
Abstract
The aim of this study was to identify factors that serve as facilitators and barriers for breastfeeding among Chuukese immigrant women living in Guam. Traditionally, Chuukese women exclusively breastfeed their babies; however, it is reported that breastfeeding decreases among these women when they migrate to Guam. Little is known about why this happens. A qualitative approach that included key informant interviews and focus groups of Chuukese women (N = 24) who had migrated to Guam and delivered a baby on Guam within the past 5 years was completed. The project interview or discussion guides were guided by the Theory of Reasoned Action and explored facilitators and barriers for successful breastfeeding among these Chuukese immigrant women. Among this population, key facilitators for breastfeeding included high levels of self-confidence, family support, knowledge about breastfeeding, and the existence of strong traditional Chuukese cultural values. Key barriers included experiences of cultural conflict or social change, lack of support from their local community, family and health-care staff, as well as limited self-knowledge about how to manage common breastfeeding problems. Where more facilitators were reported, breastfeeding was more often practiced, and where more barriers were reported, formula feeding was more likely. Social factors, health system policies, and proactive nursing support are important influencing factors for breastfeeding among the Chuukese immigrant population on Guam. Nursing can play key roles in policy, professional leadership and practice, and social advocacy to support breastfeeding promotion and maintenance on Guam.
Introduction
Infant feeding is practiced differently by various groups and societies across the world. Breastfeeding choices are influenced by many factors, including culture, traditions, socioeconomic, family, and personal pressures, to name a few. Historically, as contact with industrialization and westernization occurred formula feeding was introduced and became possible for new mothers across the world. For most newborns, formula feeding is not as beneficial as breastfeeding for infant health and well-being. Riordan and Wambach (2009) report that in many societies some mothers choose to breastfeed their babies for the social and health benefits to themselves and their infants, while others choose not to breastfeed because formula is so easily available and considered convenient to use. The decline of breastfeeding in some countries is of concern to many.
Background or Literature
Breastfeeding has consistently been identified as a leading indicator for infant health worldwide. The advantages of breastfeeding are well documented for both mother and baby (American Academy of Pediatrics, 2016; American College of Obstetricians and Gynecologists, 2016; Association of Women’s Health, Obstetric and Neonatal Nurses, 2015).). On a global level, the prevalence of exclusive breastfeeding among infants 0 to 6 months is only 39%. While this represents an increase from 33% in 1995, there is still much work to be done in this area (Xiaodong, Wardlaw, & Brown, 2012). The U.S. Department of Health and Human Services (USDHHS, 2011) reports that the incidence and duration of breastfeeding in the United States tend to decrease among all racial groups by 5 to 6 months postpartum. We know that Pacific islanders tend to have lower breastfeeding rates in Hawaii. Flood and Dodgson (2010) found that while overall breastfeeding initiation rates in Hawaii are higher compared with the United States (89.6% vs. 70%), Native Hawaiian or Pacific Islanders in the state have much lower breastfeeding initiation rates (46.5%). Exclusive breastfeeding duration rates are also different among the groups. Hayes et al. (2014) found that in Hawaii race or ethnicity was a predictor of exclusive breastfeeding for at least 8 weeks. While for Whites, it was 51.9%, for Native Hawaiians and Samoans it was only 31.8% and 24.2%, respectively. This discrepancy is quite marked. While the U.S. Healthy People 2020 (USDHHS, 2011) series has strived to increase the incidence of breastfeeding across the nation for many decades and recognizes such as an important public health goal, the USDHHS notes that much work is needed to promote breastfeeding among low-income and minority populations that are unlikely to initiate breastfeeding at birth or continue through the infant’s first year of life.
The six USAPI jurisdictions include over 104 inhabited islands and low-lying atolls, and cover a geographical expanse greater than that of the continental United States (Levin, 2008). Chuuk is a state within the Federated States of Micronesia which is part of the U.S.-Affiliated Pacific Islands (USAPI). The history of the relationship between the United States and the USAPI jurisdictions is important. Historically, policies enacted by both the United States and the individual jurisdictions have significantly impacted health systems, outcomes, and breastfeeding patterns in the region.
