
Abstract
The change of the anesthesia-, intensive-, surgery-, and oncological nursing postgraduate education into clinical-oriented master programs makes it necessary to increase the professional skills of nurse specialist clinical supervisors. A competence program for clinical supervisors (15 credits) was developed by a university in Norway from 2014 to 2015 in order to facilitate capacity building of academic and pedagogical knowledge. To illuminate nurse specialist clinical supervisors' learning components by implementing a competence program in clinical supervision. A qualitative document analysis of 44 written assignments made by 18 nurse specialist clinical supervisors participating in the competence program, which were collected from the University's electronic learning platform. One main theme and two themes emerged: Changes in the professional paradigm, Learning components that influence clinical supervisors' style and Learning components that have an impact on clinical supervisors' professional growth. This study provides valuable insight into the learning components in clinical supervision that have contributed to a change in the nurse specialist clinical supervision paradigm. The supervisors have formal competence to provide clinical supervision to postgraduate students at master level. The program confirms the value of educating nurse specialist clinical supervisors and we recommend that it should be continued and further evaluated.
Keywords
Introduction
Higher education in Europe has entered a time of reform as a result of the Bologna process, which introduced a new degree structure (Collins & Hewer, 2014). The aim of this process is to harmonize academic degree standards throughout Europe (Collins & Hewer, 2014).
The development of health-care professionals is characterized by specialization and use of technological innovations. A consequence of this is the increased demand for professional skills (Collins & Hewer, 2014; Norwegian Ministry of Education, 2011–2012). Society also demands evidence-based practice and professional development. Therefore, the content of master's programs in several health subjects has been extended to include clinically oriented subjects such as anesthesia-, intensive-, surgery-, and oncological nursing, for which in this article the abbreviation AISO is used. In these programs, clinical practice constitutes a substantial part of the education. The change of the AISO postgraduate education into a master degree makes it necessary to highlight the professional skills of nurse specialist clinical supervisors (NSCSs). Both universities and health-care institutions in European and other countries have a shared responsibility to develop competent nurse specialists through capacity building by means of clinical supervision (CS) (Dobrowolska et al., 2016). Capacity building can be defined as “an essential process for the survival of any individual or organization” (Alleyne & Jumaa, 2007). At the individual level, capacity development contributes to the individual professional paradigm (Törnebohm, 1989). Having a profession means possessing a specific paradigm comprising certain factors such as interest, competence, worldview, and science (Törnebohm, 1989, p. 13). In the professional paradigm, competence consists of cultural, linguistic, communicative, social, and sociocultural factors, and Törnebohm (1987, p. 31) argues that professional activities can enrich and enhance knowledge of the professional paradigm.
A comparative case analysis of CS by Dobrowolska et al. (2016) reveals that most countries have no special requirements in terms of education and experience in the field of CS. The study by Dobrolowska et al. (2016) covers 11 European Union and non-European Union countries. According to Altmiller (2011), the supervisors' skills are significant for the quality of supervision. They are in an ideal position to facilitate learning processes and promote students' professional growth and identity building as future nurse specialists. At present, most NSCSs in Norway have no formal CS competence. To address this issue, the University developed a customized course for clinical supervisors within AISO postgraduate education called the Competence program for NSCSs (NSCS program), 15 credits. The overall purpose of the NSCS program is capacity building of both academic and pedagogical knowledge to raise the quality of student supervision. This is in accordance with the report “Quality in Clinical Studies in Health and Social Sciences Higher Education” (The Norwegian Association of Higher Education Institutions, 2016). The report emphasizes the need for formal competence on the part of clinical supervisors with a minimum of 10 credits (The Norwegian Association of Higher Education Institutions, 2016, p. 7).
With regard to the state of the CS nursing literature, there is an increase in the amount of empirical evidence to support CS practice. In a systematic review of CS evaluation studies in nursing, Cutcliffe, Sloan, and Bashaw (2018) conclude that there has been an ongoing increase in the number of nurses participating in CS during the last 20 years. Nevertheless, there is a paucity of evidence demonstrating effective and competent delivery of CS. Cutcliffe et al. (2018) revealed a lack of clarity in relation to the purpose of CS. Their findings indicate the necessity for the profession to articulate an agreed definition of CS. The authors recommend development of a relevant competency framework for future competency-based CS training (Cutcliffe et al., 2018).
