
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is a growing cause of morbidity and mortality worldwide (Global Initiative for Chronic Obstructive Lung Disease, 2017), and the World Health Organization (WHO) estimates that COPD will be the third most common worldwide cause of death and disability by 2030, from its current fifth ranking (WHO, 2011). Although COPD has generally been considered a disease of men, mortality in women with COPD is increasing (Mannino, Homa, Akinbami, Ford, & Redd, 2002), and the prevalence of COPD in women is higher than in men (Menezes et al., 2005). The changing demographics of COPD have been attributed in part to temporal changes in smoking habits with the popularity of tobacco smoking having increased more in women than men (WHO, 2010).
Recent studies have indicated several gender differences in the clinical expression of COPD. Female patients with COPD had worse symptoms and health-related quality of life than male patients (de Torres et al., 2005; Lopez Varela et al., 2010; Martinez et al., 2007). Furthermore, a few studies suggest there may be gender-related differences in response to patient education. For example, males have shown better compliance with inhalers (Chrystyn et al., 2014), while female subjects are more likely to be admitted to emergency departments with exacerbations (Celli et al., 2011).
However, it is not yet known whether there is a gender-related difference regarding patients' information of COPD in self-management. Lifestyle behaviors such as smoking cessation and exercise are important in determining the prognosis of COPD, and changing behavior is an important starting point to impact information for self-management (Bourbeau, Nault, & Dang-Tan, 2004). It has been reported that a large majority of patients are dissatisfied with the quality of information they receive regarding lifestyle changes and ongoing management with COPD (Jones, Hyland, Hanney, & Erwin, 2004). This is consistent in Japan, where 80% of patients with chronic respiratory diseases would like more education regarding self-management skills (Japanese Respiratory Society, 2010).
The Lung Information Needs Questionnaire (LINQ) was designed to assess the patient's need for information from a patient's perspective. LINQ consists of 22 questions weighted into 6 domains and is designed to be used prior to consultation or to assess the impacts of educational initiatives (Hyland, Jones, & Hanney, 2005). The LINQ has been used to demonstrate the benefits of education for COPD based on information needed to understand their disease and maximize their self-management skills (Jones, Wang, Harding, Bott, & Hyland, 2008; Wakabayashi et al., 2011).
We hypothesized that the existence of gender differences in COPD might be related to the differences in gender-specific information needs of the patient. Therefore, this study investigates gender-related differences in patients with COPD using the LINQ and which indicators are related to patient information needs.
Methods
Patient Selection
Consecutive COPD patients in stable condition, defined as no acute exacerbations or hospitalizations for 3 months prior to the study, were recruited. Inclusion criteria were clinical course, symptoms, and laboratory data that satisfied the clinical diagnosis of COPD, defined as a postbronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) < 0.7, including airflow obstruction assessed by pulmonary function tests with postbronchodilator inhalation (Miller et al., 2005), and the clinical guidelines of the American Thoracic Society (ATS), European Respiratory Society (ERS) staging system to define disease severity (Qaseem et al., 2011).
Exclusion criteria were cognitive dysfunction defined as a score of less than 26 on the Mini-Mental State Examination (MMSE), history of atopy, any apparent clinical features of asthma, receiving any systemic corticosteroid regimens, living in a long-term care facility, or any other respiratory diseases such as bronchiectasis or pulmonary fibrosis. However, patients with comorbidities such as osteoporosis, diabetes, or gastroesophageal reflux disease were included.
Study Design
This cross-sectional and prospective cohort study was undertaken at the Respiratory Care Clinic, which specializes in COPD and is facilitated by Nippon Medical School, Tokyo, Japan.
A standardized self-management education was delivered by the respiratory nurse or primary physician at the Respiratory Care Clinic (an outpatient clinic), with an emphasis on (a) the understanding of COPD, including outlines of diagnosis and management, (b) pharmacological treatments, including positive and adverse effects, and the use of inhalant devices, (c) encouraging patients to exercise daily, (d) avoidance of exacerbations, including an action plan with instructions in the event of exacerbation, (e) smoking cessation, and (f) nutrition, based on ATS/ERS guidelines (Qaseem et al., 2011). All patients received monthly individual sessions for 6 months, with at least 30 minutes spent with each patient. Education was conducted in an interactive style, with patients encouraged to ask questions about current or past sessions. Treatment and health-care management plans were constructed on the basis of each patient's individual self-management needs from their previous visits from the abovementioned six components.