Migration Within the USAPI
The United States is a nation of immigrants. There is significant movement within the USAPI, and between the USAPI, the U.S. states, and territories. Situated in Micronesia in the Western Pacific Ocean, Guam serves as the most developed USAPI territory (Bureau of Statistics and Planning, 2012). Many of the USAPI residents including those from Chuuk migrate to Guam. Most come to Guam for employment or education, seeking better lives for themselves and their families. Unfortunately, most tend to be less educated, employed in low-paying jobs, and live at or below the poverty level in comparison to usual Guam residents. It is estimated that there are 17,974 Chuukese living on Guam which represents 11.2% of the total population (Bureau of Statistics and Planning, 2012). Chuuk state is comprised 40 small islands that are organized within nine groups. The population of the islands varies widely (13,000 on Weno to 267 on Etal). While the built environment of Chuuk is quite austere (power outages are frequent, roads are poor, and Internet connectivity is unpredictable in some islands and absent in others), the natural environment is quite beautiful. The Chuukese people have a rich culture and traditions, and most lead simple lives. The pace of life is much slower, and many fish and harvest their own food. The societal structure is matrilineal, and many live in extended families.
Guam is a U.S. territory with a population of 159,358 (Guam State Data Center, 2014). Health-care needs are provided by three hospitals (one military and two civilian). All three hospitals provide obstetric services. Additionally, one birthing center provides obstetric services to military and civilian mothers. The vast majority of mothers deliver in hospitals versus the birthing center or home environment. Prenatal and postnatal care are provided by numerous health-care clinics. Services for low-income mothers are generally provided by three community health centers. Mothers who meet eligibility are provided Women Infants and Children (WIC) services.
Exclusive breastfeeding of newborn infants is the norm in Micronesia, and in Chuuk, 79% of infants are still breastfed at the age of 6 months (UNICEF Pacific, 2013). However, data derived from recent Guam public health reports indicate that among Chuukese immigrants on Guam only 28.5% exclusively breastfeed at birth, and by the first follow-up appointment, less than 1% are still exclusively or predominantly breastfeeding (Guam Department of Public Health and Social Services, 2016). This represents an alarming deviation from the usual breastfeeding patterns seen in Micronesia. It is important to understand factors that contribute to this low rate of initiation and subsequent marked drop off in breastfeeding rates among this immigrant group on Guam.
Method
Purpose of the Study
The study aimed to gain a better understanding of facilitators and barriers for breastfeeding among Chuukese migrants on Guam.
Research Design
This was an exploratory, descriptive study, utilizing a qualitative approach, and included key informant interviews and focus groups. Key informant interviews were completed first and included health-care workers and Chuukese mothers who had delivered infants on Guam. The health-care workers included one nurse who is also an international board certified lactation consultant, one nutritionist who is a lactation consultant, and one Chuukese community health worker. All health-care workers had a history of working with Chuukese mothers for many years. Six Chuukese mothers also served as key informants; three breastfeeding mothers and three formula feeding mothers. Focus group sessions followed and included 8 breastfeeding mothers and 10 formula feeding mothers.
Theoretical Basis of the Study
The study was guided by the theory of reasoned action (TRA; Ajzen & Fishbein, 1980; Fishbein & Ajzen, 2010). The TRA posits that a person’s attitudes or personal judgment regarding a behavior combined with perception of social pressures by significant people are key to identifying an individuals’ intent to perform the proposed behavior.
Operational Definitions
For the purpose of this study, infant feeding was defined in two ways. Breastfeeding was defined as either exclusive breastfeeding or breastfeeding combined with formula or other foods with 50% or more of feedings from breastmilk. Formula feeding was defined as either formula feeding exclusively or 50% or more of nutrition through formula feeding.