The key point of CS is an opportunity for sharing, learning, and reflecting on clinical experiences of patient care and ethical issues, which leads to professional development and positive outcomes in terms of the quality of patient care (Berggren & Severinsson, 2011).
In the international literature, CS is an umbrella term that encompasses a number of models and perspectives (Fowler, 2011). However, one essential aspect is the idea that CS constitutes a professional relationship where the supervisee reflects on experience. Reflection can occur outside of CS, but CS cannot exist without reflection (Fowler, 2011). According to Jølstad, Røsnæs, Lyberg, and Severinsson (2017), finding time for nurse specialist students and their supervisors to reflect together was reported to be problematic and there is a potential for quality improvements to promote reflection on clinical experiences. A crucial part of the supervisory process is ensuring safety for the patient, professionals, and nursing students (Berggren, Bégat, & Severinsson, 2002). Røsnæs, Jølstad, Severinsson, and Lyberg (2017) argue that time to reflect and discuss together with the supervisor is of the utmost importance for specialist nurses' awareness of their responsibility. Ethical decision-making is an essential component of nursing practice in general and particularly in specialist nursing because of the complexity of the context of acute and critically ill patients (Berggren et al., 2002). The literature on CS indicates that it has been widely investigated (Cutcliffe, Hyrkas, & Fowler, 2011; Pollock et al., 2017). However, more knowledge is needed about which aspects of NSCS' learning components are important in nursing education.
The pedagogical approach in the NSCS program comprises experiential learning. Fowler (2011) defines experiential learning as the coming together of experience of a certain quality and meaningful reflection. The author states that experiential learning is a philosophy that involves the traditional learning theories but highlights the fact that some of the learning material can be based on experience, which differs from the traditional view of classroom lectures (Fowler, 2008). Furthermore, Fowler (2008) claims that CS is a vehicle for the bringing together of experience and reflection. Factors that enrich the interaction of experience and reflection are those usually facilitated in CS.
Overview of the Aims, Themes, and Activities of the NSCS Program.

Note. NSCS = nurse specialist clinical supervisor; CS = clinical supervision.
The aim of the study was to illuminate NSCS' learning components by implementing a competence program in CS. The research question was as follows: What learning components were identified by the NSCS after they had attended a competence program in CS?
Methods
Design
This study has a descriptive design based on the first implementation of a NSCS program (Table 1). According to Øvretveit (2014), successful implementation is based on four areas: structure, strategy, systems, and support. In this study, we support Øvretveit's (2014) definition of implementation as “enabling people to take up a new way of working, which is proved or promises to be more effective” (p. 135).
Sample
Demographic Characteristics of the Specialist Nurses Who Attended the NSCS Program.

Note. NSCS = nurse specialist clinical supervisor.
Data Collection
Overview of Written Assignments During the NSCS Program.

Note. NSCS = nurse specialist clinical supervisor; AISO = anesthesia-, intensive-, surgery-, and oncological nursing; CS = clinical supervision.
Data Analysis
A qualitative document analysis of all the written assignments provided by the NSCS during the program was employed in the study. According to Krippendorff (2012), texts are a good starting point for a content analysis. In this article, the stepwise analysis first explored the documents by focusing on the NSCS' chosen literature and then investigating their reflection levels, followed by a content analysis (Graneheim, Lindgren, & Lundman, 2017).
Analysis of the chosen literature and level of reflection
Themes and Subthemes of the Learning Components Identified by the NSCS After They Had Attended a CS Competence Program.