Assessment Measures
The LINQ is divided and scored into six domains including disease knowledge, medication, avoidance of exacerbations, smoking cessation, exercise, and nutrition, whereby a higher LINQ score indicates a lower need for information on self-management of the disease. The total LINQ score is obtained by adding the six domain scores, giving an overview of the patient's information needs, while the individual domain scores identify specific needs. We selected the LINQ because it is based on patient needs and because of its easy-to-use format. Because it was designed with the patient in mind, wording of the questionnaire is simple to comprehend, making patients' responses more reliable. Furthermore, because it takes only an average of 6 minutes to complete, it is an efficient self-complete tool placing minimal time burden on medical staff.
Pulmonary function parameters including postbronchodilator FEV1, vital capacity, FVC, and FEV1/FVC ratio (FEV1/FVC, %) were measured according to the ATS guidelines (Miller et al., 2005) using equipment for lung function testing with computer processing (CHESTAC; CHEST Co., Tokyo, Japan). The predicted values were calculated based on the standards of the Japanese Respiratory Society (Nagai, 2011).
Dyspnea was evaluated using the modified Medical Research Council dyspnea scale (MMRC) related to COPD disability (Mahler & Wells, 1988).
The 6-minute walking test (6-MWT) was employed according to ATS/ERS standards (Singh et al., 2014), during which oximetry was measured every 5 seconds with a pulse oximeter (PULSEOX; Teijin Co., Tokyo, Japan). A qualified respiratory specialist supervised tests.
Body mass index was calculated as the ratio of weight in kilograms to height in square meters.
Cognitive function was assessed by MMSE (Folstein, Folstein, & McHugh, 1975; Maki et al., 1999). Activities of daily living (ADL) were assessed for basic ADL (BADL) and instrumental ADL (IADL; Lawton & Brody, 1969). BADL consists of activities such as eating, dressing, personal hygiene, toileting, and physical mobility, whereas IADL includes more challenging activities such as cooking, shopping, home chores, laundry, management of money and medicines, and using public transportation. Disease-specific health-related quality of life was assessed using the St George's Respiratory Questionnaire (Japanese ver.; Jones, Quirk, Baveystock, & Littlejohns, 1992).
Comorbidities were measured using the Charlson index (Charlson, Pompei, Ales, & MacKenzie, 1987), which is associated with mortality (Budweiser, Harlacher, Pfeifer, & Jorres, 2014) as well as quality of life in COPD (Almagro et al., 2002). Charlson index can range from 0 to 33, with higher scores indicating more coexisting conditions.
Information was collected regarding the patients' education level and working years (including full or part time).
International Review Board Statement
The ethics committee of the institution approved this study with written informed consent obtained from all subjects.
Statistical Analysis
To determine the sample size, the power calculation was based on the primary outcome, the total LINQ score. In our preliminary analysis (data not shown), the distribution of the total LINQ score was with a standard deviation of 4.28. In order to detect 2.80 or more difference of the total LINQ score with an alpha level of .05, 1-beta, 0.90, and this SD, the required sample size was 100. Because we anticipated 15% attrition, we planned to assign 120 patients.
A two-sample t test was used to compare values between the two groups (with Bonferroni posttest correction where appropriate). Employing the chi-square test tested the difference in proportions. Student's t test was used for statistical analysis in cases in which the variance was homogeneous, and Welch's test was employed when the variance was heterogeneous. To investigate the correlations, linear regression analysis was applied, taking the Pearson's correlation coefficient as a measure of the extent of the relationship.
Data are presented as the mean ± SD unless otherwise stated. Significance was assumed if the null hypothesis was rejected with a probability of p < .05. Calculations for statistical analysis were performed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of Patients.

Note. All values are represented as mean (SD). VC = vital capacity; FVC = forced vital capacity; FEV1 = forced expiratory volume in 1 second; FEV1/FVC, % = forced expiratory volume in 1 second/forced vital capacity ratio; 6-MWT = 6-minute walking test; MMRC = modified Medical Research Council dyspnea scale (range 0–4); MMSE = Mini-Mental State Examination; IADL = instrumental activities of daily living; SGRQ = St. George's respiratory questionnaire; ATS = American Thoracic Society; ERS = European Respiratory Society.
