prevalence and purpose of effective interventions, can be the first step in this direction (Balogh et al., 2001). Interventions that can reduce the biomechanical load on the user's back and self-reported pain and disability can include the use of ergonomic belts, lifting equipment and small aiding equipment, patient training, multi-component interventions, cognitive behavioral therapy and use of unstable shoes while carrying the patient (Jordan et al., 2011; Richardson et al., 2018).
The handling tool policy is a method in which assistive devices, such as belts, lifts, and other devices, are used to move the patient, and the method of using these tools is given to staff (including nurses). In the case of patient handling tools, previous research suggested that adequate handling tools, and adequate space in patient care units can to some extent prevent MSDs (Krill et al., 2012) and have positive long-term and short-term effects (Elnitsky et al., 2014; Iakovou, 2008). An Ergonomic belt is one of the aids used in moving the patient. These belts are inexpensive and convenient mechanical aids. These devices are placed around the patient's waist and handles are used to lift the patient when transferring them from bed to wheelchair and stretcher, as well as moving them from sitting to standing or vice versa (Nelson, 2001/2005). The use of ergonomic belts, in addition to reducing the pressure on the spine and reducing musculoskeletal diseases, effectively provides comfort to the patients (Yassi et al., 2001). According to Li et al. (2013); ergonomic belts may improve the efficiency of physician work, reduce adverse events, and increase the completeness of physician handoffs. However, further evaluation using rigorous study designs is needed.
Preventive measures must be taken to protect health care workers from mechanical overload. But, more research is needed on the effectiveness of these devices (Jordan et al., 2011). Due to the lack of scientific evidence for determining the efficiency of ergonomic belts during patient transferring tasks and its impacts on musculoskeletal disorders, in this study, we aimed to: (1) determine the efficiency of an ergonomic belt during patient transferring task, (2) and evaluate musculoskeletal disorders among Iranian nurses while using the ergonomic belt.
Material and Methods
Participants
This was a cross-sectional study that was performed on 60 staff members of the ICU of one of the health centers in Tehran. The intended subjects were all employees of a hospital in Iran. Inclusion criteria were that the subject was a nurse or assistant nurse who had a role in patient transferring and also a willingness to participate in the study. All of the participants provided written informed consent.
Data Collection Tools
To collect data, four questionnaires of demographic information, Nordic, MAPO index and Borg criteria were used.
Demographic information questionnaire
This questionnaire contained questions about demographic characteristics (age, sex, height, weight, work experience, marital status, education, history of musculoskeletal disease before starting nursing) and labor organization (type of organizational position, working hours per week, and secondary job).
Nordic musculoskeletal disorders questionnaire
This questionnaire contained questions about neck, shoulder, elbow, wrist, back, low back, thigh, knee and/or leg pain to determine the prevalence of musculoskeletal disorders in these areas (Lei et al., 2005). The participants self-report the level of pain they are experiencing from 1 (no pain) to 9 (unbearable pain). The validity and reliability of the Persian version have been studied in some studies (Mokhtarinia et al., 2015; Namnik et al., 2016). The results of a study showed that the Intra-class Correlation Coefficient and the Standard Error of Measurement of the Persian version of the NMQ-E were deemed acceptable (SEM = 0.56–1.76 and ICC>0.7) and the Kappa coefficient was calculated as 0.78–1.00 (Mokhtarinia et al., 2015). In our study, to evaluate the prevalence of musculoskeletal disorders and the effect of the use of ergonomic belts on its reduction, the Persian version of the Extended Nordic Questionnaire presented by Dowson was used.
MAPO 1 Index
This tool assessed the risk of transferring patients to different work areas, such as hospitals and nursing homes (Menoni et al., 1999). The MAPO tool focuses on factors of work organization, average number of arrests, type of patients, equipment, environmental conditions, and operator training. The final score of the MAPO index is calculated from the combination of the mentioned factors. (Cantarella et al., 2020). In the ISO technical report in 2012, the MAPO tool was mentioned as a useful tool for planning appropriate preventive measures and selecting appropriate equipment (Hignett et al., 2014) and relocation (Villarroya et al., 2016) for different types of patients. MAPO scores can be classified into three different levels of exposure: low (green), medium (yellow) and high (red) (Battevi et al., 2006; Cantarella et al., 2020).
Borg scale
This questionnaire is used for mental exertion. Borg scale has self-report 10 ranks (from 1 to 10), which is the amount of perceived exertion during physical activity (Faulkner and Eston, 2007). The current study examines the amount of perceived exertion by nurses during patient transfer. The amount of perceived exertion to move the patient is divided into the ranks of nothing, very light, light, moderate, high, very high and maximal. In the study of Daneshmandi et al. (2012), the validation of Persian version of this scale in industrial workers based on heart rate were examined. Subjects were assessed by ergocycle test according to Astrand protocol for 6 min. The participants were asked to rate the Borg’s RPE scale during the test at the end of each minute. Additionally, heart rate was recorded by heart rate monitoring device at the end of each minute. Pearson correlation coefficient (r) indicated a high correlation between RPE and heart rate (r = 0.847).
Study Design Method
An experimental study was carried out to design and evaluate the ergonomic belt for patient transferring. This study had been carried out in three main stages, the general stages of which are shown in Figure 1.

