
Abstract
This study evaluated patient experience in a private hospital in Costa Rica using the Picker Patient Experience Questionnaire-33 (PPE-33). A digital survey administered via Qualtrics® targeted patients treated in emergency, surgical, or inpatient units between November 2024 and February 2025. A total of 567 valid responses were analyzed, exceeding the required sample size. The mean PPE-33 score indicated a satisfaction rate of 67.6%. The lowest-rated dimension was Patient Rights (27.9%), with few patients reporting being informed about their rights. In comparison, higher scores were observed for patient information (90.4%) and for confidentiality, privacy, pain management, and care (82.0%). Statistically significant differences were observed only by occupational status (p = .0122), with no variation by sex, age, educational level, or marital status. The emergency department consistently showed the lowest ratings across several dimensions. Overall, the findings highlight strengths and persistent gaps in patient-centered care and support the use of digital surveys as a feasible tool for monitoring patient experience and guiding quality improvement efforts in similar private hospital settings.
Keywords
Introduction
Patient experience is a critical indicator of person-centered care and healthcare quality. 1 In this approach, the emphasis is on the collaborative relationship between healthcare professionals, patients, and their families or caregivers throughout the entire care process. 2 Within this model, patients are encouraged to participate actively in therapeutic decision-making and comprehensive care planning, fostering a sense of shared responsibility.3,4
The concept of patient experience encompasses the emotions and perceptions of patients, their families, and other stakeholders regarding healthcare processes, structures, and outcomes. A growing consensus highlights the importance of integrating these perspectives to achieve high-quality care. 5 Effective patient journey management ensures safety, efficiency, and optimal resource use, whereas poor coordination increases risks and diminishes perceived quality.6,7 Even in the face of significant clinical and technological advances, patient experience remains central to effective healthcare delivery.8,9
Although often used interchangeably, “patient satisfaction” and “patient experience” are distinct concepts. Satisfaction is primarily associated with perceived clinical outcomes. In contrast, experience reflects the actual interactions between patients and the healthcare system. 10 Measuring patient experience remains methodologically challenging due to the absence of a universally accepted definition. While terms such as “perception” or “satisfaction” are frequently used as substitutes, experience is considered less subjective and more focused on observable aspects of care. Multiple factors, including demographic, socioeconomic, cultural, perceived health status, and characteristics of the care received, have been shown to influence these experiences.11,12
Quality of care has become a key differentiating factor among private hospitals, many of which offer clinically similar services. 13 In this context, quality is defined through multiple dimensions relevant to patients, including physical infrastructure, clinical competence, geographic accessibility, and waiting times.13,14 Although it may introduce certain biases, user satisfaction cannot be overlooked when analyzing healthcare choices, as patients are the only actors who experience the care process in its entirety.6,15
Several validated instruments are available to measure patient experience, including SERVQUAL, CAHPS®, and the Picker Patient Experience (PPE) Questionnaire.16–18 The original PPE included 40 core items, with the possibility of adding up to 100 additional questions tailored to the specific medical center, but its lack of universality limited widespread use. 18
To overcome this limitation, the Picker Institute developed the PPE-15, a condensed version with 15 core items applicable across institutions and populations. The PPE-15 allows standardized comparisons, longitudinal monitoring, and the generation of actionable insights. Building on this foundation, Barrio-Cantalejo et al. created and validated the PPE-33, an expanded version that incorporates additional dimensions related to the quality of information provided and patient involvement in decision-making. 19
Method
Study Design and Setting
This study employed an observational, descriptive, and retrospective design using a self-administered digital survey distributed via the Qualtrics® platform. Data collection was conducted at two locations of a private hospital located in X and Y, Costa Rica. The survey targeted patients who received care in emergency, surgical, or inpatient services between November 2024 and February 2025. Survey administration took place from May 20th to June 17th, 2025, following Ethics Committee approval.
Inclusion and Exclusion Criteria
A stratified random sampling design was employed, stratified by site of care (X or Y) and type of service (emergency, surgical, or inpatient). Eligible participants were required to be 18 years of age or older and to have received medical care during the reference period. The survey was sent only to individuals who had previously authorized the hospital to contact them for institutional purposes. Questionnaires were excluded if incomplete or if informed consent was not obtained.
Study Population
The reference population comprised 11,132 patients who received care at the selected services at both locations between November 2024 and February 2025. To maximize response rates and ensure representativeness, the survey was distributed to all eligible patients. The minimum required sample size was 372 valid responses, estimated at the 95% confidence level with a 5% margin of error. Ultimately, 567 valid questionnaires were obtained, exceeding the minimum target.