Sample and Setting
Participants who met inclusion criteria (aged 18 years or older, migrated from Chuuk to Guam within the past 5 years, delivered a live infant on Guam during that period, and provided nutrition to the infant) participated in the study. Participants spoke English to the extent that they could understand the spoken words in the discussion and reply in English. A total of 24 Chuukese women (breastfeeding n = 11, formula feeding n = 13) participated. Three Chuukese translators explained any concept that required clarification. These translators were born and raised on Chuuk and were currently attending college on Guam (one was an English major, one a nursing major, and one a public health major). Each was fluent in Chuukese, and each had passed an English proficiency test. The study was conducted in the northern, central, and southern villages in Guam.
Data Collection
Using procedures outlined by Morgan (1997) and Krueger & Casey (2009), key informant interviews (nine) and focus groups (six) were conducted to determine the facilitators and barriers for breastfeeding among Chuukese mothers on Guam. Findings from the key informant interviews (that were guided by the TRA) were used to inform the development of the focus group script questions for the study. Specific study steps included (a) development of the demographic data tool based on TRA concepts, (b) content validity of the key informant and focus group interview guide by maternal-child content experts, (c) cognitive testing of all tools with Chuukese mothers to ensure understandability of the words and questions, (d) development and pilot testing of the demographic data tools and interview guide questions, (e) conduct nine key informant interviews, five focus group interviews, and one final follow-up validation focus group.
Ethical Considerations
Institutional Review Board approval from the University of Hawaii, Office of Research Compliance Human Studies Program, and the University of Guam Committee on Human Research Subjects was obtained prior to initiating the study.
Data Collection and Analysis
Demographic data collected included age, marital status, extended family information, length of residence in Guam, education, income, and prenatal care. This data were entered into the Statistical Package for the Social Sciences (IBM Corp, 2012, p. 21). Descriptive statistics were used to describe the participants. Qualitative data were collected via interviews that were audio recorded. The recordings were reviewed multiple times by the researcher to gain an understanding of what was being stated by each participant. Using an approach as described by Granheim and Lundman (2004), all ideas and concepts were listed as stated by the participant. Then initial thematic coding analysis was completed by the primary researcher. Afterwards, the data were also reviewed by one other research collaborator and one Chuukese research assistant.
Rigor and Trustworthiness
Manifest (obvious components) and latent (derived from interpretation) content formed the basis for analysis. The process facilitated deriving meaning from the text. Meaning units were composed of related words or statements made by participants. The meaning units were then condensed to shorten the statements, while still preserving the basic unit. These condensed statements were further refined to arrive at codes, categories, and then themes which allowed for the final determination of the impact of the factors on breastfeeding. Where the reviewers were not in full agreement with the coding, discussion occurred until full agreement was achieved. When the three reviewers agreed, the data analysis process was considered to be complete.
Findings
Demographics
Demographic Summary for the Focus Group Mothers.