Stages and work process.
Stage 1
In this stage, first, basic and demographic information was collected from the sample group. Then, we used MAPO index to evaluate patient transferring. Finally, the prevalence of perceived exertion to move the patient by the sample group was measured using the Borg questionnaire and the prevalence of musculoskeletal disorders was measured using the Nordic questionnaire.
Stage 2
At this stage, the ergonomic belt designed to move the patient (Figure 2) and the necessary training on how to use it was given to the sample group (all 60 participants) and was used continuously for 15 days to perform the task of moving the patient. Each staff received 0.5 to 1 h of training. The training program was provided for each shift. All trials were conducted on the ward, rather than in a laboratory setting.

Image of ergonomic belt.
The ergonomic belt is rectangular in shape with dimensions of 120 × 26 cm and it is made with a strong plastic material. In the middle part of this belt, there are two hard pieces with a length of 50 cm that are used as a fixed and motionless surface on the patient's back and waist and to support it during movement. On each side of the belt, two places are placed elliptically at distances of 10 cm from each other so that the personnel in charge of handling can hold the belt through them and perform the movement action (Figure 2).
How to use this belt was taught to the nurses so that they could place the belt under and behind the patient. First, the patient was placed on one side, then the relevant nurse placed the belt in the desired part to be moved, then the patient returned to its original state. Then, by moving the patient sideways through the ergonomic belt, the patient could be fully supported so that nursing measures could be taken to change the sheets and so on. Also, in cases where there was a need to change position from sitting to lying or vice versa, the patient could be supported by using this belt. The belt was worn for all patient handling by the staff who participated in this study.
Stage 3
Again, the patient's movement was evaluated through the MAPO index, the Borg questionnaire examined the amount of perceived exertion and the Nordic questionnaire examined the effect of the ergonomic belt in reducing musculoskeletal disorders after its use.
Data Analysis
To analyze the data, version 16 of SPSS software was used using descriptive statistics, chi-square and t-test at a significance level of α <0.05 to compare before and after the intervention.
Results
The results showed that 61.1% of the subjects were female and 38.5% were male and the mean age of the subjects was 38.15 years; and, 5.5% had a diploma, 35.5% of the subjects had a post-diploma degree and 59% had a bachelor's degree. Also 23% were single and 77% of the sample were married. The average work experience of the above research subjects was 11.5 years.
The Results of MAPO index
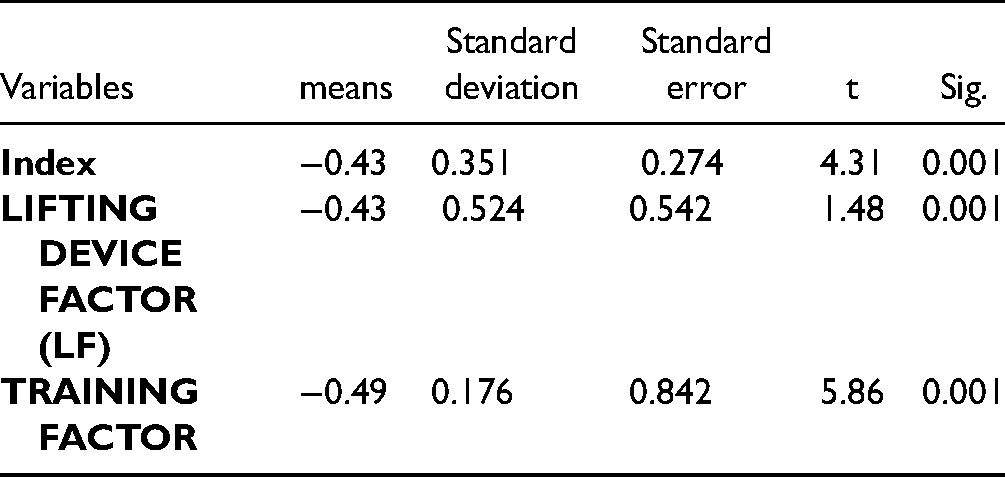
Table 1 shows the MAPO index scores obtained before and after using the ergonomic belts. As you can see in Table 2, the obtained t is at the significance level (0.001). Therefore, it can be concluded that there is a significant difference in MAPO index scores before and after using the ergonomic belt, which is a significant result.
Comparison of MAPO index Before and After Using Ergonomic Belt.

