
Abstract
Introduction
Family caregivers provide most of the care for older persons living with dementia (PLWD) and multiple chronic conditions (MCCs) in the community. Caregivers experience transitions, such as changes to their health, roles, and responsibilities, during the process of caring. Transitions encompass a time when caregivers undergo stressful responses to change. However, we know little about the transition experiences of caregivers of persons living with both dementia and MCCs.
Objective
This qualitative study explored the transition experiences of caregivers of PLWD within the context of MCCs, from the perspective of both caregivers and practitioners. The research question was the following: What are the transition experiences of family caregivers in providing care to older PLWD and MCCs living in the community?
Methods
This study was conducted using an interpretive description approach. Semistructured interviews were conducted with 19 caregivers of older community-dwelling PLWD and MCCs and 7 health-care providers working with caregivers in Ontario, Canada. Concurrent data collection and inductive data analysis were used.
Results
Caregivers of older PLWD and MCCs experienced four key transitions: (a) taking on responsibility for managing multiple complex conditions, (b) my health is getting worse, (c) caregiving now defines my social life, and (d) expecting that things will change. Findings highlight how the coexistence of MCCs with dementia complicates caregiver transitions and the importance of social networks for facilitating transitions.
Conclusion
The study provided insight on the transition experiences of caregivers of older PLWD and MCCs. MCCs increased the care load and further complicated caregivers’ transition experiences. Health-care providers, such as nurses, can play important roles in supporting caregivers during these transitions and engage them as partners in care.
There are approximately 50 million persons living with dementia (PLWD) worldwide (World Health Organization, WHO, 2019). Most PLWD are 65 years of age or older (WHO, 2019). Many older PLWD require some form of care throughout the disease process, with family or friend caregivers (hereafter referred to as “caregivers”) providing up to 90% of in-home care (Alzheimer Society of Canada, 2010). Caring for an older PLWD can result in negative physical, emotional, and economic consequences for caregivers (Brodaty & Donkin, 2009; WHO, 2019). Caregivers often undergo multiple transitions when caring for PLWD, such as changes to their health, roles, and relationships (Duggleby et al., 2011).
Review of Literature
The presence of multiple chronic conditions (MCCs), defined as two or more chronic conditions, further complicates the transition experiences of caregivers of older PLWD (Marengoni et al., 2009). Almost 70% of PLWD are living with MCC (Bunn et al., 2014; Doraiswamy et al., 2002; Poblador-Plou et al., 2014; Schubert et al., 2006). Research indicates that caregivers of older persons with MCC experience significant stress due to changes in their roles and responsibilities, which can negatively impact their health and well-being (Brémault-Phillips et al., 2016; Ploeg et al., 2017).
Persons experiencing transition processes may be more vulnerable to risks that in turn affect their health (Meleis et al., 2000). Caregivers of older PLWD and MCC often undergo transitions associated with caring for a person with progressive dementia and worsening of other chronic conditions (Bunn et al., 2014; Canadian Institute of Health Information [CIHI], 2011a; Hewitt et al., 2010; Schubert et al., 2006). The presence of dementia and MCC undermines an older person’s ability to engage in self-management behaviors and health maintenance activities (Bunn et al., 2014; CIHI, 2011a; Hewitt et al., 2010; Schubert et al., 2006). Cognitive impairment can affect a person’s ability to take their medications as prescribed, to accurately identify or report symptoms and to manage personal care (Doraiswamy et al., 2002; Eales et al., 2015). Thus, the management of MCC gradually becomes the caregiver’s responsibility (Bunn et al., 2014; Eales et al., 2015). Yet, the responsive behaviors of dementia (e.g., yelling, hitting) can also disrupt the caregivers’ efforts in managing their chronic conditions (Bunn et al., 2014; Feil et al., 2011; Lawrence et al., 2009). Despite the recognized complexity of caring for an older PLWD and MCC, there is a lack of adequate support for caregivers of this population (Bunn et al; 2014; Feil et al., 2011), and care is focused on the patient not the caregiver. In Canada, support for caregivers includes home care services directed at PLWD, which varies from one community to another, as healthcare is delivered by provincial and territorial governments (Public Health Agency of Canada, 2019; Standing Senate Committee on Social Affairs, Science and Technology, 2016). Other supports for Canadian caregivers of older PLWD include respite care, adult day programs, Alzheimer’s Society First Link (a community referral program), and online toolkits (e.g., MyTools4Care, Caregiver Resource Hub; CIHI, 2011b; Public Health Agency of Canada, 2019). Nonetheless, Canadian caregivers still report a need for increased access to resources and supports (Public Health Agency of Canada, 2019; Standing Senate Committee on Social Affairs, Science and Technology, 2016).
