
Abstract
The delivery of palliative care in the community setting has been recognized as a valued and challenging aspect of nursing care. To this end, care pathways have been shown to support nurses in a variety of settings to deliver individualized patient care. This study provides a qualitative evaluation of an end-of-life intervention known as the Dignity Care Intervention (DCI) based on patients’ perspectives. The DCI consists of four sections: a manual, the Patient Dignity Inventory, reflective questions, and evidence-based care actions. A qualitative design underpinned by the philosophy of Merlau-Ponty was employed for the evaluation of the DCI. Data collection included individual interviews with participants (n = 25). Interview data were analyzed using framework thematic analysis. Four theme categories were identified: “experience of DCI,” “responding to my illness concerns,” “how illness affects me as a person,” and “how illness concerns affect my relationships.” The DCI was found to enable patients to discuss openly important issues with community nurses that they might not otherwise have raised. Participants conveyed satisfaction with the support they received through the DCI. The use of care pathways detailing interventions to manage clinical problems and ensure systematic integration of the best available evidence into care delivery can improve end-of-life care.
Introduction
The need to improve the quality of end-of-life care for people living with advanced, progressive, and life-limiting conditions has been recognized within the health care strategic and policy direction in the UK (Department of Health, 2008; The Scottish Government, 2008) and abroad (Martin-Moreno et al., 2008). The majority of people (60%–67%) indicate that if circumstances permit, they would prefer to die at home; hence, the increase of home deaths from 18.3% in 2004 to 20.8% in 2010 (Gomes, Calanzani & Higginson, 2011; Gomes et al., 2012; Gomes, McCrone, Hall, Koffman, & Higginson, 2010). Therefore, primary health care teams have a pivotal role in the coordination and provision of end-of-life care (Murray & Sheikh, 2008).
The delivery of palliative care in the community setting is recognized as a valued and challenging aspect of nursing (Walshe & Luker, 2010). This care is often provided by generalist district nurses and can be supported by specialist nurses, depending on the complexity and needs of the patient and family (Andrews & Seymour, 2011). Community nurses (CNs) undertake key roles in the assessment, planning, coordination, and provision of care (Burt, Shipman, Addington-Hall, & White, 2008). However, evidence suggests that CNs may struggle with psychosocial aspects of end-of-life care (Evans, Stone, & Elwyn, 2003; Walshe & Luker, 2010) and can show limited capability to engage in psychological concerns (Griffiths, Drew, & Goldman, 2010).
The concept of dignity has been characterized as “notoriously vague” and is attributed to three characteristics: (a) subjective, (b) social or relational, and (c) intrinsic (Leget, 2013). Subjective dignity is described as “something that people experience of themselves” (Leget, 2013; Leung, 2007). Social and relational dignity refers to the recognition of one’s social position; whereas intrinsic dignity, originating from the work of Cicero, is unique to humans and separates them from other beings (Leget, 2013; Van Brussel, 2012). This study focuses on aspects of subjective dignity through patient experience.
Patient experience refers to how patients perceive their illness, how it impacts on their daily life, and what it is like to use health, social, and voluntary care services. This definition acknowledges the totality of experience, including survival, morbidity (physical and psychological), social, and family issues and was devised by the research team and advisory group for the purposes of this study. Palliative care lends itself well to a patient-focused approach, and person-centered care is fundamental to the work of palliative care clinicians. However, there is a paucity of palliative care research, particularly when it relates to end-of-life care and nursing that is patient focused and explores patients’ experiences. Therefore, there is an increasing need to create a patient-focused culture of involvement, listening, and feedback, wherein patient experience is the catalyst for improving services.
Care pathways detailing interventions to manage clinical problems and ensure systematic integration of the best available evidence into care delivery has been shown to improve end-of-life care (De Bleser et al., 2006; Phillips, Halcomb, & Davidson, 2011). The Dignity Care Intervention (DCI) for use by CNs offers one such intervention.
The Dignity Care Intervention
The DCI—previously known as “Dignity Care Pathway” (Brown, Östlund, & Johnston, 2011; Johnston, Östlund, & Brown, 2012; Östlund, Brown, & Johnston, 2012) was renamed after the suggestion of clinicians in an effort to make a distinction from other currently existing pathways, describes a sequence of clinical steps or tasks. It was designed to help CNs conserve the dignity of people nearing end-of-life (see Figure 1). The DCI, based on an empirical model of dignity (Chochinov, 2002; Chochinov, Hack, McClement, Kristjanson, & Harlos, 2002), enables CNs to individualize end-of-life care by using evidence-based care actions in relation to key patient identified dignity-related concerns.
