
Abstract
Research shows that using a patient's preferred language is vital for effective healthcare communication. Consultations in a second language can lead to treatment delays and misdiagnoses. In Wales, while Welsh and English have equal status in the public sector, independent primary care providers like General Practices (GPs) are not fully bound by Welsh Language Standards (WLS), resulting in inconsistent bilingual provision. This mixed methods study combined focus groups and a survey of 361 Welsh speakers to explore awareness of WLS and experiences of bilingual GP care. Analysis revealed low awareness (27%) of the WLS and significant unmet language needs. 71% had never been offered a Welsh-language consultation and 57% with English-speaking GPs said they would feel more comfortable having Welsh-medium consultations. In high Welsh-speaking areas, 32% felt restricted by not being able to use their first language during GP appointments. There was strong support for recording language preference in health records. Findings highlight both the need and desire for Welsh-language provision in primary care, and the importance of policy changes to support an “active offer” approach.
Keywords
Introduction
Effective communication is vital to quality healthcare, yet the impact of the lack of bilingual provision has not been fully established. Language barriers can compromise patient healthcare 1 especially when consultations occur in a patient's second language. This can lead to misinterpreted information, less treatment compliance, inadequate psychological support, 2 and a lack of informed consent. 3 Language discordance is also linked to delayed treatment, misdiagnosis, longer hospital stays, medication errors, poor management of chronic conditions, increased adverse events, and even death.4–8
Notably, the negative effects of language discordance have been documented in vulnerable groups, including children9–11 and older adults, particularly during dementia. 12 Cultural differences between patients and healthcarers can also lead to less trust and contribute to adverse effects, even if they live in the same country.13,14 Much of this evidence comes from international research on bilingualism and minority languages in healthcare, but research specific to Welsh-medium healthcare is limited.
According to the 2021 Census, 29.1% of Wales’ population speak Welsh. While all Welsh speakers are considered bilingual (able to speak both Welsh and English), many prefer using Welsh, particularly in stressful or vulnerable situations. 15 Importantly, health literacy is often lower in a person's second language, 16 making language choice critical in healthcare. However, as a minority language, Welsh is not consistently available in healthcare settings, placing bilingual patients at a disadvantage. 17 This is particularly concerning for vulnerable groups such as children who haven’t yet learned English, people with dementia who may lose their second language, 12 and individuals with learning disabilities or mental health conditions who communicate more easily in their preferred language. 18 For these groups, limited access to first language healthcare can compromise care delivery. 19 For people in these groups with low health literacy, the lack of bilingual services may further impact their understanding, communication, and health outcomes.
Since 2018, all Health Boards in Wales must comply with and report on their compliance to the Welsh Language Standards (WLS), set by the Welsh Language Commissioner. However, these standards do not apply to independent healthcare providers, such as general practice (GP) surgeries, which are considered independent businesses. 20 As a result, most GPs in Wales are not required to offer bilingual services or comply with WLS, and patients cannot demand Welsh-medium healthcare. This study explores Welsh speakers’ perceptions of Welsh-language use in primary care and assesses the demand/need for more bilingual rights and services in these settings.
Methods
A staged mixed methods approach was used. Stage 1 involved a literature review and focus group exploration of Welsh language experiences in healthcare. Participants were recruited through purposive sampling, they were familiar with the context to help ensure that the questions reflected real experiences and priorities. They were invited by email to join online focus groups (using Zoom) held between 12/2021 and 01/2022. Participants provided written consent prior to taking part. Discussions were recorded and verbatim transcribed. Thematic analysis followed Braun and Clarke's (2006) 21 method, supported by NVivo. Two researchers (AM, ME) independently familiarized themselves with the data, undertook initial coding whereby both researchers independently read, re-read, and coded raw data. Initial codes were discussed and overlapping codes were merged, unclear codes refined, and agreed definitions recorded to create one coding framework which was applied to the remaining transcript. When new codes emerged, they were discussed and agreed and transcripts reread. Codes were grouped into larger themes, discussed using a thematic map. Disagreements were resolved through discussion until a consensus was achieved. Candidate themes and transcripts were reviewed again to ensure no data were missed and all coded data aligned with final agreed themes. Finally, themes were named, and extracts selected. Themes informed the questionnaire design.