While it is important to support older PLWD and MCC, it is also necessary to pay attention to their caregivers, because they are at increased risk for serious illness and mortality (Brodaty & Donkin, 2009). The presence of MCC in the PLWD can negatively affect caregivers’ physical and mental well-being, as they manage more health activities on a daily basis (Bunn et al., 2016). In turn, PLWD have a greater risk of institutionalization when caregivers have poor physical health, low satisfaction with social and community support, symptoms of depression, and high levels of caregiver burden (Mittleman et al., 2006). Therefore, supporting caregivers can promote the well-being of both the caregiver and the PLWD. Health-care providers (HCPs), such as nurses, are ideally positioned to support caregivers through their challenging transitions in caring for older PLWD and MCC (Brémault-Phillips et al., 2016).
There is some literature on the transition experiences of caregivers of PLWD, but we found little on the transition experiences of caregivers of older PLWD and MCC. A qualitative study of 72 caregivers of PLWD and MCC identified three key changes that they experienced including increasing responsibilities, as they take on more personal support tasks and household duties; significant emotional exhaustion and frustration from being a caregiver; and a lack of personal time for themselves (Ploeg et al., 2019). Caregivers of PLWD have been found to experience multiple concurrent transitions throughout the dementia caregiving trajectory; these include diagnosis, the need for formal care at home, placement in an institution, and death and bereavement (Gaugler et al., 2011; Lethin et al., 2016; Montgomery & Kosloski, 2000). According to Lethin et al. (2016), the dementia diagnosis is an unstable time to caregivers, who are still novices and must develop knowledge about caregiving. The progression of dementia, which leads to increased need for formal care and nursing home placement, also challenges caregivers, as they learn how to interact with a fragmented care system and experience increased dependence on care staff (Lethin et al., 2016).
The transition into the caregiver role can have a significant effect on caregivers, who may feel a lack of confidence in their role, as well as increased psychological stress and decreased self-care behaviors (Adams, 2006; Robinson et al., 2011; Schulz & Sherwood, 2008). Across Canada, support offered by HCP to caregivers varies between provinces and territories; support can include case management of home care services, telephone access to dementia care professionals, respite services, and therapeutic skills training for caregivers (Public Health Agency of Canada, 2019). However, little is known about caregivers’ transition experiences when providing care to an older PLWD within the context of MCC. It is important to capture the voices of these caregivers and better understand their transition experiences, as this can inform nurses and other HCP of ways to best intervene and support caregivers during often stressful times. The purpose of this interpretive description (ID) study was to explore the transition experiences of caregivers of older PLWD within the context of MCC, from the perspective of both caregivers and practitioners.
Methods
Design and Research Question
This qualitative study was conducted using Thorne’s (2016) ID approach. ID is an inductive method that addresses clinical questions in order to inform and improve practice. This constructivist approach is founded on the understanding that reality is subjective, constructed, complex, and contextual (Thorne, 2016). The research question was the following: What are the transition experiences of family caregivers in providing care to older PLWD and MCC living in the community?