* The value assigned to the LF varies from 0.5 to 4.
** 0.75 = adequate training, 1 = when training simply provided information, and 2 = When no training was given.
*** 0.1 to 1.5 = negligible exposure level (green), 1.51 to 5 = medium exposure level (yellow), and >5 = high exposure level (red).
Correlated t-Test Results to Compare MAPO index Before and After Using Ergonomic Belt.
Results of Borg Scale
Based on the t-test (Table 4), there is a significant difference in Borg standard scores before and after using the ergonomic belt (P <0.001). The percentage of perceived exertion before using ergonomic belt was 71.91% and after using ergonomic belt, it reduced to 48.58% (Table 3).
Borg index Before and After Using Ergonomic Belt.

Correlated t-Test Results to Compare Borg Scale Before and After Using Ergonomic Belt.

Results of Nordic Questionnaire
The results of the Nordic Questionnaire showed that the use of ergonomic belt has the greatest effect in reducing lumbar disorders, and has the lowest effect on the elbow and forearm (Figure 3). According to this questionnaire, there are significant differences before and after using the ergonomic belt in the neck, shoulders and arms, waist, hands and wrists, buttocks, thighs, knees and legs. There is no significant difference in the elbow and forearm before and after using the ergonomic belt (Table 5).

Mean of scores obtained in the NORDIC questionnaire for each part of the body. before and after using the ergonomic belt.
Correlated t-Test Results to Compare Nordic Questionnaire Scores Before and After Using Ergonomic Belt.