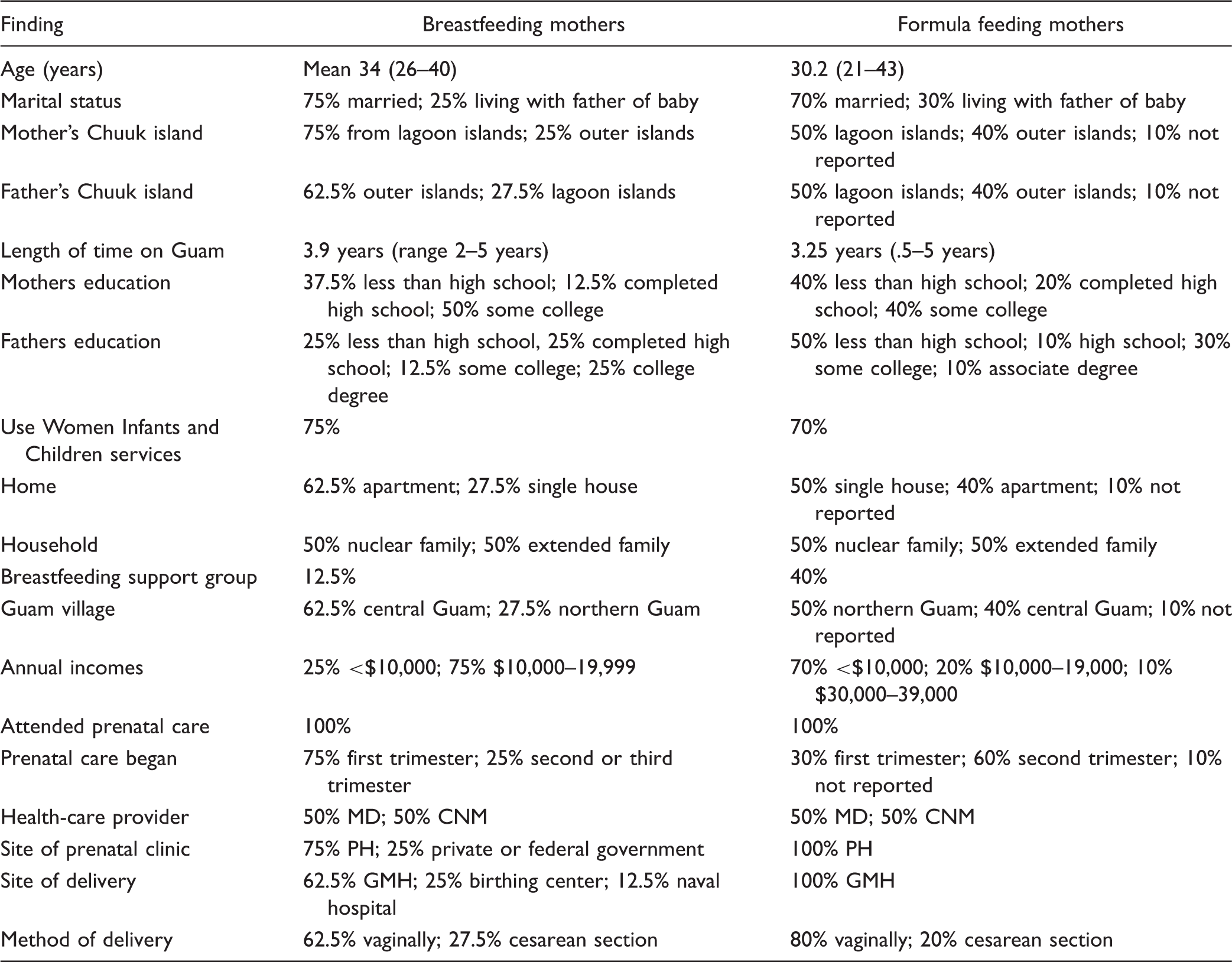
Note. MD = physician; CNM = certified nurse midwife; PH = Public Health Department; GMH = Guam Memorial Hospital.
Factors That Influence Breastfeeding
Facilitators and barriers were described by both groups of mothers. As expected, more facilitators were reported by the breastfeeding mothers, while the formula feeding mothers reported more barriers for breastfeeding.
Facilitators
Five key themes that describe facilitation of breastfeeding emerged (a) positive attitude shaping for breastfeeding, (b) confidence in abilities, (c) support from family and health-care staff for breastfeeding, (d) knowledge acquisition about breastfeeding, and (e) traditional values toward breastfeeding.
Attitude shaping
Breastfeeding mothers identified many advantages to breastfeeding which led to the shaping of positive attitudes toward breastfeeding. The mothers reported that when they weighed the advantages and disadvantages to breastfeeding, the positive advantages influenced their positive attitude for breastfeeding. One mother relayed, “Breastfeeding is better because it comes from us. Mothers breastfeed on my island. I knew I should breastfeed from when I was a little girl. I saw others breastfeeding.” These findings suggest that when attitudes are positive and other social circumstances are positive, breastfeeding follows.