Setting and Sample
This study was conducted in southern Ontario, Canada. Purposive sampling was used, including criterion and theoretical sampling strategies. Caregivers met the following inclusion criteria: (a) a family or friend caregiver (≥18 years) who provided physical, emotional, or financial care to an older adult (≥65 years) with Alzheimer Disease or related dementias and two or more additional chronic conditions, (b) English-speaking, and (c) had access to and able to use a computer. Theoretical sampling was conducted in the middle phases of data collection and analysis. As patterns and themes were identified from the data, additional participants were sought (specifically male caregivers, working caregivers, and caregivers other than spouses) to achieve a better understanding of the emerging themes.
A small number of practitioners who had worked with caregivers of older PLWD were sampled to complement the understanding of the caregivers’ experiences. Thorne (2016) refers to this as the thoughtful practitioner perspective, which is integral to the ID methodology. Practitioners were eligible if they were currently providing physical, mental, emotional, or psychological support to caregivers of older PLWD and MCC living in the community.
Recruitment
Caregivers were recruited by phone from the Ontario arm of a randomized controlled trial examining the effectiveness of a self-administered online toolkit called MyTools4Care for family caregivers of PLWD and MCC (Duggleby et al., 2018; Ploeg et al., 2018). Participants who provided verbal consent to be contacted for future studies were invited to participate in this study, and all those approached agreed to participate. Participants in the trial were recruited from local branches of the Alzheimer Society in Southern Ontario. Investigators had no previous relationships with participants. Practitioners who worked with caregivers of PLWD and MCC were recruited by phone or email from organizations such as the Alzheimer Society.
Data Collection
Semistructured in-person interviews were conducted by AL, an MSc in nursing student, with caregivers and practitioners from October 2015 to January 2016. All interviews were one-on-one with the exception of one interview where two clinicians from the same organization were present. Most caregiver interviews were conducted in their homes. In cases where caregivers were not comfortable with conducting the interview in their homes (e.g., privacy concerns when older adult also present), interviews were conducted at local cafes. All interviews with practitioners took place at their workplace during breaks or after work hours. A single interview was conducted with each participant and interviews took an average of 60 minutes to complete.
Interview guides (see Table 1) were developed based on the literature review and discussion with research team members, who had experience in conducting research with caregivers, HCPs, and older PLWD and MCC. Field notes were maintained to document details regarding vocal intonations, facial expressions, and gestures not audible on the recording. All interviews were audio taped with permission. Consistent with Thorne’s (2016) approach, data collection ended when the research team had confidence that the complexity and variation of participant responses addressed the research question, with the acknowledgement that there is always more to learn about a topic.
Sample Interview Questions.
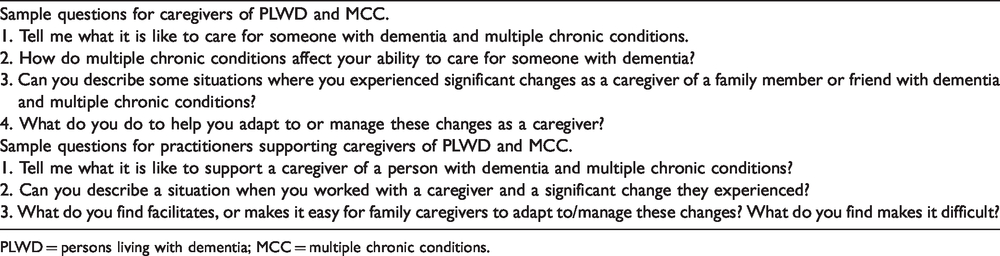
PLWD = persons living with dementia; MCC = multiple chronic conditions.
Data Analysis
Data collection and analysis were concurrent. Data analysis employed an inductive approach where new explanations, concepts, and/or understandings were generated from the data (Patton, 2015; Thorne et al., 1997). All interview recordings were transcribed verbatim and checked for accuracy. Early data analysis consisted of data immersion through journaling and hand-written notes, thus allowing for sense-making of the data as a whole (Thorne, 2016; Thorne et al., 1997; Thorne et al., 2004). During transcription, early patterns were captured through highlighting and memos. Data were later managed, uploaded, and further analyzed using NVivo 10 software.