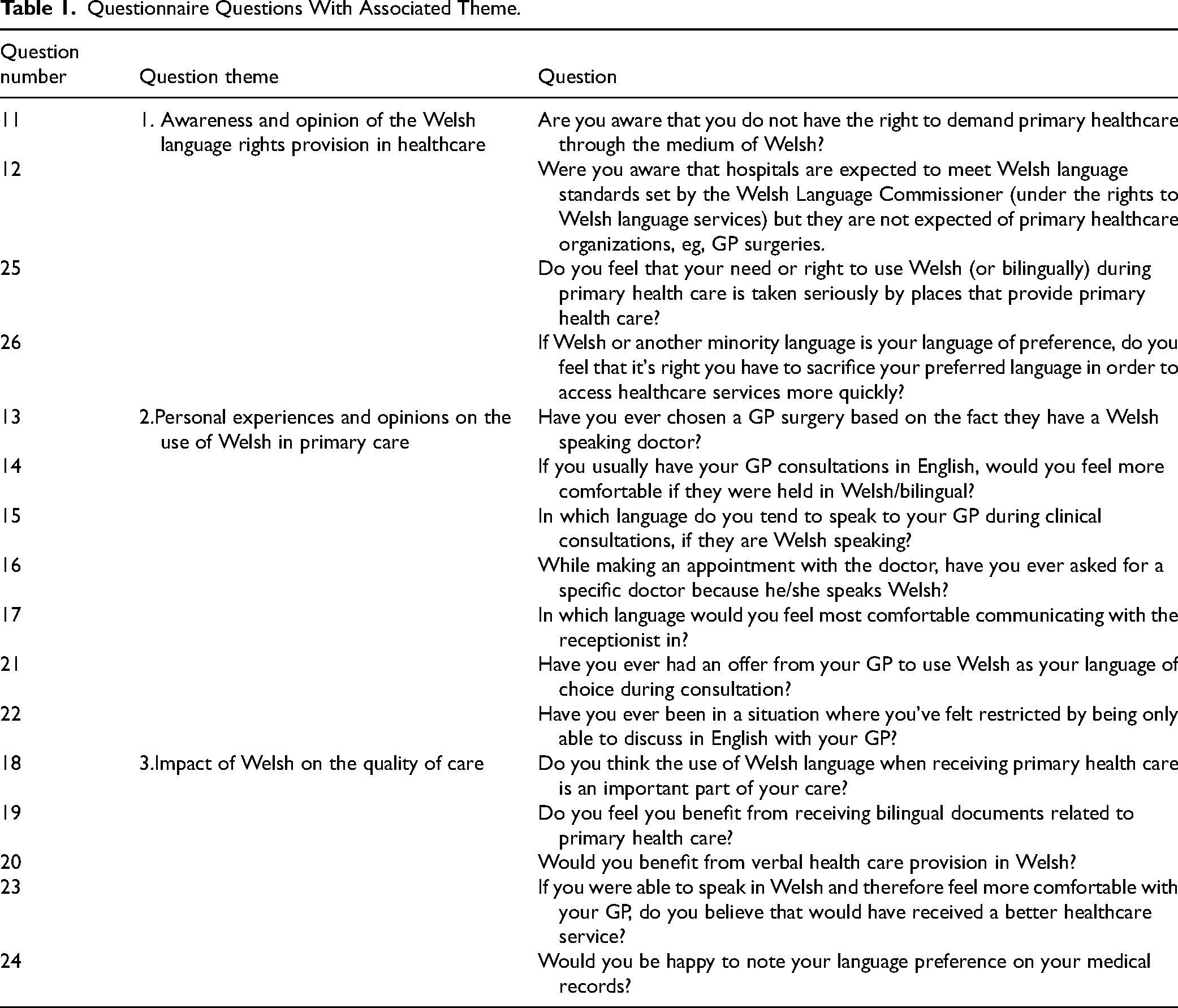
Stage 2 involved distributing an anonymous online questionnaire using Qualtrics XM. The questionnaire was promoted to Welsh speakers at Swansea University, through personal contacts and on social media (Twitter and Instagram). Inclusion criteria included being >18 years old, self-identify as being Welsh-speaking, able to give informed consent and internet access. Participants reviewed the participant information sheet before giving consent and commencing the survey. The 28-item survey covered demographics, language ability/preferences, and explored three themes: (1) Awareness and opinions of Welsh language rights in Healthcare; (2) Experiences of using Welsh in primary care, and (3) Perceived impact of Welsh on care quality (Table 1 and Appendix 1). Questions included a mix of closed answer and free-text responses. Initial analysis suggested regional variation, thus, in addition to data analysis of the whole cohort we also carried out regional subgroup analysis. Respondents were grouped by residence in areas with above or below 35% Welsh-speaking populations (“Higher” Welsh-speaking areas included: Gwynedd, Anglesey, Carmarthenshire, Ceredigion, Denbighshire, and Conwy). 35% was chosen based on data reported by the Office for National Statistics (ONS) (2021) of Welsh speakers in each Welsh county. When displayed as a percentage, the ONS data showed a clear visual separation at this level, with counties having either below 35% or above 35% Welsh speakers, making 35% a reasonable cut-off for sub-categorization. Quantitative data were analyzed using SPSS (version 28) using Chi-square analysis unless stated otherwise with significance being indicated by a 5% change. Free text responses underwent thematic analysis using pragmatic content analysis,22,23 informed by the results from Stages 1 and 2. For some, question frequency analysis was undertaken to identify common themes.
Questionnaire Questions With Associated Theme.
Results