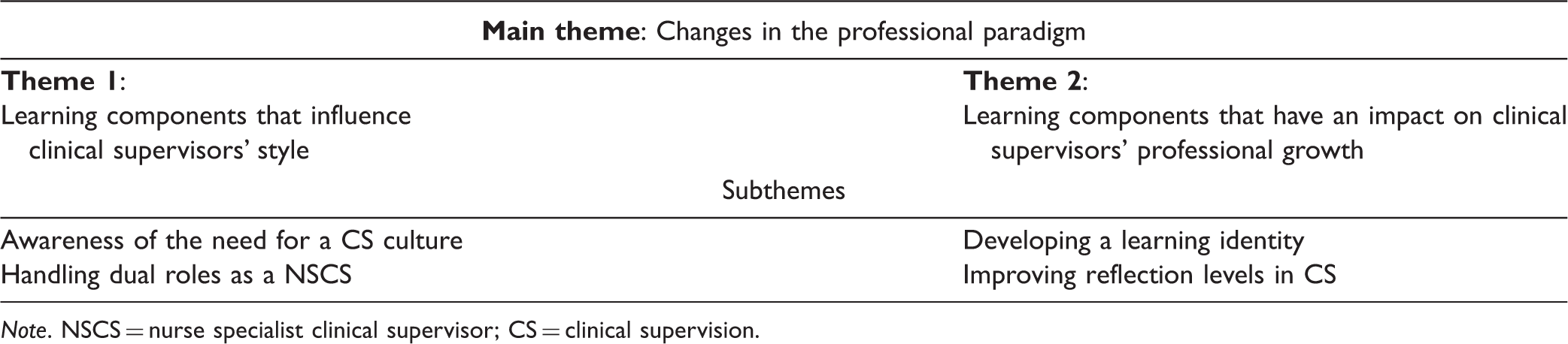
Note. NSCS = nurse specialist clinical supervisor; CS = clinical supervision.
Summary of the Literature in the NSCS' Written Assignments.

Note. NSCS = nurse specialist clinical supervisor.
Overview of the NSCS' Level of Reflection.
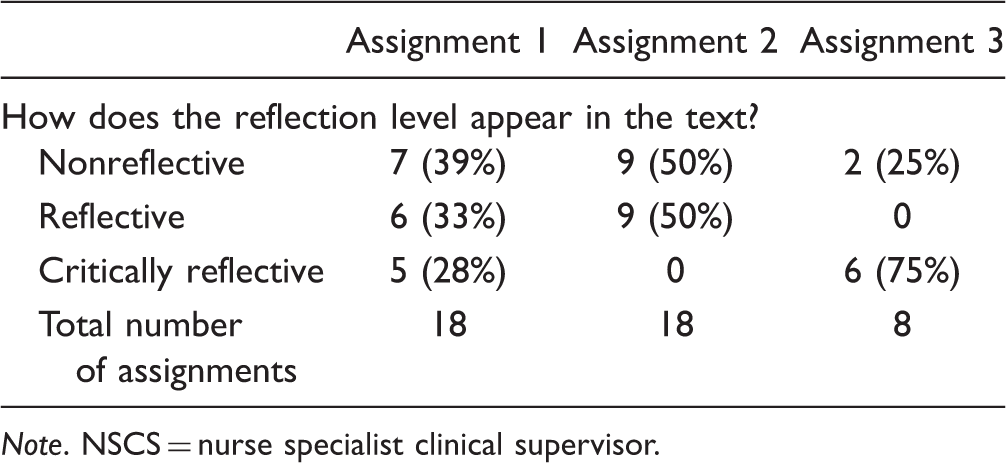
Note. NSCS = nurse specialist clinical supervisor.
Qualitative content analysis of the written assignments
In the second part of the analysis process, we used an inductive approach driven by the texts in which we searched for a pattern in the NSCS' written assignments. All the researchers were involved in the analysis and maintained both a closeness and distance to the texts. The first (A. L. J.) and second author (E. R. R.) read all the texts to obtain an initial impression and overall understanding of the content (Graneheim & Lundman, 2004). Next, they worked on identifying meaning units, which were condensed into descriptions close to the text. The condensed meaning units were then categorized and abstracted into subthemes and themes. To ensure that the meaning units were compatible with the subthemes and themes, the analysis process moved back and forth repeatedly until all the authors agreed on the final categorization and abstraction through shared interpretation and discussion (Table 6).