Data Collection
Patient experience was assessed using the Picker Patient Experience Questionnaire-33 (PPE-33). This validated instrument evaluates multiple dimensions of patient-centered care, including patient rights, understanding of medical condition, clarity and method of information delivery, staff empathy and accessibility, discharge information, confidentiality and privacy, pain management, and overall quality of care.
At the beginning of the survey, participants were informed of the confidentiality of their responses and given the option to withdraw at any point or to indicate if a question did not apply to their situation. Items 21 and 22 were analyzed separately because their responses were qualitative.
Statistical Analysis
All variables, except for items 21 and 22, were coded to assign a score, with each favorable response receiving a value of 1 and each unfavorable response a value of 0. This coding allowed for the calculation of mean scores at the participant, item, and dimension levels.
Comparisons were then made across sociodemographic categories, including sex, age group, educational level, marital status, and occupation. A one-way analysis of variance was used to assess differences between groups, while Student's t-tests were employed to compare mean scores between campuses and services. An alpha level of 0.05 was applied in all tests. Statistical analyses were conducted using RStudio, version 4.3.0.
Ethics Approval
The study was approved by the Ethics Committee (CEC-HCB; approval No. CEC-HCB-0340-2024; approved October 21, 2024).
Results
Patient Demographics
A total of 567 valid questionnaires were analyzed, exceeding the initially established minimum number of participants (372). Regarding sex distribution, 56.2% of participants identified as female and 43.8% identified as male. Most respondents (43.4%) were aged 18–44, followed by 36.2% aged 45–64 and 20.5% aged 65 or older. In terms of educational attainment, the largest group consisted of individuals with postgraduate studies (55.7%), followed by those with undergraduate education (22.9%).
With respect to marital status, more than half of the participants (51.5%) were married, while 24.9% were single. Concerning occupation, 35.7% reported being employed, 28.8% identified as professionals, and 17.3% were retired. A detailed presentation of sociodemographic characteristics is provided in Table 1.
Sociodemographic Characteristics and PPE-33 Scores by Sex, Age, Educational Level, Marital Status, and Occupation.
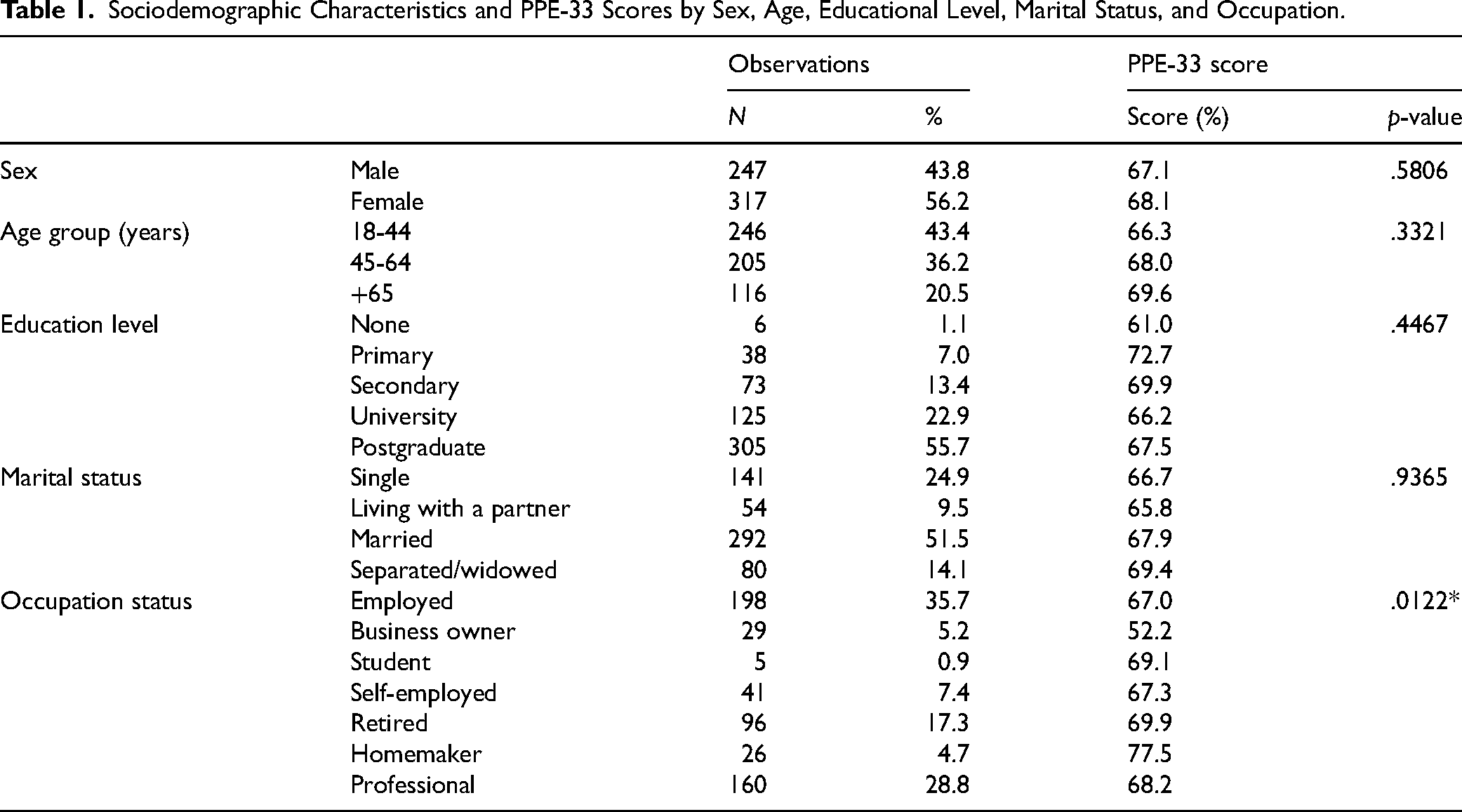
Table 1 shows a statistically significant difference (p = .0122) in PPE-33 scores only by occupation, with mean values ranging from 52.2% among business owners to 77.5% among homemakers. In contrast, no significant differences were observed by sex (p = .5806), age group (p = .3321), educational level (p = .4467), or marital status (p = .9365). These results suggest that the hospital provides consistent quality of care across most demographic groups, although differences by occupation may warrant further examination. Finally, the Student's t-test comparing mean patient satisfaction between the two hospital campuses revealed no statistically significant difference (p = .6856), indicating that perceived quality of care was similar across both sites.