An initial coding scheme was developed by AL and JP, which evolved as AL continued to collect data and compared codes across transcripts (available on request). An initial coding structure developed through analysis of 15 transcripts was discussed with the research team. Data analysis moved between caregiver’s individual experiences, clinician’s individual experiences, the experience of caregivers, and clinicians as separate groups, and then the entire sample as a whole (Hunt, 2009; Thorne et al., 1997, 2004). Following regular research team meetings with extensive discussion of the results, four main themes related to caregiver transition experiences were identified from the data. These themes emerged from the initial phases of data collection and analysis with the first 8 to 10 participants. A coding structure (available on request) was developed from these themes.
Rigor and Trustworthiness
Trustworthiness of findings was enhanced through the use of strategies addressing the quality criteria of credibility, transferability, dependability, and confirmability (Lincoln & Guba, 1985). Credibility was enriched by including both caregiver and practitioner perspectives and through the use of self-reflection and field notes. Credibility was also enhanced through investigator triangulation by sharing findings with research team members in order to ensure that the initial understanding of themes was consistent. Transferability was ensured by providing detailed, rich accounts of the research process and participants so that readers can make decisions regarding the applicability of the identified themes to their contexts (Lincoln & Guba, 1985). Dependability was maintained by asking participants comparable questions (Creswell & Poth, 2017; Lincoln & Guba, 1985; Patton, 2015). Finally, confirmability was achieved by including participant quotes and staying true to their words and stories (Lincoln & Guba, 1985; Patton, 2015; Thorne, 2016). An audit trail was maintained to track all processes, field notes, and analytical decisions (Lincoln & Guba, 1985; Patton, 2015; Thorne, 2016).
Ethical Considerations
This study was conducted in accordance with the Tri-Council Policy Statement, Ethical Conduct for Research Involving Humans (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, and Social Sciences and Humanities Research Council of Canada, 2018). Ethics approval was obtained from the Hamilton Integrated Research Ethics Board (HIREB #0418). All participants provided written informed consent prior to the interviews.
Results
Demographic Characteristics of Participants
The average age of the 19 caregivers was 68 years (SD = 10.0; Table 2). All caregivers were Caucasian, and most were female (78.9%) and spouses of the PLWD and MCC (57.9%). Most caregivers were retired and had spent on average 4 years as a caregiver. Most PLWD and MCC (47.4%) had from 7 to 10 chronic conditions in addition to dementia. The average age of the seven practitioners was 43.6 years (SD = 9.6), and most were female (85.7%; Table 3). All practitioners worked full-time and had been working in their current position for almost 12 years. Practitioners had a variety of disciplinary backgrounds and worked for organizations such as the Alzheimer Society, outpatient geriatric clinics, and geriatric outreach teams.
Demographic Characteristics of Caregivers (n = 19).

PLWD = persons living with dementia; MCC = multiple chronic conditions.
Demographic Characteristics of Practitioners (n = 7).

Transition Themes
Four themes and corresponding subthemes reflecting transitions experienced by caregivers of older PLWD and MCC were identified. Participant quotations are indicated by the letters C and P for caregivers and practitioners, respectively.
Transition 1: Taking on Responsibility for Managing Multiple Complex Conditions
The first transition experienced by caregivers of older PLWD and MCC was a progressive increase in caregiving tasks and responsibilities associated with the complexities of both dementia and MCC. The accumulation of these responsibilities was often gradual and related to the progression of dementia and other chronic conditions. Caregivers “slid into taking over tasks, very gently, over a long period of time” (C01).