Ethical Considerations
The head of the Institute of Nursing and the dean of the faculty approved the study. The Norwegian Centre for Research Data gave approval to complete the study (No. 57732). This study adhered to the research guidelines set out in the Helsinki Declaration (World Medical Association, 2013). Important ethical research principles are ensuring the participants' confidentiality and voluntary consent. Ethical aspects such as the consequences of the research for the participants were taken into account as they had the opportunity to decline participation or to withdraw at any time without consequences. The participants gave their written consent after receiving verbal and written information about the purpose of the study during the last seminar of the NSCS program. In accordance with the university regulations, the data were stored securely in a fireproof cabinet. All of the researchers have several years of higher education experience and are nurse specialists with formal CS expertise.
Results
The results reflect the findings from the analysis of the chosen literature, level of reflection, and the qualitative content analysis of the written assignments. One main theme and two themes emerged: Changes in the professional paradigm, Learning components that influence clinical supervisors' style and Learning components that have an impact on clinical supervisors' professional growth. These themes are based on four subthemes: awareness of the need for a CS culture, handling dual roles as a NSCS, developing a learning identity, and improving reflection levels in CS. The themes and subthemes led to a comprehensive understanding of the results and are presented in Table 4.
Changes in the Professional Paradigm
The main theme summarizes the two themes and four subthemes by highlighting the concept of capacity building as a result of participating in the NSCS program for 1 year.
Through experiential learning, the NSCS developed new competence in different CS theories and models of how to improve AISO students' reflection levels. It concerns capacity building through awareness of the NSCS' style as well as the various learning processes that promote professional growth. Their professional growth and supervisor identity were strengthened, making them more capable of handling their dual role as a supervisor and nurse specialist with responsibility for ensuring patient safety and facilitating CS. In addition, the NSCS developed both their linguistic and communicative competence, expressed through their reflection level and ability to pose reflective questions. The results indicate that the NSCS changed their supervisory style and developed increased interest and competence in CS. These changes can be termed a professional paradigm shift.
Learning components that influence clinical supervisors' style
This theme concerns learning components such as Awareness of the Need for a CS Culture and Handling Dual Roles as a NSCS. The CS took place in a complex and challenging context as the NSCS worked in specialist departments with acute and critically ill patients, which can often lead to an unpredictable situation in terms of CS. The NSCS expressed both a need to explain to nurse management that CS requires time and the necessity of supervision for their supervisory role. They revealed a need to raise awareness of their supervisory style through reflection. Another challenge for supervisors was their dual role that involved both ensuring patient safety and facilitating the students' growth and development. At the same time, the NSCS stated that CS of students is an important source of work satisfaction.
Subthemes concerning the CS culture include the way the NSCS desired a recognized CS climate for their students. At the same time, they related that the time allocated to CS is limited. CS is unpaid extra work that is expected to be undertaken by nurse management. NSCS frequently do not have the time and resources to facilitate CS. The result is usually ad-hoc supervision characterized by unpredictability. The NSCS expressed a great need to learn how they could employ communication to pose questions that promote reflection among the students. The following quotations were taken from the NSCS' written assignments: Our CS tradition is that the “expert” teaches the “novice” through demonstration, exercise and correction. In our setting it has not been common for the NSCS to reflect together upon the students' experiences of action. The students can perform a procedure and the supervisor comments “that went well” or says that the students need more practice. We usually do not talk about why and in what way things went well. Our desire as supervisors is to develop communication tools to correct the students in a positive way and help them to reflect on their actions. We need to change the CS culture, which is often experienced as tough by the students. It is important that nurse management and co-workers acknowledge and prioritize the work that the supervisors perform. In the future, CS should be included as part of the nurse specialists' competence development plan at the department. I experience having two roles that do not necessarily coincide, as they raise ethical dilemmas or conflicts of interest. It is my responsibility to contribute to creating relevant and appropriate learning situations for the student, but my primary and most essential focus is always the patient and her/his need for professional nursing. Students are in an addictive relationship with their supervisors in order to become independent. There is vulnerability in this dependence. We wish to encounter this vulnerability with respect because we are aware of the power relationship. Creating security for the student is essential for providing feedback in a way that it is not perceived as negative criticism and distrust.