Confidence
Confidence was found to be an important facilitator. The breastfeeding mother group more often reported a strong sense of confidence that they would be able to successfully breastfeed their infant. This confidence was not found in the formula feeding mothers.
Support from family and health-care staff
This theme was linked to self-control over infant feeding choice. Breastfeeding mothers indicated that they felt control over breastfeeding when there was positive breastfeeding support from family or health-care staff. They reported that they experienced few problems but felt that when problems did occur they received support from family and health-care staff and they were able to address these problems. One mother said, “I knew I could breastfeed. If there were any problems, someone would help me.”
Knowledge acquisition
Knowledge acquisition from trusted persons and life experiences that were supportive of breastfeeding were recurring themes that impacted behavioral beliefs and subsequent infant feeding choice among the breastfeeding group. The Chuukese mothers primarily acquired information from trusted individuals close to them and also from life experiences related to breastfeeding, such as witnessing many women in their community in Chuuk openly breastfeeding. It was reported that the grandmother of the infant was particularly important as a source of encouragement and support for breastfeeding their infant. A breastfeeding mother reported, “My mother spent time helping me to breastfeed.”
Traditional values
Traditional Chuukese values and family were identified as key components for supporting intentions to breastfeed. Traditional values (including family traditions) influenced the mothers’ normative beliefs and subjective norms. They wanted to respect what they believed to be their family’s traditional values related to breastfeeding. One mother noted that, “Families expect mothers to breastfeed their babies.” Another mother reported “If you are from Chuuk, and you breastfeed your baby, you are a good mother.”
Mothers in the breastfeeding group more frequently reported following tradition when determining the duration of the breastfeeding experience. Most indicated an intent to breastfeed for at least 1 to 2 years with the mother and infant controlling the length of the breastfeeding experience. Only the introduction of solid food, work, or additional pregnancies would be likely to change their intent.
Barriers
More barriers than facilitators were identified for the formula feeding group. The key themes that represent barriers to breastfeeding included the following: (a) cultural conflict or social change, (b) time commitment required for breastfeeding, (c) lack of family support, (d) lack of community support, (e) lack of health-care support, (f) inadequate knowledge related to breastfeeding, and (g) mixed messages.
Cultural conflict or social change
The mothers explained that while there is a strong tradition for breastfeeding within the Chuukese culture, economic needs made working outside of the home an over-riding importance. This need to work creates cultural conflict and social change within the family. Working mothers reported that use of formula made it easier for them to work, and they also believed that their family supported formula feeding their infants while they worked. One mother said, “Breastfeeding is easy. My family cooks for me. But I need to work. When I work, they need to give formula.” Like the breastfeeding feeding mothers, the formula feeding mothers indicated that it is traditional to follow their perception of family values and beliefs.
Both breastfeeding and formula feeding mothers reported reluctance for breastfeeding in public. Despite the fact that in Chuuk breastfeeding in public is commonplace, on Guam it is not. Participants felt that breastfeeding in public was not socially acceptable or the norm on Guam. One mother explained, “Sometimes breastfeeding is hard because showing my breast in public to breastfeed is hard.”
The formula feeding mothers reported a shift in their social norm. They reported a belief that breastfeeding was easy, and best for the infant, but they also reported that the use of formula gave them a sense of independence, and a socially acceptable way to leave the infant with family while they spent time away from the house. These mothers experienced cultural and social conflict when considering the economic need to work, advantages and disadvantages to breastfeeding.
Time commitment required for breastfeeding
The amount of time breastfeeding requires emerged as a barrier for intentions to breastfeed. Working Chuukese mothers had less time available for breastfeeding. One key informant summarized, “The new generation has lost the essence of patience. They want everything instantly. Formula is the new fast food.”
Lack of support from family, community, and health care
Lack of support for breastfeeding was most commonly reported among formula feeding mothers and served as a significant barrier for breastfeeding. This lack of support was experienced at multiple levels. One mother noted that her family told her to formula feed the infant when she expressed a concern that she did not produce enough milk. Without positive breastfeeding support from her family to manage this common problem, the choice to use formula was made. Another mother indicated that she wanted to breastfeed, but her mother had died before the infant was born. Without her mother to support her breastfeeding, she gave up and fed formula to her infant.