Patient Experience Evaluation
The mean scores for each dimension of patient experience, as assessed by the PPE-33 questionnaire, were distributed as follows: the highest-rated dimensions were “How the patient was informed” (90.4%), “Confidentiality, privacy, and consideration of pain, and care” (82.0%), and “Comprehensibility” (77.2%). Conversely, lower scores were observed for “Empathy of informants” (63.4%), “Information upon discharge” (64.0%), and, most notably, “Patient's Rights,” which recorded the lowest score (27.9%). These results underscore both strengths and areas requiring improvement in the delivery of person-centered care. Table 2 presents a more detailed breakdown of the item scores for each dimension.
Percentage Distribution of Responses to the PPE-33 Items in the Study Group.

Patient's Rights
Assessment of knowledge of patient rights was the lowest-scoring area in the evaluation, with an average score of 27.9%. Survey results showed that fewer than one-third of respondents reported receiving information about key aspects of their patient rights. Specifically, only 25% indicated being informed about the letter outlining patients’ rights and duties, 30% about their right to refuse treatments or tests, and 25% about their right to access the information recorded in their medical history.
Patient's Condition
The dimension “Patient's Condition,” which explores patients’ understanding of their illness, obtained an overall score of 68.8%. While it is encouraging that 80% of patients (Q4) reported receiving information about their condition or illness, only 70% (Q5) reported being informed about the effects of their treatment. Most concerning, only 56% (Q6) reported receiving information about the potential risks associated with diagnostic tests. These findings highlight the need to strengthen clinical communication regarding both potential risks and treatment effects.
Comprehensibility
The “Comprehensibility” dimension achieved an average score of 77.2%. Most patients reported receiving clear, easy-to-understand answers when asking physicians (Q7: 87%) and nurses (Q8: 84%) questions. However, only 61% (Q9) indicated that they would have liked to participate more in decisions related to their care and treatment. These findings point to effective communication in response to patient inquiries but also highlight the need to strengthen shared decision-making processes.
How the Patient Was Informed
The “How the patient was informed” dimension scored 90.4% overall, but specific items raised concerns. For Q10, 86% of patients reported receiving contradictory information from healthcare staff. Similarly, 94% of patients (Q11) indicated that physicians spoke as if they were not present. These findings highlight significant issues with communication coherence and patient inclusion in clinical discussions, despite the high overall score for the dimension.