General Themes From the Focus Groups & Dual Interview
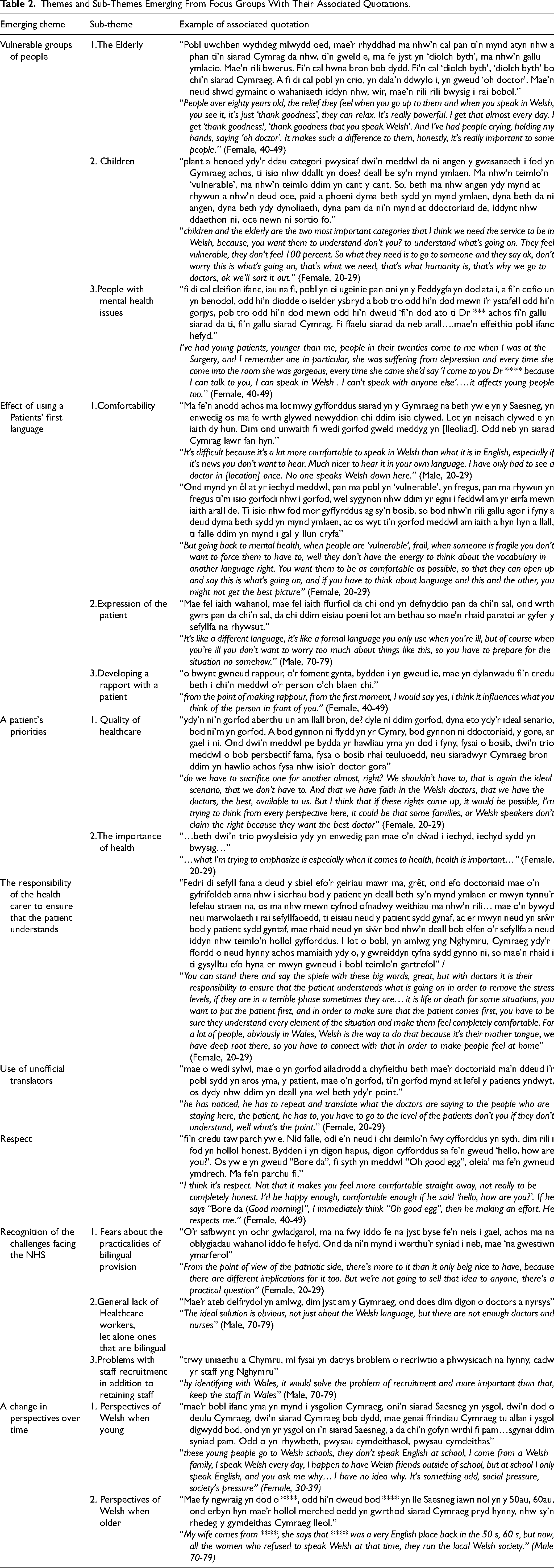
Eligible participants were Welsh-speaking adults aged over 18. The focus group included one male >60, two females aged 25-59, and one male <25. Due to two last-minute withdrawals, a second session was held as an extended dual interview with one male (>60) and one female (25-59) with no opportunity to re-organize additional focus groups due to time constraints of the project. These sessions explored participants’ healthcare experiences to help inform the questionnaire. Transcript analysis identified eight themes: “recognising the challenges facing the NHS,” “identification of vulnerable groups,” “patient's priorities,” “respect,” “responsibility of healthcare staff to ensure patient understanding,” “use of unofficial translators,” “impact of using a patients first language,” and “a change in perspectives over time” (Table 2).
Themes and Sub-Themes Emerging From Focus Groups With Their Associated Quotations.
Questionnaire Results
Summary
Of the 377 submitted questionnaires, 361 were sufficiently complete (>50%) and included in the final dataset. The sample was predominantly female (76%, 272/357) and plurality aged 30-49 (45%) with 26% < 30 and 29% > 50. Respondents represented all 22 Welsh counties, with 44% from areas where over 35% of the population speak Welsh. Most were currently in work (73%), with students comprising a further 16%.
Welsh Language Status of Participants
Although all participants were Welsh speakers, only 53% reported Welsh as their primary home language, with 18% using both Welsh and English. Around a quarter identified English as their main home language. This varied significantly with age (P = .004), with 63% of those >50 spoke Welsh at home, compared to just 38% of those <30.
Most respondents felt comfortable using Welsh: 77% verbally, 60% in writing, and 61% when reading. While comfort with reading and writing did not vary significantly by age, there was a significant association (P = .008) between age and spoken Welsh where 50% of those >50 preferred to express themselves verbally in Welsh.