Stages of the DCI.
The DCI was developed from a systematic review providing research evidence (Johnston et al., 2015; Östlund et al., 2012) and from focus group interviews with patient participants, carers, and health professionals to gain local context evidence (Brown et al., 2011). Use of the DCI is preceded by an education day. The DCI consists of four component parts: an instruction manual, the Patient Dignity Inventory (PDI), examples of reflective questions, and suggestions on care actions.
First, the PDI, a validated tool to assess various facets of dignity (Chochinov et al., 2008; Chochinov et al., 2012), is used to identify dignity-related distress and key concerns from the patients’ viewpoint. The PDI questions are scored from 1 (not a problem) to 5 (an overwhelming problem). Any items scored 3 or more were issues seen as a problem for the patient and, therefore, a concern to be dealt with by the nurse, using reflective questions and suggested care actions.
Second, reflective questions are used to expand the identified issues, as well as elucidate patient preferences on how to deal with them, and to identify if further actions are needed. These questions are also an intervention per se (Benzein, Hagberg, & Saveman, 2008) and a way of acknowledging a person’s human value and worth. An example of a reflective question in response to the item “worrying about my future” is “is there anything about the later stages of your illness that you would like to discuss?”
Third, care actions are intended to be used, by the nurse, in discussion with the patient. An example of a care action for the PDI item for no.15 “feeling like I have unfinished business” is: listen to and acknowledge patients’ perceptions on what they think needs to be done, support patients in achieving these things and refer to others if required, and give room for and support patients to say goodbyes and reconciliation.
Finally, CNs evaluate the effectiveness of the care actions used by reusing the PDI. This maintains continuity and identifies new issues. Thus, the circle of care continues.
A recently published feasibility study found that the DCI was acceptable to CNs and helped them identify patient dignity-related concerns. Using the DCI helped CNs provide holistic, dignity conserving care for people approaching end-of-life care (Johnston, Östlund, et al., 2012).
This article specifically explores patients’ perceptions about whether the DCI identifies dignity-related key concerns and if so, how it enables the delivery of individualized dignity-conserving nursing care. The primary objective of this study was to explore how the DCI enables patients’ dignity-related needs to be assessed and met.
Methods
Study Design
This study utilized a qualitative, evaluation approach, with the design, data collection, and analysis informed by the work of Merleau-Ponty (Diprose & Reynolds, 2008; Earl, 2010; Merleau-Ponty, 2005; Thomas, 2005). Merleau-Ponty postulates that embodiment is the basis of experience and perception. He argued that perception provides a direct experience of events, objects, and worldly phenomena. The key tenet of this philosophy as applied in this study is in relation to the distinction between the body object and body subject or lived body; the body of personal experience, as well as the integral interconnectedness between people and their life world, in particular, the interconnectedness between nurses and patients at the end-of-life (Diprose & Reynolds, 2008; Merleau-Ponty, 2005; Moran, 2000; Thomas, 2005). This philosophy provides a means of understanding whether patients’ dignity-related concerns were met by asking them to describe their everyday embodied experiences. This approach supports the evaluative intentions of the study in by enabling patients’ experiences and perceptions of the DCI to emerge.
The development and delivery of the project was supported by a research steering group and a patient advisory group.
Setting
Participants were recruited from three geographic areas across the North East of Scotland, UK.
CN Involvement
CNs were identified by their managers and were invited to participate in the study and use the DCI. The CNs attended one day of training on the use of the DCI, during which they also discussed the concept of dignity-conserving care. In total, 39 CNs (community experience ranged from 1 to 31 years [mean length of community experience 12 ± 7.24 years; range 1 to 31 years]) were trained. All participating CNs were invited to attend two focus groups at the beginning and end of the study, wherein their opinions on the study and pathway were elicited (reported elsewhere). All participating CNs were given a written information sheet, signed an informed consent form, and were assured of confidentiality and anonymity.
Participants
Participants with advanced disease (cancer and other life limiting progressive illnesses) who were in the last months of life (for example on the palliative care register) were invited by their CN to take part in the study.
Data Collection and Procedures
Ethical and research governance approval for the study was obtained through the local NHS REC. Participants were identified purposively by their CN. Participants meeting the inclusion criteria and having an established relationship with their CN were invited to participate in the study. Names of participants who agreed to participate and with whom the participating CN had used the DCI were given to the researcher. These participants were given an information sheet outlining the study, with those who agreed to take part providing written consent.