* significant values are bold.
Discussion
After an intervention consisting of using an ergonomic belt and training in its use, we observed beneficial changes. These changes included a decrease in mental exertion and musculoskeletal disorders, as well as a significant decrease in MAPO index scores.
Health care workers and especially nursing staff are at risk of musculoskeletal disorders due to the nature of work, as well as the severity of tasks and the intervention of influential factors, such as individual, organizational and work-related parameters (Azizpour et al., 2017; Choobineh et al., 2007; Daraiseh et al., 2010; Davis and Kotowski, 2015; Hignett, 1996; Hofmann et al., 2002; Schneider et al., 2006). In our study, the prevalence of musculoskeletal disorders among nursing staff was high (88.2%). This finding is consistent with the results of other studies (Kim et al., 2012; Nakhaei et al., 2006). Another similar study was conducted by Battevi et al. (2006). They reported that 85.5% of all subjects, that were nurses, were at risk for musculoskeletal injury; of which, 41.5% were at high risk. The findings of the present study showed that in the ICU, where disabled people are hospitalized, the incidence of back pain was high. According to our research findings, the most relevant complaint among the participants was pain in the lumbar region, followed by the shoulder and arm pain.
In a study by Bernal et al. (2015) conducted in the United States, 50 percent of occupational health care workers with low back pain reported adverse effects on their lives. According to various reports, it can be stated that the prevalence of low back pain in nursing staff is due to prolonged standing and activities, such as transferring the patient and constantly changing the patient position from sitting to standing and vice versa (Bernal et al., 2015; Engst et al., 2004). Therefore, principled and practical measures should be taken to reduce and prevent this disorder. According to our study, after using the ergonomic belt, the amount of back pain had decreased significantly.
According to previous studies by Marras et al. (2009) and Santaguida et al. (2005), the main purpose of patient transport assistive devices is only to prevent back injuries during patient transfer. However, the findings of our study showed that the most effective use of ergonomic belt in the prevention of musculoskeletal pain in addition to the back, is seen in shoulder, arm and neck. Also, according to the results of a study by Lee et al. (2013), the use of assistive devices has led to a reduction in shoulder and neck injuries, which is consistent with the present study. In another study by J.Li et al. (2004), the greatest effect of use of mechanical patient lifts in the six months follow up was in the lumbar region and upper back, shoulders and arms.
According to the findings of our study, there is a significant relationship between using ergonomic belts and preventing hand and wrist disorders. In a study on ergonomic assessment of the risk of musculoskeletal disorders due to patient transfer in nursing staff using the Nordic questionnaire, findings indicated that the prevalence of musculoskeletal disorders in nurses was 88.2%, and in particular, the prevalence of musculoskeletal disorders of the hands and wrists was 5.64 (Jensen and Hygiene, 1990). It can be concluded that the prevalence of disorders in this area is considerable and measures should be taken to reduce and control it. In the present study, it was the use of ergonomic belts that could be useful in reducing it.
According to our results, there is a significant relationship between calf, thigh and knee disorders, and using ergonomic belt. Research shows that a risk factor for musculoskeletal pain is when the frequency of transport of the patient is more than 15 times per shift and involves 25 kg or more. Musculoskeletal injuries are reduced by using equipment aids, such as ergonomic belts, in nursing units (Hoogendoorn et al., 2000). The use of patient lifting equipment can be effective in reducing musculoskeletal injuries caused by work in nursing staff in both long-term and short-term care (Evanoff et al., 2003).
Regarding the MAPO index, according to the findings of our study, the influential factors included the assistant tool factor and the training factor, which showed a significant difference in scores before and after using the ergonomic belt. Abedini et al. (2013) in their study stated that the assistant tool factor was not present in any of the hospitals in their study and this could be an important issue in the occurrence of musculoskeletal disorders. Insufficient equipment is one of the most important barriers to motivation and the possibility of using them in medical personnel (Evanoff et al., 2003; Fujishiro et al., 2005; Li et al., 2004). Therefore, having enough equipment to reduce the load is very important; and, the availability of adequate relocation assistance equipment should be included in management policies.
Bewick et al. (2000) reported in their study that one of the reasons for not using patient transfer equipment is the lack of knowledge of nurses about how to use it. Nurses who have received practical training in the use of transfer equipment in their ward or who use transfer equipment frequently have a lower risk of back injuries (Engkvist, 2004). Evanoff et al. (2003) reported that lack of knowledge is an obstacle to ergonomic interventions. In our study, these trainings were given to all participants before working with the belt. Although training seems to be ineffective as an initial preventive intervention to reduce the incidence of low back pain (Hignett, 2003; Martimo et al., 2008), training can be used as a first step to increase knowledge to encourage nurses to use assistive devices (Koppelaar et al., 2013).
Strengths and Limitations
The strengths of this study were the comprehensive evaluation and consideration of various criteria, including the criteria of physical pain, perceived exertion and evaluation of the effectiveness of the ergonomic belt, as well as providing the necessary training for the use of assistive devices.
This study had potential limitations. The study was cross-sectional in nature and assessed respondent perceptions at a short specific time (14 days). The result of this study may not be completely generalizable because the sample size was small. It also is not generalizable to other units in the same hospital. Due to the fact that the population of the study was nurses of a hospital, caution should be exercised in generalizing the above results to nurses in other hospitals. Additionally, the study did not include a quantitative assessment of the risk. The evaluation focused on transfers, not repositioning, and last but not least, the evaluation wasn’t from patient perspective.
Implication for Practice
Despite these limitations, this study supports the theory that using an ergonomic belt is helpful for transferring patients. This study gives valuable information about prevalence of musculoskeletal disorders and perceived exertion before and after using ergonomics belt for patient transfer in nursing staff. These results may also be valuable for those who work with patients suffering from disabilities both in primary care and the hospital setting.
Conclusion
In general, it can be concluded that the use of an ergonomic belt helped to reduce the risk of musculoskeletal disorders, especially in the low back, shoulders and arms, thighs and knees, as well as reduced the perceived exertion of nurses and other relevant personnel. Of course, these results have only been obtained in the study population. Future studies should be performed to examine the effectiveness of using other devices to transport patients in other communities and compare the effectiveness of different devices to each other.
Footnotes
Acknowledgments
The present study is the result of a master's thesis. We would like to express our gratitude to Tehran University of Medical Sciences, as well as to all the dear and hard-working nurses participating in this study.
Declaration of Conflicting Interests
The authors have no conflicts of interest to declare.