Respondents from Welsh-speaking regions were more likely (P < .001) to have Welsh as their first language at home in comparison to areas with fewer Welsh speakers (91% vs 56%). A similar result was seen for people expressing themselves in Welsh, with 91% (verbal), 71% (writing), and 75% (reading) either preferring to use Welsh or being comfortable in both languages.
Results Theme 1—Awareness of the Lack of Right to Access to Bilingual Primary Healthcare in Wales
The 2022 Mae gen i hawl (“I have a right”) campaign aimed to raise awareness of the right of the public to Welsh-medium services. However, the WLS only apply to public entities, for example, health boards and not independent entities such as most GP surgeries-only around 9%, are managed by health boards (Welsh government statistics, 2019). Thus, there is likely confusion regarding who have to offer bilingual services. Survey responses confirmed low awareness, only 27% knew hospitals are required to meet WLS, and only 28% knew these rights do not apply to independent primary care providers. Awareness was significantly higher among those over 50, who were twice as likely to know their rights compared to under 30s. Awareness of language rights in hospitals in those >50 was 37%, compared to 19% for people <30s. The equivalent figures for language rights in independent primary care establishments were 36% and 17% respectively. No significant differences were found by region or gender. Overall, respondents felt that their need to use their first language is not taken seriously. Only 18% felt that this was given sufficient priority in primary care. Over half (53%) felt that it was unfair to “sacrifice” their preferred language to access faster care. Those living in Welsh-speaking regions were more likely to feel that their language needs were being taken seriously in primary healthcare (P = .008), relative to those from other regions (27% vs 14%).