I am managing many medications for multiple health conditions
As their memory deteriorated, the older PLWD and MCC lost the ability to engage in self-management activities such as taking prescription medications. Caregivers ended up taking over; they managed multiple medications, many of which were prescribed for conditions other than dementia and often by a number of different physicians and specialists. There was always a potential risk that the older adult would forget to either take their medications or overmedicate. As such, caregivers developed their own routines to medication management, which involved picking up medications, organizing and preparing them on a weekly or daily basis, and administering or supervising the older adult to take them. Some older adults also had complex medical conditions in addition to dementia that required more intense medication management. For instance, one caregiver described the complexity of managing pain medications: She’s always in pain. She only has the one pain pill in the morning, Dilaudid, and she’s on a [long-acting] pain patch, Fentanyl. […] The Dilaudid, at one point we gave too many and she was lethargic all weekend. […] The pain patch is every three days, but I have trouble remembering that. I try to mark it on the calendar, but I forgot one time and it was a day and a half before I realized it! (C13)
I am always listening to ensure his safety
The second new responsibility that caregivers took on was a constant vigilance to ensure the safety and protection of the older PLWD and MCC. Caregivers were especially concerned about falls and wandering behaviors and were hesitant to leave the older adult alone. Many older adults had at least one other chronic condition that affected their mobility and gait, making them unsteady on their feet. Memory impairment further increased the risk of falls as the older adult sometimes lacked insight into their physical limitations, thus forgetting to use walking aids.
Given that many older adults were prone to wandering, caregivers were constantly aware of their surroundings, ensuring that doors and windows were locked. They were often up at night listening for movement and wandering around the house: “When he is sleeping, I wake up at any noise … It’s totally time consuming because you’re always on it” (C11). Other caregivers had experiences where the PLWD had wandered outside the house and became lost: He’d been gone out of the house for a while. I peek out and see a black car and he’s leaning in it talking to the man. When he came in, he said “Oh, that was the fella who took me home. I guess I made a wrong turn.” … I have to watch him 24/7 or he’ll get lost again. He has been lost three times! (C03)
Transition 2: My Health Is Getting Worse
The second over-arching transition experienced by caregivers was a deterioration in their own overall health and well-being. Caregivers described feeling increasingly tired and depressed. Practitioners described the role of a caregiver as a “sick role,” where “it’s almost like caregivers are accepting these responsibilities; they know this is their role, not realizing that eventually they’re in a sick role because they’re experiencing burnout” (P02).
I’m not sleeping, I’m tired
The “chronicity of being a caregiver and being trapped in the role is very, very difficult” (P04), and many caregivers experienced increasing fatigue. Some caregivers were up every night listening for the older PLWD and MCC, therefore, not getting a good night’s rest. Caregivers who had to provide hands-on care were constantly engaged in repetitive physical movement that increased their fatigue.
Many caregivers also had their own pre-existing health conditions that affected their ability to care for the older adult. Some chronic conditions were associated with recurrent acute exacerbations that made it more difficult to physically meet the demands of caregiving: I recently came through a COPD [chronic obstructive pulmonary disease] exacerbation where I was on antibiotics. I had great deal of difficulty catching my breath doing physical labour. […] So, my chronic condition makes it very difficult to be physically on top of everything … I have to slow down. I’m limited. (C09) I was sitting and my chest was heavy … I called my daughter but she was out. I sat in my chair for who knows how long and kept pumping nitro, trying to keep going, you know? Because I couldn’t leave [my wife] alone! I didn’t know what to do! […] Eventually my daughter came over and she called the hospital … [The] doctor there says, “You’re having a heart attack!” (C17)
I get very depressed
Caregivers also experienced changes to their mental and emotional health. The isolating and constantly changing nature of caregiving meant that caregivers “get very depressed sometimes” (C08). Caregivers were overwhelmed with sadness and loss, as they reflected on who the older adult used to be and how they had deteriorated. Many caregivers were teary-eyed and emotional when reflecting on and speaking about the past: It’s hard for me to see her in this condition. Yeah, it’s really heartbreaking. [sighs, teary-eyed, staring at wife]. It just breaks my heart. Sometimes I feel like going and crying because she’s been such an active, such a wonderful person all her life. (C17) Well, I’m an artist and I can’t paint because I haven’t got enough time. And the sad thing is, for me personally, I find that that’s what fulfills me … And not being able to paint, is part of the problem because [make a fist and holding it to her chest, brows furrowed] I just, I want to get my emotions out and express it! And I can’t! (C14)
Transition 3: Caregiving Now Defines My Social Life
The third major transition experienced by caregivers of older PLWD and MCC was a change in their social lives that were now defined by being a caregiver. As their relationships changed with the older adult as well as family members and friends around them, caregivers found themselves experiencing several shifts in their social boundaries.