Empathy of Informants
The “Empathy of informants” dimension obtained an overall score of 63.4%, reflecting heterogeneous results. While 80% of patients considered the consent document easy to understand (Q15), only 64% indicated that a physician had discussed their concerns or fears regarding their health or treatment (Q12), and just 49% reported receiving such support from a nurse (Q16). In addition, 56% found a staff member with whom they could discuss their concerns (Q17). Regarding support in the informed consent process, 71% stated that a professional helped them understand the document (Q14). These findings suggest clear opportunities to improve the active identification of patient concerns and to create spaces for empathetic communication among healthcare staff.
Accessibility of Informants
The “Accessibility of informants” dimension obtained an average score of 66.9%, indicating generally positive results, though with areas for improvement. Seventy-five percent of patients reported that it was easy to reach their physician to clarify questions (Q19), and 74% indicated that their relatives or close contacts were able to speak with the physician when needed (Q20). However, only 60% reported that healthcare professionals actively encouraged them to ask questions about their illness or related aspects (Q18), suggesting opportunities to further strengthen staff proactivity in fostering patient participation.
Figure 1 illustrates the distribution of responses to questions 21 and 22, which used a different response format related to the provision of information by healthcare staff. Question 21 asked who usually received information during the patient's hospital stay. Results showed that 35% of patients reported receiving the information directly, 10% indicated it was provided to their relatives, 15% stated it was given to both them and their companions, and 27% noted that it depended on the circumstances.
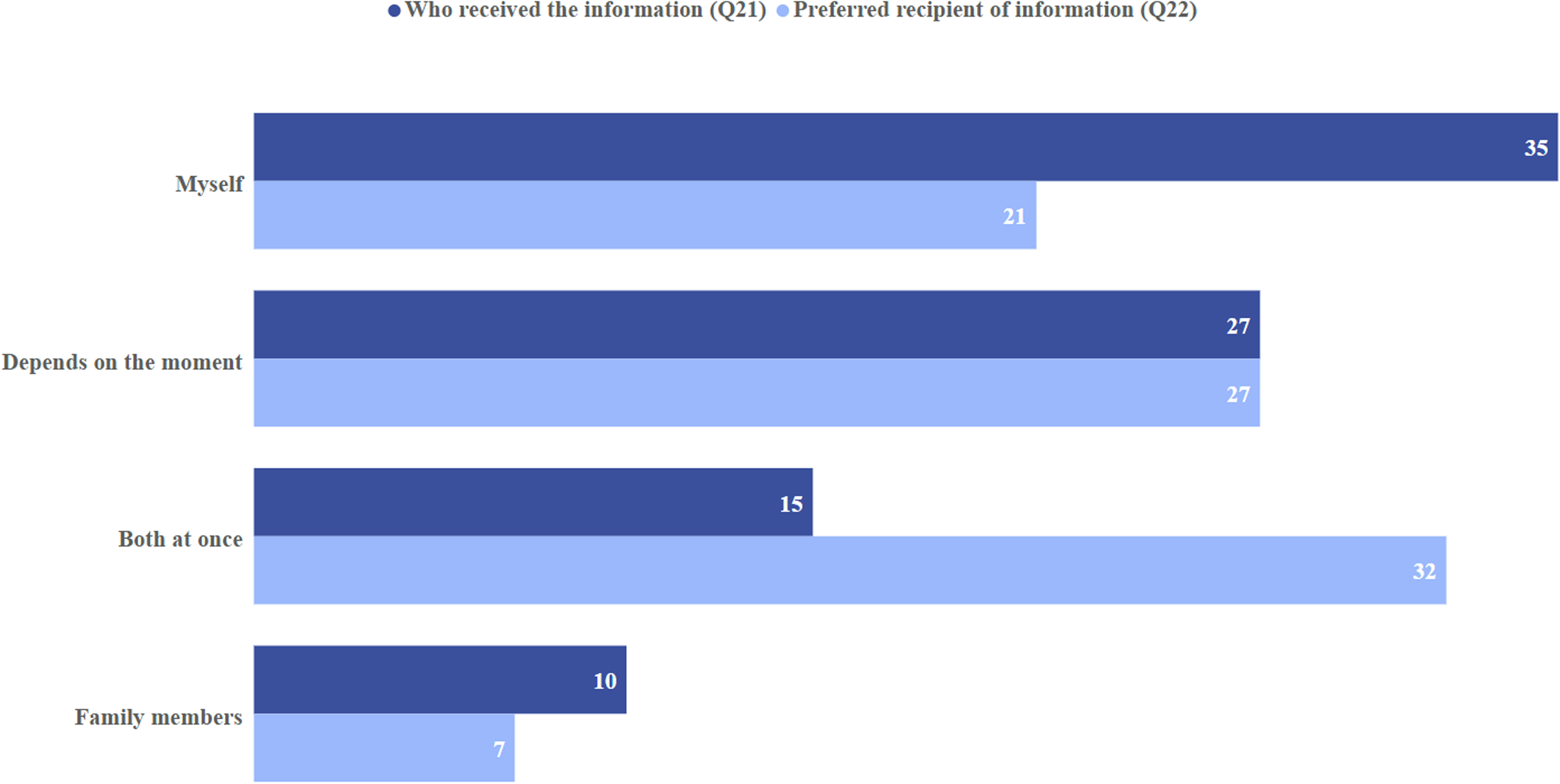
Comparison of current practices and patient preferences regarding recipients of medical information (Q21 and Q22).