*p < .001. **p < .0001.
Females displayed lower vital capacity (p < .0001), FVC (p < .0001), and values for FEV1 (p < .005). However, there was no significant difference noted in FEV1, % predicted or COPD severity between genders.
No significant gender differences were seen on MMRC dyspnea, distance on the 6-minute walking test, body mass index, Charlson index, MMSE, the total score of St George's Respiratory Questionnaire, or school education in years.
Both males and females obtained full scores in BADL, while IADL were significantly higher in females (p < .0001), and the number of working years was significantly higher in males (p < .0001).
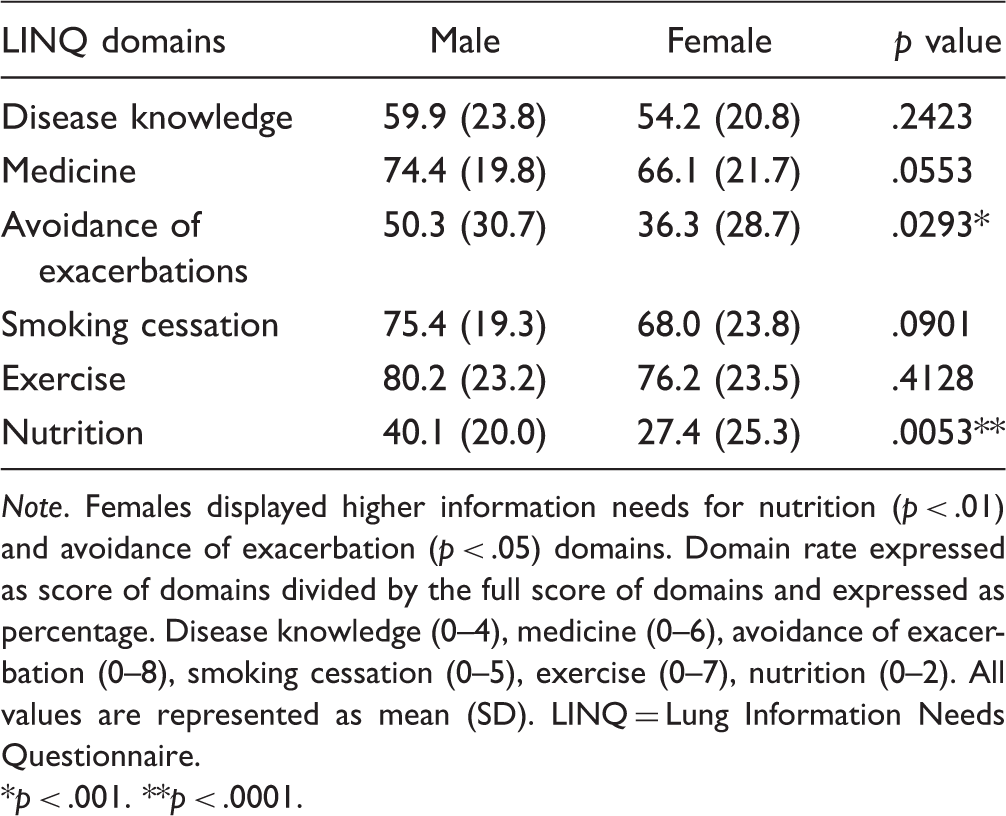
A marked gender difference was seen in the total LINQ score (Figure 1), with females showing higher information needs than males (female 18.0 ± 4.57, male 21.2 ± 4.57, p < .001; lower LINQ score indicates higher information needs). Females displayed significantly lower in LINQ domain scores for avoidance of exacerbation (p < .03) and nutrition (p < .006; Table 2), but no difference in information needs was seen for disease knowledge, medicine, smoking and exercise domains.