I gave up my social life
Many caregivers described how their social lives became more confined. Interestingly, there were varying levels of confinement that depended on factors such as whether the older PLWD and MCC could be safely left alone, whether the caregiver had available support networks or respite care options, and whether the older adult would accept others coming into the home. Spousal caregivers described a very tight level of confinement where they were constantly physically together with the older adult, as described later: He watches me. Like, if I’m in the basement, he shadows me. I turn around and he’s right there behind you. He finds me. I never go anywhere without him because he’s very competitive for my time … I have to wait until he goes to bed at night [to talk on the phone]. He doesn’t want me talking to someone else. (C08)
My social network keeps me sane
Some caregivers developed new positive networks of support, while others found new strengths and bonds within existing networks of support. This helped to expand their world in that caregivers were building relationships with friends and family members who were able to support them, physically or emotionally. Given that caregivers found the emotional part of caregiving the most distressing, talking with others supported them during difficult times: I have a friend and she is my rock. She is my spiritual advisor … I can send her a text message, at any time of day or night … She is my friend. And my advisor. She is one of my branches. And I have another friend who is my other branch. Together, those branches hold me up. They keep me grounded. They keep me sane. (C19)
Transition 4: Expecting That Things Will Change
The final transition was that caregivers were constantly anticipating future changes that would come with their caregiving roles. They felt that as long as the older PLWD and MCC was taking medication and attending regular medical follow-up appointments, they were able to “keep things under control” (C07). Practitioners felt that the lack of a clear disease trajectory put caregivers in a difficult position when they realized that “it’s not going to get any better” (C07), making it difficult for caregivers to plan ahead.
I try to keep her active
As caregivers anticipated the expected deterioration of health status of the PLWD and MCC, they used strategies to maximize mobility and independence while maintaining the older adult’s identity. Some caregivers made a concentrated effort to prevent further functional decline and manage other MCC such as cardiovascular disease: She’s gotta get her out of the chair … Because, the more she gets out of that chair, the more she moves, the better she’ll feel, the better it is for her feet that swell. It’s better for her heart. I try to get her up and moving while she still can. (C09)
I am preparing for the future
Most caregivers had basic knowledge about the progression of dementia and were able to anticipate certain aspects of the future. Regardless of the amount of physical, mental, and emotional preparation for the future, caregivers admitted that it was difficult to determine how long the older PLWD and MCC would remain “stable.” They acknowledged that “[things] will change again; how things are right now is not how they’re going to be a year from now […] he is deteriorating so it won’t remain the same” (C15). In the earlier stages, caregivers often prioritized their caring efforts on dementia rather than other chronic conditions. This was because dementia was often associated with responsive behaviors that were more overt and troubling, such physical/verbal agitation, sleep disturbances, and wandering. Only a few caregivers described the importance of proactively caring for other chronic conditions as a way to address future cognitive changes. One practitioner noted: For example, someone who stopped taking their thyroid medication. Instead of fighting, a lot of families just give up … But, they don’t realize that if they found a way to get him to take the medication, it could help with the thyroid or help with the other chronic conditions which could potentially impact the dementia. (P05) I’m tired of putting mom through tests. There has to be an end to it … At her last doctor appointment we talked about Do Not Resuscitate forms … That’s not easy but I don’t want her to suffer. I feel very, very badly. (C19)
Discussion
Study findings make important contributions to understanding caregivers’ transition experiences in caring for older adults with both dementia and MCC. Study themes are distinct from the themes of a previous study of changes experienced by caregivers of PLWD and MCC (Ploeg et al., 2019). The unique findings highlight the following: how the presence of MCC further complicates transitions, the importance of social networks for facilitating transitions, and the anticipation of health changes in the older PLWD and MCC and planning for the future.