Learning components that have an impact on clinical supervisors' professional growth
This theme concerns learning components such as Developing a Learning Identity and Improving Reflection Levels in CS. The NSCS expressed a need for supervisory experience and theoretical competence. We identified that the NSCS had developed a thirst for and an awareness of the meaning of knowledge, as well as greater maturity, which awakened the need for continuous learning. Through reading the assignments, counting the use of and evaluating the choice of research and other relevant literature, the NSCS developed evidence-based practice. By investing in and familiarizing themselves with research and CS theory, they extended their knowledge of how to provide students with authority and participation. The results demonstrate that the use of research articles by the NSCS increased from 1.5% on the first assignment to 20% on the third assignment (Table 5).
The use of research articles illustrates that the NSCS strengthened their competence to provide more evidence-based CS of their students. This strategy can promote the students' positive resources. Furthermore, the NSCS expressed a joy of learning and a desire for more education. Improved confidence and maturity enabled the NSCS to argue with nurse management about the need to facilitate CS and acknowledge its importance. They became aware of their responsibility to implement their new CS competence at the workplace: As a supervisor, I am now aware that the dialogue and focus on equality between NSCS and students leads to a higher level of academic quality. It is our responsibility to take the new knowledge into our meeting with the students. We find that critical thinking is a more meaningful term than we previously thought. Now we realize more clearly the value of educating critically minded nurse specialists. The NSCS program made us aware of the fact that we will never be fully trained, either as a nurse specialist or as a NSCS. As supervisors, we also need supervision to improve both our CS competence and our professional competence.
The results from the content analysis indicated that reflection is one of the main learning components. The NSCSs were aware of the importance of reflection in their supervisory role and for the professional growth of both themselves and their students. The texts illustrated a development from a nonreflective level to a critically reflective level: Facilitate the students to reflect on their own practice, it is also crucial that we reflect on and ask questions about our own practice as supervisors. Through reflective dialogue, which is the main form of CS, we should become conscious of our own listening ability, feelings and reactions. It is good practice to be a reflective supervisor. Then we can justify our behaviour and change them if necessary. We have great power and influence in our role as supervisor and therefore ethical reflection is extremely valuable. Through reflection, ethical judgement can be improved.
Discussion
In this study, written assignments from NSCS who attended a CS competence program were analyzed to illuminate the learning components they had gained. The main components revealed by the study are the NSCS' development of interest and competence in CS. According to Törnebohm (1983), these are essential factors in the professional paradigm. The findings emphasize that the learning components influence the NSCS' style and professional growth.
Learning Components That Influence the Clinical Supervisors' Style
In the present study, learning components that influence the NSCS' style comprise the subthemes awareness of the need for a CS culture and handling dual roles as a NSCS. The NSCS program was based on the philosophy of experiential learning (Fowler, 2008), which is grounded on lived experiences and implies a holistic involvement of the learner's body, mind, and feelings. This approach seems to have been successful for the individual professional development of the NSCS and to have contributed to a change in their professional CS style and professional paradigm. This corresponds with Lindström (1992), who claims that a professional paradigm is of a personal nature, embodied in the individual practitioner as an in-depth understanding of key terms, tasks, functions, and perspectives. The NSCS' awareness of the need for a CS culture was characterized by lack of sufficient time to facilitate CS. The NSCS developed a CS community with a shared understanding of the CS field, worked toward a common CS language, and strengthened their communicative skills. This can be seen as social competence that might enable them to influence their colleagues and nurse manager toward an increased understanding and acceptance of the benefits of CS. Cultural, social, and linguistic competence are key factors in a professional paradigm (Törnebohm, 1983). Social and sociocultural competence can be developed in a culture characterized by fellowship, humility, and respect (Lindström, 1992), which corresponds with the way the NSCS attempted to challenge the existing CS culture and style.