On the community level, a serious barrier for breastfeeding was identified. The mothers reported that on Guam there is little or no support for breastfeeding or pumping outside of the home (e.g., workplace or college). This posed a problem when they were working or going to school. One formula feeding mother stated, “When I started working, there was no place to breastfeed or pump milk, so I gave formula.”
Many of the participants (both breastfeeding and formula feeding) reported a lack of breastfeeding support from the local health-care staff. One mother reported that when she could not get the baby to latch on, the nursing staff were not able to help her address the problem. Therefore, she felt that she had to give her baby formula. This mother reported feeling powerless to solve the problem. She said, “How a baby is fed is important. I try not to think about this, though, because I couldn’t get my baby to breastfeed. No one helped.” Other mothers indicated that they thought they did not have enough milk to breastfeed and when they reported this concern, the nurses quickly gave the mothers formula for their babies. Some mothers reported that they were able to breastfeed in the hospital, but when they were discharged from the hospital before their infant was—the nurses fed the infants formula without waiting for them to come from home with their breastmilk. One mother tearfully stated, My baby started to breastfeed, but she had to stay in the hospital after I was discharged. When I visited her and tried to breastfeed, she didn’t want to. I told the nurses, but they didn’t do anything to help. They gave me formula to feed to her.
Several mothers also discussed the formula as a gift. While they initially planned to breastfeed their infants, the nurses brought formula to them to give to the infant while in the hospital. Within the Chuukese culture, it is rude to refuse a gift, so they gave the formula to the infant. They also believed that since the nurse was the one to give the formula, it must be as good or even better than breastmilk. They then fed the infant formula because they thought it was best for the infant. These practices by the nurses served to turn breastfed infants into formula fed infants.
Inadequate knowledge related to breastfeeding
Some mothers reported that when they experienced problems such as believing that they did not have enough milk, or their nipples were sore from breastfeeding, or could not get the infant to latch on, there was little or no support from the nursing staff to address these common issues. This resulted in reverting to formula feeding the infant. They also reported that they did not know that breastmilk was nutritionally superior for their infants. As one mother said, “Both breastmilk and formula are the same. Formula is given when I don’t make enough breastmilk or the baby doesn’t like to breastfeed.”
Mixed messages
The formula feeding mothers reported receiving many mixed messages from their families as well as the health-care providers. For example, some mothers stated that they were told by their family that breastfeeding was best, but that formula was also okay. Mixed messages also came from WIC Program staff, where mothers were encouraged to breastfeed, but formula was provided to them free of charge. Nurses in the hospital also sent mixed messages and routinely provided formula when mothers indicated their desire to breastfeed. These mixed messages resulted in uncertainty with regard to breastfeeding being the best method for infant feeding.
Discussion and Recommendations for the Future
Discussion
The TRA was a useful model for examination of facilitators and barriers for breastfeeding. Attitudes or personal judgment regarding a behavior combined with perception of social pressures by significant people are key to identifying an individuals’ intent to perform the proposed behavior. The social pressures of culture and tradition, positive attitudes, and self-confidence (that was reinforced by support from the more experienced women—like the grandmother) were found to serve as facilitators for successful breastfeeding. Those who had positive attitudes and confidence for breastfeeding were able to overcome difficulties with breastfeeding and continue to breastfeed. The social support from family and friends is important for successful breastfeeding among this immigrant group. The maternal grandmother of the infant is particularly important to support breastfeeding. Where support from family and friends are lacking, formula feeding often follows. Cultural conflict, social change, and economics also serve as significant barriers to breastfeeding. When mothers strive to fit in to the new cultural environment, they often chose what they perceive as the modern way, which for some is formula feeding. When mothers need to work, breastfeeding often requires a larger time commitment than these women can provide, and mothers were often not even aware that policies were available to support breastfeeding in the workplace. Anderson et al. (2015) found interpersonal communication about breastfeeding in the workplace lacking between employees and employers due to age (mothers are younger), gender (mothers are female), and employment rank (mothers are more commonly at beginning ranks). These factors limited the ability of the mothers to make their needs known, as they were afraid to speak up. The authors highlight the importance of interpersonal communication to ensure that employees and employers both know of the needs of employees. This will take breastfeeding support to a higher level that addresses both equity and diversity.