Coexistence of MCC With Dementia Complicates Transitions
Study findings indicate that the coexistence of MCC with dementia adds complexity to caregivers’ transition experiences. Caring for an older person with MCC requires the caregiver to manage multiple medications and appointments with various HCP, and this responsibility can overwhelm the caregiver (Ploeg et al., 2017). In this study, although caregivers were caring for PLWD who also had on average 10 other chronic conditions, their main focus was on the management of dementia, a finding also evident in the literature (Schulz & Martire, 2004). Practitioners discussed the importance of considering other chronic conditions, because if left untreated, they could contribute to the decline in dementia.
There is increasing evidence that demonstrates the link between dementia and common comorbidities among PLWD, such as hypertension, diabetes, and cerebrovascular disease (Bauer et al., 2014; Poblador-Plou et al., 2014). However, caregivers, in this study, seldom recognized that poor management of comorbid conditions could affect cognition as they focused primarily on the dementia. These findings can be partly explained by the public’s limited understanding of the management of risk factors for dementia and related comorbidities (Scrutton & Brancati, 2016). Furthermore, both HCP and caregivers may be unaware of the presence of certain comorbidities, as older PLWD are less likely to receive a diagnosis for other health conditions (Löppönen et al., 2004; Sanderson, 2002; Scrutton & Brancati, 2016). Caregivers unaware of other existing comorbid conditions in the older PLWD are unable to seek and receive the care and support needed to manage these conditions (Bunn et al., 2016; Scrutton & Brancati, 2016). This complicates their experience of transitions, as they may not possess the appropriate knowledge to care for the older PLWD and MCC. This study adds further evidence that caregivers of older PLDW tend to focus on their dementia and overlook coexisting MCC, illustrating the need to educate caregivers about the relationship between dementia and MCC.
The Importance of Social Networks for Facilitating Transitions
The next key study finding was that informal and formal support networks were crucial in supporting caregivers during transitions. The literature, however, reveals mixed findings in relation to caregivers’ perceptions of support networks and their willingness to seek help (Adams, 2006; Donnellan et al., 2015; Sanders, 2007). Studies have found that caregivers of PLWD may be ambivalent about seeking or accepting help from others (Adams, 2006; Donnellan et al., 2015; Sanders, 2007). In some cases, caregivers are reluctant to ask for assistance because they feel that family and friends do not understand the extent of the problem or may criticize them, resulting in negative relationships and emotions (Adams, 2006; Sanders, 2007). This study also found that within the context of dementia and MCC, some caregivers had family members and friends who withdrew from them, leading to increased feelings of confinement. Nonetheless, the findings also demonstrate that social support networks remained important in supporting caregivers during transition times. Formal supports, such as respite care and community networks (e.g., Alzheimer’s Society) were also critical to caregivers’ self-care. In fact, research has shown that support groups help caregivers overcome social isolation and facilitate resilience (Donnellan et al., 2015; Sörensen et al., 2006). Thus, this study’s findings illustrate that informal and formal supports are essential to assist caregivers of older PLWD with MCC with transitions.
Anticipating Health Changes in the PLWD and MCC and Planning for the Future
The final key finding indicated that caregivers anticipated changes in the health and function of the older PLWD and MCC, and they started to plan for the future. In the early phases of caregiving, it is not uncommon for caregivers to experience uncertainty regarding what the future holds (Dupuis, 2002). A systematic review by Bunn et al. (2012) found that caregivers described the struggle between living in the present and having to deal with the anxiety surrounding preparing for the future. This is consistent with the findings in this study, as caregivers described a tension between wanting to prepare for the future, but at the same time, holding back the expected. Consistent in both a systematic review (Bunn et al., 2012), as well as this study, was that as chronic conditions progress, caregivers transitioned from focusing on delaying disease progression to actively planning for future care. However, this study’s findings also demonstrate that when caregiver participants discussed the future, few considered the impact of MCC on the older adult’s cognitive and functional status near the end-of-life. Literature shows that decision-making regarding treatment and care in dementia is different than that of other chronic diseases, as persons with MCC (without dementia) may have more time to consider options and make conscious choices over time (Bunn et al., 2016; Wolfs et al., 2011).