Comparison of total LINQ scores between male and female patients. Females displayed lower scores on the total LINQ score (p < .001) and showed higher information needs on self-management (female 18.0 [SD = 4.57], male 21.2 [SD = 4.57], p < .001; lower LINQ scores indicates higher information needs). Range of the total LINQ score: 0–32. Comparison of LINQ Domain Scores Between Male and Female Patients. Note. Females displayed higher information needs for nutrition (p < .01) and avoidance of exacerbation (p < .05) domains. Domain rate expressed as score of domains divided by the full score of domains and expressed as percentage. Disease knowledge (0–4), medicine (0–6), avoidance of exacerbation (0–8), smoking cessation (0–5), exercise (0–7), nutrition (0–2). All values are represented as mean (SD). LINQ = Lung Information Needs Questionnaire. *p < .001. **p < .0001.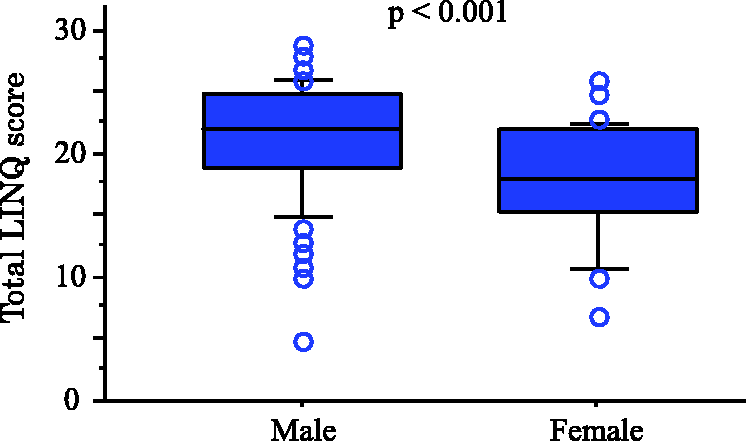
Indicators for Total LINQ Score in Logistic Regression Models by Gender.

Note. LINQ = Lung Information Needs Questionnaire (range: 0–32: Lower scores indicate higher information needs); FEV1 = forced expiratory volume in 1 second; 6-MWT = 6-minute walking test; MMRC = modified Medical Research Council dyspnea scale (range 0–4); MMSE = Mini-Mental State Examination; IADL = instrumental activities of daily living; SGRQ = St. George's respiratory questionnaire; ATS = American Thoracic Society; ERS = European Respiratory Society.
*p < .05. **p < .01.
Discussion
COPD is a chronic illness that is usually self-managed in a home care setting. According to the latest ATS/ERS statement on pulmonary rehabilitation, education to promote effective self-management is the cornerstone of this intervention (Blackstock et al., 2018). Several studies have indicated that efficient self-management yields better outcomes as measured by reducing the number of hospital days and emergency visits (Bourbeau et al., 2003; Zwerink et al., 2014), lower frequencies of exacerbation (Worth & Dhein, 2004), improved quality of life (Bourbeau et al., 2003; Cannon et al., 2016), and reduced medical expenditure (Hernandez et al., 2003; Gallefoss, 2004). Efficient self-management of COPD is achieved by enhancing patients' knowledge and skills regarding COPD (Bourbeau et al., 2004).
The LINQ was used in this study, as it is a validated assessment tool specifically developed to assess patients' information needs in a number of domains including disease management. We found that the total LINQ score was lower in females with COPD, and after comparing domain scores between genders, female patients scored significantly lower for avoidance of exacerbation and nutrition, indicating higher information needs than males. The LINQ's avoidance of exacerbation domain associates with whether patients have obtained information on “how to respond” if they experience an exacerbation or if their condition worsens and whether medical staff have adequately instructed patients on executing an action plan, while the nutrition domain indicates whether patients have a sufficient understanding regarding nutrition related to COPD. It is known that females with COPD are more likely to be admitted for exacerbation (Roche et al., 2014) and emergency visits (Martinez et al., 2012). Furthermore, women generally have less knowledge for self-medication and tend to wait longer than males before visiting an emergency room (Chapman, Tashkin, & Pye, 2001). In our study, females showed that they did not have sufficient information on how to execute a successful action plan, what to do at exacerbation, or when their conditions worsened. These suggest that for female COPD patients, more exacerbations and emergency visits may occur as a lack of information regarding patient needs are not being met and that action plans might not be executed correctly. For information on nutrition, it has been previously reported that females have a better knowledge on diet compared with males (Farragher, Wang, & Worsley, 2016) and are more sensitive to improving or avoiding obesity (Paeratakul, White, Williamson, Ryan, & Bray, 2002). However, a study reported contrasting results in that the prevalence of nutritional depletion is higher in female patients with moderate to severe COPD than in males (Vermeeren et al., 2006). Females with COPD may indeed have sufficient knowledge regarding general nutrition and diet; however, they might lack disease-specific knowledge on nutrition and diet. Furthermore, the LINQ domain scores for smoking and medication were lower in female patients suggesting higher information needs than male patients. Females find it more difficult to stop smoking (de Torres et al., 2005; Camp & Goring, 2007), and this may be due in part that pharmacologic therapies are less effective in women (Camp & Goring, 2007) and that females tend to have less information on smoking cessation.