The messages about breastfeeding that are given to these immigrant mothers emerged as being extremely important. Mixed messages from family, health-care staff, and nurses can serve to reduce breastfeeding and promote formula feeding. When a mother is encouraged to breastfeed but then provided with formula, confusion about what is best for the infant results. In addition, breastfeeding education for these mothers must be culturally appropriate. Riordan and Gill-Hopple (2001) noted that breastfeeding education must be in alignment with the learners’ culture and is best when it comes from within the culture itself. During this study, no evidence was discovered that described culturally tailored or relevant breastfeeding education for these mothers. This might be an explanation for why breastfeeding was less common when the infants’ grandmother was not available to teach the mother. The health-care system needs to serve as a proxy when such support is not available to a new mother. Hawley et al. (2015) in their study of mothers in American Samoa proposed that as health-care members sought to promote breastfeeding, the positive aspects of breastfeeding were highlighted, but the management of common problems was not discussed. This led to mothers feeling ill prepared to manage common problems such as sore nipples and perceived lack of adequate milk supply. The authors suggest that discussion of the positive, as well as the challenging aspects of breastfeeding needs to be included in discussions with new mothers.
Surprisingly, the most significant barrier to successful breastfeeding was lack of support from the health-care community. Mothers believed that while they were encouraged to breastfeed, the nurses more often seemed to support formula feeding. When faced with separation from their babies, or encountering common problems with breastfeeding, some mothers in this study reported that did not feel support from the nurses for continuance of breastfeeding and reported that they received little assistance with addressing problems. These barriers that came from the health-care community, especially from the nursing profession are alarming, but somewhat consistent with the findings of Marks and O’Connor (2015). These researchers examined the attitudes of health professionals’ in Great Britain toward breastfeeding and found that this group of workers felt that their role was to inform rather than promote breastfeeding. Mere provision of information is not enough to support breastfeeding among any group. What is required is culturally appropriate support and education that is in alignment with the traditions and values of the mother. Ward and Byrne (2011) in their critical review of the literature addressed the need for continuing education for nurses and midwives providing breastfeeding support. They found knowledge and attitudes, clinical practices and skills, and counseling to be key concepts to include in the education programs. They found several programs based on the 18-hr United Nations Children's Fund (UNICEF), the 40-hr World Health Organization (WHO) course, and the 20-hr WHO/UNICEF course. Resistance to change and sustainability of changes were key to successful exclusive breastfeeding. Ongoing staff education needs to be developed to address these issues.
While a breastfeeding policy exists in the main hospital on Guam, the practices there as well as in the WIC clinic to allow liberal use of formula is contrary to international and U.S. standards for infant feeding. Many of the practices reported are not in alignment with the Baby Friendly Hospital Initiative (Baby Friendly USA, 2016). Initiation to such would likely go a long way to promoting breastfeeding on Guam. Another strategy to improve breastfeeding was reported by Jurkowski, Svistova, Nguyen, and Dennison (2016). Their qualitative study sought to determine the response of health-care providers to New York states’ mandate that all hospitals providing maternity care publicly disseminate their infant feeding statistics. This mandate prompted positive measures to improve breastfeeding support and awareness among staff and administrators. This strategy could serve to improve breastfeeding on Guam.