Strengths and Limitations
One strength of the study was the inclusion of varied caregivers in relation to age, relationship with the care receiver, and length of time caregiving. This diversity increases the transferability of results to similar populations. Another strength involves the integration of multiple sources of data (e.g., caregivers and practitioners), which enhanced study credibility (Thorne, 2016). The inclusion of practitioners, the use of an interpretive design, and the use of a theoretical perspective (transition theory) were unique aspects of this study in comparison to a previous study of changes experienced by caregivers of a similar population (Ploeg et al., 2019). A study limitation was that most caregivers were female, Caucasian, and English-speaking, which limits the transferability of the findings to other populations.
Implications
Multiple practice implications can be drawn from these study findings. First, it is vital that HCP, such as nurses, understand the complex transition experiences of caregivers of PLWD and MCC, assess their needs for support, and take appropriate action to address those needs. Maintaining communication in a timely and sensitive manner with caregivers can decrease feelings of uncertainty and frustration (Gill et al., 2014). Education of caregivers related to the interconnections between MCC and dementia are important. For instance, stroke, diabetes, hypertension, and atherosclerosis are common dementia risk factors (Bauer et al., 2014; Sahathevan et al., 2011). HCP can play important roles in facilitating access to health and social care services that can support caregivers through transition experiences (Kuluski, Peckham, et al., 2019). It is recommended that HCP routinely engage caregivers in decision-making and acknowledge their role as key partners in the care of the older PLWD and MCC (Kuluski, Kokorelias, et al., 2019; Kuluski, Peckham, et al., 2019). Finally, HCP should assist caregivers in planning for the future in a manner that reflects caregivers’ priorities and beliefs (Kuluski, Peckham, et al., 2019). HCP should engage in early discussions regarding advance care planning with caregivers and the older adult themselves.
Future research is needed to understand the transition experiences of certain groups of caregivers of older PLWD and MCC (e.g., males, working caregivers, and people of different cultures). Future research should also explore the impact of the social determinants of health (e.g., income, social support) on transition experiences of caregivers of older PLWD with MCC (Northwood et al., 2018). These experiences should be considered within the context of MCC, as it reflects the reality for most persons with dementia and adds an important layer of complexity influencing caregivers’ transition experiences.
Conclusion
The study findings provide a new in-depth understanding of the transition experiences of caregivers of older PLWD and MCC. The presence of MCC adds to the already heavy load of caring for PLWD and intensifies the complex transitions caregivers experience. As the population of older adults living with dementia and MCC increases, and the health-care system continues to shift the burden of care to the community, family, and friend caregivers are expected to address their multifaceted care needs. However, caregivers are particularly vulnerable, as they move through caring transitions and require support. HCPs, such as nurses, can play key roles to help caregivers through these transitions and include them as full partners in care planning.
Footnotes
Availability of Data and Materials
The datasets analyzed during the current study are not publicly available due to the lack of consent from study participants to share the data beyond the study.
Acknowledgments
The authors thank the caregivers and practitioners who participated in this study.
Authors’ Contributions
A. L., J. P., S. C., W. D., and C. M. designed this study. A. L. completed data collection. A. L., J. P., S. C., W.D., C. M., and P. J. contributed to data analysis. J. P. and P. J. wrote the first draft of this article, and all authors reviewed and contributed to revisions of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by The Alzheimer Society Foundation of Brant, Haldimand-Norfolk, Hamilton, and Halton. This work was supported by a program of research (Aging, Community and Health Research Unit, School of Nursing, McMaster University) funded by the Canadian Institutes of Health Research Signature Initiative in Community-Based Primary Healthcare (![]() ; funding ref. no. TTF 128261).
; funding ref. no. TTF 128261).