In addition, gender differences on medication were reported. The proportion of females on respiratory medication was twice that of males; however, there was no difference in medication use between men and women (Dales, Mehdizadeh, Aaron, Vandemheen, & Clinch, 2006). This trend was seen in our study. Females received the same education but showed poorer information in the medicine domain.
The total LINQ score was associated with gender, FEV1, % predicted, and MMSE. Also, in male patients, this trend was seen; however, MMRC was associated with total LINQ score in females only. The rate of clinical intervention increases according to severity, and even after diagnosis, physicians unfortunately tend to neglect clinical intervention in COPD (Takahashi et al., 2003). Patients with early-stage to mild COPD are not perceived as high risk and subsequently might not receive an adequate self-management education, and this may explain why the total LINQ score was correlated with FEV1, % predicted.
In this study, we excluded patients scoring less than 26 on the MMSE, but there was a significant correlation seen between information needs and cognitive impairment in patients. It has been reported that severe COPD is associated with lower level cognitive performance (Hung, Wisnivesky, Siu, & Ross, 2009). Regular assessment of cognitive performance is important and should be used in the education of COPD patients. Although there was no significant difference seen for dyspnea between males and females and that the total LINQ score was associated with only MMRC in females, women with COPD are more likely to report dyspnea (Lopez Varela et al., 2010; Martinez et al., 2007). This supports our findings that the total LINQ score was significantly associated with dyspnea in females. However, it has also been reported that men may be more reluctant to report the level of dyspnea they experience (Camp & Goring, 2007). Furthermore, after adjusting for lung function, women with COPD were more likely to experience depression and anxiety compared with men (Di Marco et al., 2006). The benefits of symptomatic COPD may have an influence on information that patients obtain rather than by severity, and this may have led to dyspnea being associated with information needs in females.
Limitations
The present study includes some limitations. Recruitment was limited to 122 patients due to time and funding constraints, and the number of females was considerably less than the number of males. Our study also could not confirm recent reports of higher COPD prevalence of among women (Han et al., 2007). In Japan, the prevalence of airflow limitation in males was 16.4% and 5.0% for females (Fukuchi et al., 2004), and the gender ratio of Japanese smokers is approximately 4:1 (males: females) (Health, Labour and Welfare, 2012). In addition, a primary setting (23 hospitals and 33 general practices) study showed females accounted for only 14.6% of the subjects with airway obstruction (FEV1/FVC < 70%; Takahashi et al., 2003). Even though the prevalence of females with COPD is increasing worldwide, at present, there are still more male patients with a formal diagnosis of COPD in Japan, and these rates are similar with our study. There may also be ethnic differences as all our patients were Japanese. COPD is known as more of a heterogeneous disease, and therefore, more studies with larger sample sizes and different clinical settings are needed.
Implications for Practice
Current guidelines for the self-management and treatment of COPD have largely been derived from studies that are disproportionately male dominated (Jenkins et al., 2017). While some studies have shown that females with COPD endure a higher burden for comorbidities such as asthma (Dal Negro, Bonadiman, & Turco, 2015), anxiety, and depression (Di Marco et al., 2006), the current study found that female subjects reported higher information needs in the overall score and, in particular, in the avoidance of exacerbation and nutrition domains. Thus, these findings suggest a possible gender bias when assessing female patents. Therefore, better awareness is needed on the part of medical staff to recognize the importance of gender-specific approaches in the treatment and self-management of COPD for female patients.
This study revealed that by assessing the patients' lack of information, gender differences for COPD might be more easily identified, which might better assist medical staff in delivering optimal treatments to female patients with COPD.
Summary
In conclusion, by employing the LINQ, we demonstrated that female patients with COPD showed higher information needs in the self-management of COPD, which might assist in shedding light on gender differences in the clinical course of COPD management. Behavioral differences in gender might have an effect on the long-term management of chronic diseases such as COPD.
Footnotes
Acknowledgments
The authors would like to thank Mr. Jason Tonge from St. Marianna School of Medicine for his English review of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.