Conversely, question 22 explored patients’ preferences regarding who should receive this information. Responses revealed that 21% preferred to receive it directly, 7% preferred it to be given exclusively to a relative, 32% indicated that they would prefer it to be delivered to both simultaneously, and 27% stated that this could vary depending on the situation.
Information upon Discharge
The “Information upon discharge” dimension had an average score of 64.0%, with variation across items. Seventy-six percent of patients (Q24) reported that a staff member explained how to use prescribed medications at home in an easily understandable manner, and 74% (Q23) indicated that their family or a close contact received information to support their recovery from doctors or nurses. However, only 49% (Q25) reported being informed about the possible side effects of their medication, and 61% (Q26) reported receiving guidance on warning signs to monitor after returning home. These findings reveal a clear need to strengthen communication regarding post-discharge care.
Confidentiality, Privacy, Consideration of Pain, and Care
The “Confidentiality, privacy, consideration of pain, and care” dimension obtained an overall score of 82.0%, reflecting strong institutional performance. Most patients reported that their privacy was protected during their stay (86%, Q28) and that physicians took measures to prevent others from overhearing sensitive health information (67%, Q27).
Regarding pain management, 78% (Q30) considered that staff did everything possible to relieve their pain. Communication was also rated positively: 87% (Q31) reported that information was provided sensitively, 84% (Q32) felt that sufficient time was devoted to them, and 86% (Q33) stated that they were treated with respect throughout their hospital stay.
Analysis of Dimensions by Place of Care
Table 3 shows that the emergency department had the lowest scores, particularly in “Patient's Rights” (19.9%), “Empathy of informants” (57.2%), and “Information upon discharge” (61.3%). These findings likely reflect the constraints of acute care settings. In contrast, surgical and inpatient units received higher ratings, particularly for “Confidentiality, privacy, consideration of pain, and care” and “How the patient was informed,” indicating more structured communication and greater respect for patients.
Average Score for Each Dimension by Service.

Discussion
The Picker Patient Experience Questionnaire was selected as the assessment instrument for several reasons. This questionnaire is designed to measure patient experience, thereby enabling a direct evaluation of the construct under study. 20 In addition, the instrument allows for international comparisons, as it has been translated and validated into Spanish, facilitating its application across diverse populations.19,20 Furthermore, the self-administered digital format achieved a response rate exceeding the required sample size while minimizing time demands and interviewer bias.
Overall, patient experience in this study was moderately favorable, with an estimated satisfaction rate of 67.6% based on the mean PPE-33 score. The lowest-performing dimension was Patient's Rights (27.9%), while all other dimensions exceeded 63.4%. The highest ratings were for the provision of information to patients and for confidentiality, privacy, consideration of pain, and care, all of which exceeded 82.0%. These findings highlight both strengths and persistent gaps in patient-centered care that may also be present in similar private hospital settings.
In acute care environments, immediate clinical needs often take precedence over formal communication processes. This pattern was evident in the emergency department, which recorded the lowest scores for Patient's Rights, Informant Empathy, and Patient Condition. Such findings reflect the inherent tension between clinical urgency and patient-centered communication, a challenge reported in emergency care settings across diverse healthcare systems.