The majority of participants were interviewed at home with the exception of one participant who was interviewed at the local hospice. A semistructured interview guide was developed with the support of the patient advisory group, the expert steering group, and the principal investigator (BJ). Questions within the interview guide were developed to capture participants’ views on the use of the DCI by their CNs, and to explore if the DCI allowed their dignity-related concerns to be expressed and subsequently addressed.
Data were collected between February 2012 and August 2012. All interviews were audio recorded after consent and transcribed verbatim. Reflexive notes were also taken after each interview.
Data Analysis
Data analysis was facilitated using computer software QSR NVivo© 9. Data were organized using framework analysis, which is an explicit analytic process of charting and sorting the data, to facilitate comparisons and interpretation of the key emerging themes (Ritchie, Spencer, & O’Connor, 2003; Please see Figure 2 for further details).
Stages of framework analysis.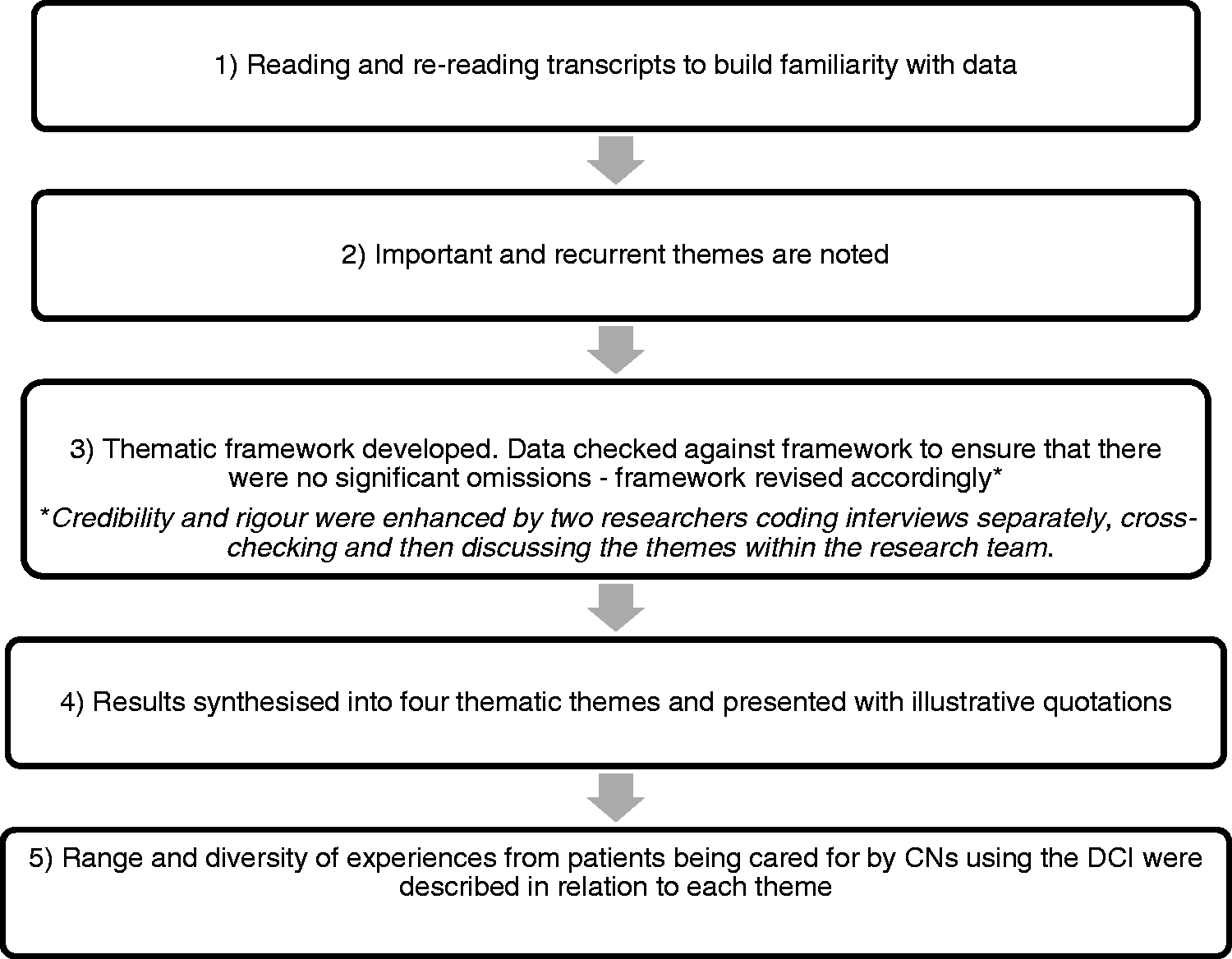
Results
Sample Characteristics
Patient Characteristics.