Handling dual roles was a source of frustration for the NSCS before they attended the NSCS program. While continuously handling dual roles might be possible in an ideal world, in a complex health-care system with focus on effectiveness, the NSCSs were occasionally required to prioritize. However, they clearly stated that in acute situations, patient safety always comes first. The results of the study may indicate a gap between political and economic thinking. The organization and management of the health-care service are mostly based on the idea of New Public Management on the one hand and the basic ethical and professional codex on the other (Skogsaas, 2011). The purpose of New Public Management can be understood as economic rationality in health care to produce as much as possible to a satisfactory standard to minimize costs. Patients have become “customers” who expect high-quality services, and nurses have become “service workers” (Magnussen, Vrangbaek, & Saltman, 2009), which contrasts with the values and ideals in nursing and CS such as respectfulness, responsiveness, compassion, trustworthiness, and integrity (International Council of Nurses, 2012). The NSCS' awareness of the meaning of critical reflection develops their capacity and competence to handle dual roles. This includes ensuring patient safety while also promoting the AISO students' professional development despite increasing demands for efficiency that often leads to ethical dilemmas in practice. However, how the NSCS' dual role affects patient safety and student learning components requires further research (Dobrowolska et al., 2016). Berggren and Severinsson (2006) point out that ethical decision-making and problem solving are characteristic of a nurse's daily work. Different ethical decision-making styles in CS concern ensuring safety and facilitating the transformation of theoretical knowledge into practice (Berggren & Severinsson, 2006, p. 639).
The NSCS' previous experiences of CS were not particularly appreciated and prioritized by their nurse manager. Changes in the NSCS' style and professional paradigm at an individual level might make the implementation of the new CS competence more difficult when returning to practice where the focus is on efficiency in a context characterized by acute and critically ill patients. The fact that the NSCS program merely provides capacity building in CS on an individual level can be experienced as a challenge. To successfully implement the NSCS' new competence in practice, the nurse management and the whole organization need to be involved (Alleyne & Jumaa, 2007; Øvretveit, 2014). According to Dobrowolska et al. (2016), the CS role has been highlighted in previous international studies focusing on the positive effects of staff attitudes and ward atmosphere on students' clinical experiences. The study also underlines the importance of a supportive context provided by colleagues and nurse managers (Dobrowolska et al., 2016). Few health-care interventions are rapidly adopted but require the investment of effort and resources in their implementation (Øvretveit, 2014). Nevertheless, our results confirm that the NSCS act in a new and more efficient manner due to their improved CS style.
Learning Components That Have an Impact on Clinical Supervisors' Professional Growth
Learning components that have an impact on clinical supervisors' professional growth are encompassed by the subthemes developing a learning identity and improved reflection levels in CS. A thirst for and an awareness of the meaning of knowledge on the part of the NSCS, as well as a greater maturity and the need for continuous learning were identified as the learning components that have an impact on professional growth. The NSCS' interest and increasing competence in CS combined with improved linguistic, cultural, and communication skills reinforce each other (Törnebohm, 1983). This encompasses an awareness of the NSCS' learning identity. A prerequisite for CS is educated supervisors who can influence the development of both the students' and their own professional identity (Holm Wiebe, Johansson, Lindquist, & Severinsson, 2011). CS can increase reflective capacity and strengthen the ability to assume responsibility in nursing. A prerequisite for success in continually developing the NSCS' learning identity is for them to reflect on the way they perform CS and on their own supervisor role and responsibility. Moreover, there is a need to reflect together with other supervisors to maintain their new professional growth and identity. Goward, Kellet, and Wren (2011) believe it is essential for practitioners providing CS to receive CS. Providing CS should be a career-long activity, where the benefits of CS also apply to supervisors (Goward et al., 2011).