Recommendations for the Future
These findings are consistent with other populations who migrate from other developing countries (Condon & McClean, 2015).It is important to recognize and address the social and cultural isolation that is often experienced by Chuukese immigrants on Guam, and how this has a negative impact on breastfeeding rates. Newly pregnant women should be assessed for the presence of a culturally appropriate support system that can facilitate the role of motherhood, including breastfeeding. For those who do not have such support in place, follow-up care at home, including support systems need to be developed. This might include peer counselors of the same ethnicity who the new mother can turn to for assistance as well as integration of Chuukese grandmothers for breastfeeding support during the prenatal and postnatal care timeframes. Many such groups can be formed through faith-based organizations or local community centers.
Policy makers must do their part as well. Health-care policies regarding breastfeeding need to be enforced. While breastfeeding policies exist within the territory of Guam, enforcement is lacking. The Nana Yan Patgon Act (2013) addresses assuring privacy and access to breastfeeding in public and in the workplace. This act needs to be fully implemented and enforced. The WIC program in Guam needs to reassess its policies regarding the distribution of formula. Formula feeding of infants should be initiated only when necessary.
These findings represent important issues that need to be addressed. The hospitals and clinics need to integrate Baby Friendly Initiatives into their policy structure and ensure that compliance is in place. The health-care system needs to proactively promote and support breastfeeding. Nurses in the hospital, community, and public health settings must endorse the concept that breast is best, support mothers to every extent possible, and seek out lactation consultant resources for difficult cases. Lactation consultants are crucial to providing both education and support to health-care workers and nurses to assist mothers to successfully breastfeed their infants. More lactation consultants need to be educated and utilized in the territory, including women of the same ethnicity. Nursing as a profession needs to lead the way to improving breastfeeding in Guam as well as in all parts of the world. Employers must assure that the nurses and other practitioners in the maternal child sector have adequate competencies related to support for breastfeeding. Hospitals on Guam should assess their policies regarding the distribution of free formula samples on maternity units, and consider a policy that requires a prescription for formula use within the hospital. Local pediatricians, primary care, and WIC clinics need to actively promote and support breastfeeding of all infants. Nursing education programs must assure that breastfeeding is an important element in the maternal or child curriculum of nursing school. Ongoing continuing education regarding breastfeeding is essential for all types of health-care workers who are engaged in maternal child care services.
Future Research
Additional research needs to be undertaken to get a better understanding of how to promote facilitators and reduce barriers for this vulnerable group, as well as other groups of immigrants on Guam. An exploratory study to discover what happens regarding breastfeeding with second generation Chuukese mothers on Guam would provide an understanding of how these patterns change across generations. A replication study could be completed to include a sample of non-English speaking Chuukese mothers to examine the relationship between language and breastfeeding patterns. It is also important to examine breastfeeding patterns among other cultural groups who are living on Guam as this would provide data for larger generic breastfeeding promotion programs. Researchers on the mainland United States should examine breastfeeding patterns among Micronesian immigrants in their states. While most breastfeeding research has focused on mothers, it would be interesting to examine factors for fathers (e.g., knowledge, values, beliefs, and level of support about breastfeeding) in relation to breastfeeding of infants. A study to determine how health-care staff perceive their role in breastfeeding and factors that influence levels of support for breastfeeding would provide a starting point for education and policy development. Intervention studies that aim to develop and implement culturally tailored interventions to promote breastfeeding among Chuukese (and other immigrant women) would serve to identify what works. Such studies must surely include all levels of health-care workers engaged in women’s and children’s health. Finally, studies that examine facilitators and barriers for health policy to support breastfeeding need to be conducted. Barriers identified can then be addressed through public programming.
It takes a whole community to support an infant as it grows and develops to become a healthy child. Community support for breastfeeding is one of the first steps in this process. Community includes the government, the health-care system, the nursing profession, local communities and organizations, the mothers, and their families. All have a part to play. As Griswold (2016) outlined in her address to the 2016 International Lactation Consultant Association, three core values are needed for successful breastfeeding support: knowledge, diversity, and equity. Addressing these core values can make significant progress to transform world health.
Footnotes
Acknowledgments
The authors wish to thank the Chuukese mothers who gave their time and knowledge to make this study a possibility.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.