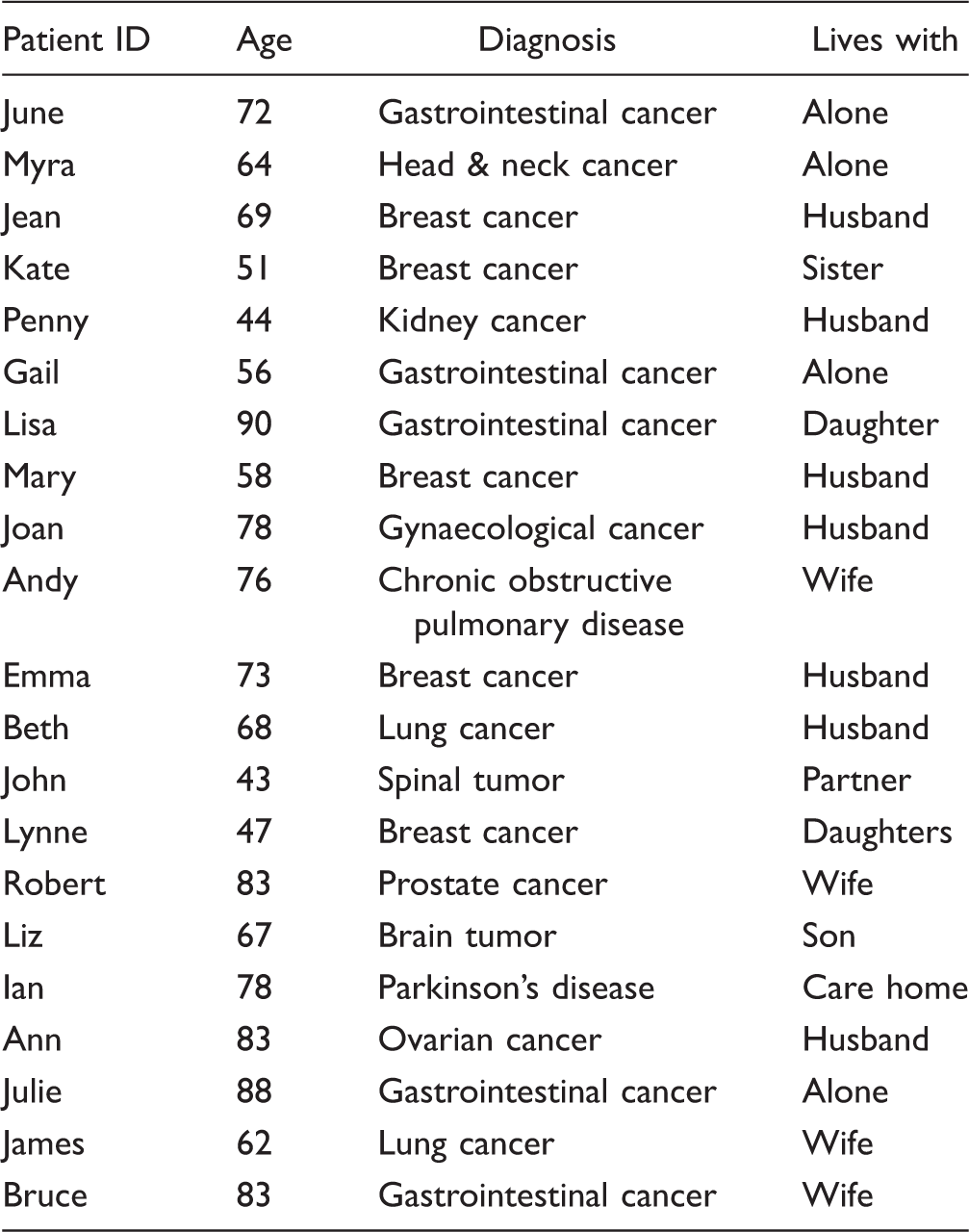
The analysis of the interviews resulted in four theme categories and 16 subthemes. Three of the four themes aligned closely to Chochinov’s model of dignity (Chochinov et al., 2002). This was expected since the model provided the framework for the DCI and that the questions in the PDI are derived from the model. The four theme categories were “experience of the DCI,” “responding to my illness concerns,” “how illness affects me as a person,” and “how illness affects my relationships” (Figure 3). These will be presented and further discussed later.