A component of special attention was the NSCS' development of the ability to reflect critically. Ekebergh (2007) claims that reflection and learning are strongly linked and reflection ought to be understood as the center of the learning process. Furthermore, the meaning of learning is connecting to the individual's understanding process, thus from this point of view, learning and understanding are synonymous (Ekebergh, 2007). Nevertheless, the heart of experiential learning is the combination of experience and reflection that results in learning (Fowler, 2008). Fowler (2008) claims that “no” reflection is associated with “surface learning,” while “critical” reflection is linked with “deep learning.”
The NSCS' interest in ever-new and life-long learning with the aim of increasing their CS competence contributes to a new preparedness. The paradigm factors interest and competence constitute preparedness (Severinsson, 1990). Being critically reflective means having the ability to see the action in relation to one's own values and attitudes, which can lead to a change in the way we perceive the world around us, other people, and ourselves. Others' response and new perspectives are important on the critical reflection level (Dahl & Alvsvåg, 2013). Therefore, it is vital for the NSCS to reflect critically together with other supervisors in order to continue developing their professional growth and identity. Through reflective capacity, the NSCS might be able to challenge their students to engage in critical reflection, which is one of the core phenomena in CS (Holm Wiebe et al., 2011).
In summary, the results reveal that the NSCS gained a new and extended understanding of the content and possibilities of CS, which they seem to have integrated in their professional identity. Their CS commitment was strengthened in parallel with the increase in their CS competence. This is supported by Törnebohm (1983) who claims that professional paradigm factors such as interest and competence strengthen each other. These competence factors comprise cultural, linguistic, communicative, social, and sociocultural competence understood as capacity building that might lead to a change in the NSCS' professional paradigm. According to Severinsson (1990, p. 40), the interest factor in the professional paradigm triggers commitment, the search for new knowledge, and the development of professional awareness. This corresponds with the NSCS' need for continuous learning and thirst for ever-new knowledge. The results suggest that the implementation of the NSCS program contributed to changes in the NSCS' professional paradigm.
In the absence of research on CS for NSCS, we consider that the study by Dobrowolska et al. (2016) is interesting, relevant, and transferable to AISO postgraduate education. Its aim was to describe and compare the CS' role and responsibilities, experience, qualifications, and employment requirements in 11 European Union and non-European Union countries. However, few countries have developed formal rules, national standards, or qualification requirements for the CS field (Dobrowolska et al., 2016). The United Kingdom, Ireland, and the United States underline that CS have to be specially educated and approved to supervise student nurses. With reference to the Bologna process, there is a need for standardization and harmonization to accommodate the increased globalization of nursing higher education (Collins & Hewer, 2014). Such globalization includes improved opportunities for mobility, employment, and collaborative research across international borders (Collins & Hewer, 2014). The study by Dobrowolska et al. (2016) reveals a strong need for the development of special CS educational programs, which should be organized based on cooperation and communication between universities and health-care organizations (Dobrowolska et al., 2016). The NSCS competence program presented in this study might be a relevant contribution that could facilitate other universities and health organizations to develop CS programs for NSCS at master level.
Strengths and Limitations
This study adopted a qualitative document analysis. The study's strength is the amount of data, which comprised 232 pages of text. By deepening and analyzing the text, we were surprised by the richness of the content. The results have given rise to new questions. A focus group interview could therefore be an alternative and appropriate method for gaining a deeper understanding of the NSCS' learning outcomes through the implementation of the NSCS program. Interaction between participants, together with the group process, is central to focus groups. By exploring and clarifying beliefs and experiences, the researcher can reveal aspects of understanding that are often concealed by the interaction (Liamputtong, 2011). The results of the study cannot be generalized as they are limited to the NSCS program participants.
Conclusion
In conclusion, the implementation of the NSCS program has contributed to changes in the NSCS paradigm. Through experiential learning, the NSCS built capacity by developing their supervisory style, professional identity, and growth. After attending the program, the NSCS gained the formal competence to provide CS to postgraduate AISO students at master level. To maintain the NSCS' interest and engagement in their new CS competence, we recommend that they can be given an opportunity to participate in CS groups in order to critically reflect upon their supervisory style and role. The NSCS program confirms the value of educating nurse specialists in CS and we recommend that it should be both continued and evaluated for further improvements.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.