To promote sustainability, the hospital replaced the physical Patient's Rights document with a digital version, which may partly explain the low scores observed in this dimension. This finding underscores the challenge of balancing operational efficiency with effective communication of patient rights, particularly in high-demand services such as emergency departments. Prior studies have shown that more extended emergency department stays and limited communication are associated with lower patient satisfaction, underscoring the importance of structured information delivery even in time-pressured environments.21,22
Patient experience in emergency departments has garnered increasing attention from patients, healthcare professionals, hospitals, and regulatory bodies. 23 Adequate dissemination of information has consistently been identified as a key determinant of patient satisfaction and perceived quality of care. 24 Evidence suggests that patients who receive clear, timely, and comprehensive information are more likely to report positive experiences, even in acute care contexts. 22 These insights suggest that targeted communication strategies may help mitigate some of the structural limitations inherent to emergency care.
Among sociodemographic factors, occupational status was the only variable associated with patient experience scores at the level of statistical significance. Business owners reported the lowest satisfaction levels, while homemakers reported the highest. This finding contrasts with some prior studies that have identified associations between patient satisfaction and factors such as age, sex, marital status, education, and employment status.11,12 However, growing evidence indicates that sociodemographic characteristics often exert less influence on patient experience than care-related factors, including access, waiting times, communication quality, empathy, and patient involvement in decision-making. 25 These results support the notion that institutional practices and care processes are primary drivers of patient experience across diverse settings.
Physical comfort, particularly pain management, also emerged as an essential component of patient experience. In this study, 78% of patients reported that efforts were made to alleviate their pain, indicating that nearly one-quarter perceived pain control as insufficient. Similar gaps in pain management have been reported in other hospital settings, underscoring the need for systematic approaches to pain assessment and management as integral components of patient-centered care. 26
Taken together, these findings may inform initiatives to improve patient experience not only within the studied hospitals but also in other private healthcare institutions operating in comparable regional or middle-income contexts. While local organizational factors undoubtedly shape patient perceptions, the observed patterns highlight common challenges and opportunities that may be relevant across similar healthcare environments.
Limitations
This study has some limitations. Certain factors influencing patient experience, such as accessibility of hospital infrastructure for family members, as well as clinical variables and disease severity indicators, were not captured, limiting analysis in chronic, oncologic, or palliative populations. In addition, the time elapsed between receipt of care and completion of the survey may have influenced patient responses. Although all participants received care during the same reference period, variability in response timing could introduce recall bias, as prior research suggests that patient experience ratings may differ depending on how soon surveys are completed after care.
Nevertheless, this study provides a valuable contribution given the scarcity of research on patient experience in Costa Rica. The use of the internationally validated PPE-33 and a self-administered digital survey enabled robust measurement, high response rates, and international comparability, reinforcing the validity and feasibility of this methodological approach in the hospital setting. 27
Conclusions
This study indicates that, although overall patient experience in the hospital was moderately positive, areas such as patient rights, empathetic communication, and discharge information warrant further attention. The lower scores observed in the emergency department highlight the ongoing challenge of balancing urgent clinical care with patient-centered approaches. The limited influence of most sociodemographic variables suggests that institutional practices and care processes are the primary drivers of patient experience.
Findings related to pain management and communication of patient rights underscore opportunities to strengthen both clinical processes and information delivery. These areas represent actionable targets for quality improvement initiatives aimed at enhancing patient-centered care.
Notably, the high response rate achieved through a self-administered digital survey demonstrates the feasibility of using online questionnaires for systematic monitoring of patient experience. This approach offers a practical and scalable tool for continuous quality improvement. While the findings reflect the context of two private hospitals in Costa Rica, they may also inform efforts to improve patient experience in similar private hospital settings or in comparable regional and middle-income healthcare contexts. Addressing these aspects through systematic strategies can enhance patient trust, continuity of care, and overall service quality.
Footnotes
Acknowledgements
We would like to thank Cristhian García and Vanessa López from the Patient Experience Department at Hospital Clínica Bíblica for their invaluable insight and support, which made this research possible.
Data Availability Statement
The anonymized datasets generated and analyzed during this study are available from the corresponding author upon reasonable request and subject to approval by the Hospital Clínica Bíblica Ethics Committee.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The paper's authors are employed by Hospital Clínica Bíblica.
Ethical Approval and Informed Consent Statements
This study was approved by the Ethics Committee of Hospital Clínica Bíblica, which operates independently from the research center where the authors are affiliated. Only patients who had previously authorized Hospital Clínica Bíblica to contact them for institutional purposes were invited to participate. In addition, the digital survey included an initial informed consent question, which participants were required to complete before proceeding; only those who consented were able to continue with the questionnaire.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.