Four theme categories and subthemes.
“Experience of the DCI”
The theme category of “Experience of the DCI” was composed of the subthemes; It is ok to be asked; giving permission to talk; DCI providing structure and timing of the DCI.
It’s ok to be asked or acceptability of DCI
The majority of participants said that it was “OK to be asked” to participate in the study and found it acceptable to respond to the questions from the PDI. While some participants acknowledged the potential of some questions to raise emotions, in general, questions were found to be straightforward, relevant, and pertinent to living with an advanced illness. I thought they (the questions) were quite relevant to my illness, I just thought they were relevant and they were easy to understand. (Lynne)
Giving permission to talk
As a result of this study, the use of the DCI allowed participants to initiate discussions with their nurse, where open emotional expression led to further, deep, significant conversations with staff. Participants stressed that talking about their concerns allowed information to be shared; which resulted in an increased understanding of their illness, and also allowed plans to be made for the future. For some participants, the use of the DCI, in particular the PDI, and the subsequent reflective questions, gave permission to discuss important issues they would not have raised otherwise. There were issues that I had thought were of concern to me … there were further questions asked, not leading questions, that made me think maybe more broadly or deeply about the issues involved. (James) Not making any difference to me one way or another, to tell you the truth, but you see, for some people it might, because they may not be so well off with people to talk to. (Val, patient)
DCI providing structure
The structure of the DCI was found to be helpful in forming a picture of participants’ concerns and the severity of these, and provided a focus to prioritize issues for further discussion. This approach to gathering information was perceived to be straightforward, quick, easy, and prevented information from being missed. That’s probably better being structured like that because, there's probably things on there you wouldn’t think of saying at the time. And there's probably things on it, you’d think “I should have thought of that, an hour later you think” ffft! I should have said that to the nurse, and I should have said this. (John)
Timing of the DCI
Several participants highlighted that their situation and needs can change over time, and offered suggestions of timing for the use of the DCI, such as being part of an assessment and review, perhaps monthly or every 3 months, or if the nurse identified a change in the patient and family situation. I suppose it would really need to be on-going from now and further down the line as well […] because as my illness progresses that will change. My priorities will change, my worries will change, my perception of help I'm getting or not getting will change. (Myra) Maybe every month, I don’t know. It depends on what [the nurse] has found with that person, and if [the nurse] has found an area where they're needing more support. (Lynne)
“Responding to my illness concerns”
Participants explained the importance of responding to a number of illness concerns causing them physical and psychological distress and limited functional capacity.
Physical distress
Participants reported a number of care actions by nurses related to the relief of physically distressing symptoms, such as, breathlessness, cough, fatigue, pain, loss of short-term memory, sleep disturbances, and nausea. These included use of medication, such as inhalers and steroids for breathlessness and analgesics, as well as pressure area care, and the nurse addressing practical needs, such as ordering a hospital bed. The provision of patient education related to illness modalities were also commonly identified nursing care actions: … and her [nurse] just even coming in today just to do reassure me, because she got on top of everything, she told me that I would get my pain killer, I'd run out of my morphine pain killer, which I've got to have all the time, I've got a really sore ear, I've got a bedsore in my ear […] which has broken out, which she’s going to have to get sorted, so she’s getting that sorted out. Also she's looking at a new mattress for me for my bed, and just coming, knowing that she’s coming to do these things for me […] just reassuring isn't it? (Molly)
Functional capacity
Six participants pointed out that symptoms, such as fatigue, had an impact on their functional capacity (affected mobility, less mental acuity, incontinence, not being able to attend to their own personal hygiene, getting dressed) which subsequently impacted on their feelings of dependence. They identified both nursing and personal actions to help them with these issues (use of catheters, being bathed by a nurse, and use of a chair at the wash basin). Yeah that's right, Oh I need that (urine catheter), I've been slightly incontinent with urine and I've had to run like heck, you know so that, that’s been a help. (Emma)
Psychological distress
Seven participants also identified dignity-related concerns that caused them psychological distress. These issues included dealing with the new vocabulary of end-of-life, such as “keeping it stable,” feelings of frustration, the decision not to be resuscitated, and fear of the actual stage of death. Nursing care actions identified by participants involved discussions regarding the stages of dying and the available support; and in one case, the use of antidepressants. maybe be quite a balance and I am dealing with quite a lot of, of stuff with my illness and, I mean you're diagnosis is completely different when it's secondary, you know [yeah, yeah], it's not like the first diagnosis, the, the words they kept using was “eradicate, eradicate, eradicate”, and now the words are just “keeping it stable” and [...] control and palliative pain relief and the vocabulary’s all different, so sometimes it does still get overwhelming. (Lynne)
“How illness affects me as a person”
Several aspects of dignity included the impact of illness on participants’ sense of personhood and related needs. Personhood can be seen as an acquired status of being a “human being,” established through the words, actions, and attitudes of others. Five subthemes were identified: accepting the new reality, affected roles, living day to day or maintaining normality, retaining autonomy or control, and self-preservation.
Accepting the new reality
The DCI offered participants a chance to discuss their thoughts and feelings with their CNs and helped them in accepting their new reality. In their conversations, participants described the ways in which they dealt with their illness experience by remaining positive, and by “getting on with it.” Others openly accepted the finality of their illness and impending death, with some relating it to the inevitability of old age. Some participants struggled to accept their situation and reported on-going feelings of shock, anger, and asking “why me.” It's difficult really to put it into words … I was angry at what I had not done or, how had I got into a situation where I had “why me?” (Ian) Yeah well, when [name of nurse] was here, I wasn’t crying or anything, because, I've accepted it. I know that … I know that I'm not going to be here forever [crying] but I'd like to think I've got another 3 to 4 year to go [very emotional] I'm a positive person. (Beth)
Affected roles
A major concern reported by participants was being unable to contribute to previous roles including practical, caring, and leisure activities. This resulted in feelings of loss, anxiety, frustration, and low self-worth. Participants mentioned that other family members needed to assume extra roles for them. Nursing actions in response to these concerns included providing positive reinforcement on achievable roles. I’m the organizer in this family and this is what worries me about what’s happening to me because Frank (husband) is 9 years older than me and I felt it should be … I should be the one that’s looking after him and now he’s looking after me. And it’s difficult for him. But that’s the thing when you are the organizer … and you are no longer able to do it, it’s very difficult. (Jean)
Living day to day or normality
For participants, living on a day-to-day basis and maintaining normality was a way to cope with the uncertainty, the changes in their well-being and to help maintain their dignity. Participants discussed with their CNs, the importance of doing normal things and carrying on with living as usual. This sometimes required adjustments to how activities of daily living were maintained, such as, taking things more slowly. Take it slowly and … carry on as usual. (Andy) Just take a day as it comes, every day is different. You can wake up in the morning and you’re feeling down […].but you just have to get on with it. Other days you’re out and you feel great and away you go and that’s it. Every day is different. (Ian) I mean we've just got to deal with things on a day-to-day basis, ‘cause you can't make too many plans for the future in a lot of ways. […] It's like you live two different lives you know, you live temporarily in the life that you used to have, because you still have all the normal things in life to do, like paying the bills […] and cutting the grass, and doing the shopping and all that … (Gail)
Retaining autonomy or control
For 10 participants, retaining control over their life was an important aspect of their dignity. Participants stressed the importance of being able to make their own choices and decisions, including treatment, place of care, and care provision. The DCI helped in voicing their needs to their CNs. Nursing actions identified involving participants in the decision-making process, as well as building confidence by pointing what participants can already do to maintain their autonomy. I know I am achieving, getting up and having a shower and doing my shopping, that’s a big achievement, but before I never really thought about that as an achievement, it was [yeah] (name of nurse) brought that to my notice that, you know having a shower and that’s all big things because some days you were unable to actually do that in the past. (Lynne)
Self-preservation
A few participants identified key concerns (via their scores on the PDI and the nurse using the DCI) related to the impact of their illness on their self-perception. They maintained that their illness experience had brought about physical and emotional changes, and changes to how others treated them. These changes were described as not feeling like the same person as they were before the illness. Being listened to and having the opportunity to discuss their feelings with their nurses were deemed as the most helpful care actions by participants. I have definitely changed, the illness itself and the hormone treatment … I was in the police all very male, very hard environments, and I was completely different, now this thing has changed me, so that, we went through all that with the nurse. (James)
“How illness affects my relationships”
The theme of how illness affects my relationships comprises several subthemes, including: the nature of the caring relationships, their feelings of being a burden to their family, the importance of preserving their privacy, their need to feel supported, and their worries about how their family would cope after their death.
The nature of care relationships
The relationships participants had with their nurses appeared to be very important to them. All participants commented on this, in particular, in relation to whether the use of the DCI had enabled nurses to identify, and meet, their dignity-related concerns. Having a relationship with the nurse meant that participants felt comfortable answering questions in the PDI. Most of the participants recruited to the study had well-established care relationships with CNs and valued this. The development of a safe and trusting interpersonal relationship enabled participants to feel comfortable and confident to raise, and further discuss, dignity-related issues. Key elements of this relationship were showing genuine interest, making them feel important, being active listeners, being compassionate and empathic, being open and honest, and working collaboratively with the participant, as well as, being accessible and available. I mean, as I say when [nurse] comes, we have a laugh and all that, so we're not sitting and talking just about my condition, we're speaking about family life and that, [...] we get on with [nurse] it's nice to have someone we feel relaxed with and we can talk to and we can just be there with … (Penny)
Being a burden to others
On many occasions, participants spoke about their feelings of being a burden to their family and friends. To protect family from their concerns and worries, participants described keeping things to themselves, trying to keep things normal. Nursing actions identified by participants were being able to have these discussions with their nurse, as well as, the nurse listening to them. Even if I'm no feeling fine I just say “yes, I'm fine”, I never go deep into it with them [my family..] Yes, I'd rather speak to somebody else, I'd rather speak to someone outside the family like X my nurse. I don’t want to upset [the family] and they're thinking “oh God”, and “she's all doom and gloom” […] I couldn’t see me speaking to my family like that, I'm no’ saying they don’t understand, but they just want things to go on as normal. (June)
Privacy
One important aspect of dignity that many participants discussed was how their privacy was compromised by their illness. They often related this to personal hygiene and toileting needs, but also, the need to talk about their concerns in private. This privacy violation often led to feelings of embarrassment. Having to shout on a young man just to tell, to help you to try and get you down, up to the toilet and then he’s got to wait ‘til you've had the toilet and then wait on you coming back down, which is not very nice because it's not very dignified, a 30-year-old man having to give his mother a shower … that’s the only thing. (Liz)
Feeling supported
The degree to which people felt supported by their family, friends, and healthcare services was also reported by participant scores using the PDI. It was acknowledged that illness could change interpersonal relationships and impact on how support is given and received. Examples of such support included practical, emotional, and social aspects. Nursing care actions identified by participants included facilitating access to social support services, providing practical advice, and using positive reinforcements. It was the amount of care, we needed, this was before the Marie Curie thing came [...] in of course,, and I wasn’t sure in myself how I could handle it or cope with it, and, she (the CN) then said but if you need more visits for that she says, “then that will happen”, and she solved it that way. (George)
Worries about how family will cope after my death
Three participants mentioned having made preparations for their family, such as funeral and financial plans. Others expressed concerns for the emotional well-being of their family after their death. I’ve put things in place and there were some of the things, and particularly, the one that I did score (on the PDI), I suppose particularly high on, was the concerns for my family after I'm gone. (Kate)
Discussion
The findings of this study provide evidence that the DCI is useful and helpful approach for use by CNs in the context of end-of-life care. Participants described their embodied experience of their illness and found that the use of the DCI by their CNs helped them identify their dignity-related concerns. In particular, the DCI offered an avenue for specific dignity-related needs to be raised and addressed. Notably the use of the PDI by the CNs enabled participants to discuss important issues they would not have otherwise raised. Therefore, it is essential for nurses to prioritize these issues and include them as part of standard care.
The DCI is a valuable tool to help CNs address patients’ dignity-related concerns and also enable CNs to respond to psychosocial concerns in a person-centered manner. This is significant given that psychosocial concerns have previously been identified as difficult for CNs to manage (Griffiths et al., 2007; Law, 2009; Walshe & Luker, 2010).
A key feature of the experience of participants in this study was the need to live day to day or maintain normality, and be in control. This feature has been raised in previous research (Horne, Seymour, & Payne, 2012; Johnston, Milligan, Foster, & Kearney, 2012; Johnston & Smith, 2006) and is a key component of the dignity model (Chochinov et al., 2002). What is novel about the DCI is that it provides practical suggestions as to how nurses can deal with, or respond to, these concerns; and when applied, appears to be well received by patients. This, maybe congruent with the current Advance Care Planning agenda (Blackford & Street, 2012), although, Advance Care Planning discussions need to be invited, dynamic, and ongoing, if embarked upon.
Another issue featured in the patient experience was the interplay between feeling a burden, the personal sense of dignity, and the usefulness of the DCI opening up this discussion in a helpful way. This seemed to be a strong theme and is a recurrent problem that patients often feel they should not raise. Self-perceived burden has been found to be a major concern for people who are nearing the end-of-life, particularly in terms of concern for others and the implications it carries on a self-level (McPherson, Wilson, & Murray, 2007). The DCI allows for a safe, legitimatized start to this conversation—one by asking the question, two by listening, and three by participants knowing “everyone” is being asked about this so they must be vaguely normal to feel that way.
Likewise, privacy was also a strong theme and raising issues within DCI discussion again provided a safe place, and way, for participants to comment. Privacy concerns have been cited as important in end-of-life care (Steinhauser et al., 2000; Teno et al., 2004). While there is little evidence to help nurses and other health care professionals deal with this important concern, the DCI offers nurses a guide to care for privacy concerns effectively.
In a recent international online survey of palliative care professionals views on the use of patient reported outcome measures, respondents reported that patient reported outcome measures helped them better understand patients’ and families’ situations and to monitor change and evaluate interventions (Bausewein et al., 2011). However, the multiplicity of potential tools, lack of training and guidance, time constraints, workload issues, and concerns that patients may be too unwell, cognitively impaired or unnecessarily burdened and distressed, are all barriers for their routine application in practice (Bausewein et al., 2011; Hughes et al., 2004). Despite this, participants in this study found using the PDI acceptable, as a key component of the DCI, and in fact it enhanced the care provided to them by nurses. Furthermore, use of the DCI supported holistic assessment and opened up conversations about emotionally sensitive subjects and legitimatized discussing a wide range of issues that impact on dignity in advanced illness. Many participants in the study had established relationships with the CNs; as such, there were instances when the PDI did not identify unmet dignity-related issues, perhaps validating the care already being provided. For others, however, it helped the CN identify and respond to previously undisclosed dignity-related concerns.
The importance of relationships with healthcare professionals has been identified by palliative care patients as an important influence on positive experiences of healthcare (Kennett & Payne, 2009). Patients identified genuineness, person centeredness, active listening, and being accessible and available as key elements of the nurse–patient relationship (Chapple, Ziebland, & McPherson, 2006; Exley, Field, Jones, & Stokes, 2005; Grande, Farquhar, Barclay, & Todd, 2004). However, few studies have explored the nature of nurse–patient relationships in community palliative care. This study adds to the literature, suggesting that the DCI offers CNs a means of further developing and deepening the nurse–patient relationship.
Limitations and Strengths
This study provided necessary evidence for the DCI to be adopted into routine practice when caring for patients nearing the end of their life. However, as the majority of participants were diagnosed with terminal cancer, the transferability of the study findings to other conditions may be limited. Although the researchers aimed to recruit patients diagnosed with any illness within their final 6 months of life, recruiting participants with non-cancer life-limiting conditions proved difficult. The cross-sectional nature of the study design was also a limitation. A prospective design with serial interviews may have provided insights regarding how dignity-related concerns change and evolve other time.
Clinical Implications
The DCI is a tool for use in clinical practice by CNs offering evidence-based care actions that enhance holistic assessment of patients receiving palliative care. The findings from the evaluation study suggest that it is received well by patients and serves to facilitate a good opportunity for drawing out dignity-related concerns. The reflective questions and suggested care actions enable CNs to have evidence-based strategies for responding to such concerns. Advanced communication skills as well as specialized training are required for CNs to be able to support conversations with patients regarding their dignity concerns. Further research is needed on patients with other chronic conditions, such as heart failure, as well as different settings (e.g., nursing homes), to further test the transferability of the DCI.
Conclusions
As the model of palliative care has moved to a community setting, new challenges were identified in the delivery of end-of-life care by nurses. The findings of this study provide necessary evidence that the DCI allows patients to convey diverse dignity-related needs to CNs. As a key component of the DCI, use of the PDI facilitated patients’ communication of their dignity-related needs to their CNs. Patients expressed increased satisfaction with the support that they received. The DCI is particularly useful in helping CNs to deliver psychosocial care, previously identified as a difficult area for CNs in practice. The use of care pathways detailing interventions to manage clinical problems and ensure systematic integration of the best available evidence into care delivery can improve end-of-life care.
Footnotes
Acknowledgments
We would like to thank all the patients and relatives who gave their time to this study. We would like to thank the steering committee research advisory group and hospice patients advisory group who helped shape the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the support of Dr. Margaret McGuire, Director of Nursing who supported the study and NHS Tayside endowment fund for funding the study.