Results Theme 2—Personal Experiences and Opinions on Using Welsh in Primary Care
After assessing public awareness of their rights to bilingual provision, we explored their personal experiences of bilingual healthcare. Overall, 44% (156/354) of respondents said they choose to speak Welsh with their GP. This figure increased to 60% (156/264) among those with a Welsh-speaking GP and a further 13% (34/264) choose to communicate bilingually. Use of Welsh varied by age (P = .001), with 82% (70/85) of over-50s choosing Welsh or bilingual communication, compared to 52% (32/62) of under-30s. In Welsh-speaking regions the average figure, across all ages, is even higher at 89% (119/133) and even in non-Welsh-speaking regions over half choose to use Welsh to some extent (54%, 71/131) if the GP could speak Welsh (P < .001). Where patients usually use English with their GP, 57% reported they would be more comfortable conversing in Welsh or using both languages. Even among the under 30s and in non-Welsh-speaking regions these figures were 49% and 42% respectively. While the consultation is the most critical part of engagement with primary care, an overwhelming majority (84%) felt more comfortable using Welsh (including bilingually) with reception staff.
Despite strong demand for the use of the Welsh, 71% (246/346) reported not being offered the option. Given the high numbers who use Welsh this suggests that the option is not always offered even where the GP is Welsh-speaking. However, Welsh provision is significantly more common in Welsh-speaking regions in comparison to non-Welsh-speaking regions (32% vs 14%, P < .001). As a result, 24% (83/345) reported feeling restricted by their inability to communicate in their preferred language, with this figure rising to 32% for respondents from Welsh-speaking areas (vs 18% elsewhere). Free-text responses highlighted these challenges particularly in the contexts of children (47%), older people (37%), mental health (10%), dementia (3%), and maternity care (3%). Language access is taken seriously by many, with 18% (63/354) actively requesting Welsh-speaking GPs and 20% (72/358) choosing a surgery that employ Welsh-speaking GPs. In Welsh-speaking regions, these figures rise to 25% (40/159) and 29% (46/159) respectively. Among those with a strong preference for Welsh during a consultation, 41% (64/156) have chosen a surgery to ensure this is possible.
Results Theme 3—Impact on Quality of Care
The questionnaire then explored the patients’ opinion on the impact of Welsh provision on quality of care. The majority of respondents (67%, 233/346) believed they would benefit from receiving verbal healthcare in Welsh. Older patients felt even more strongly (80%) but even among the under 30s the majority agreed (55%) (P < .001). The effect per region was similar, with 81% in Welsh-speaking regions believing they would benefit. Even in non-Welsh-speaking regions over a half (56%) shared this belief.
While 31% (105/337) felt that speaking Welsh with their GP would enhance treatment, 38% (129/337) disagreed. There was a stronger response to the use of bilingual documents, with 63% (220/350) reporting that this would improve their healthcare, rising to 69% in Welsh-speaking areas (P = .016). Twenty-two comments were left in free text boxes for this question, which revealed several themes. For comments relating to bilingual provision not adding value to their care there were 5 main themes: “no service improvement” (3 comments); “patients equally comfortable using English” (3 comments); “a lack of Welsh-speaking staff” (2 comments); “a restriction in services” (1 comment) and that “there might be a better service but not care” (1 comment). Conversely, 13 themes highlighted benefits of bilingual healthcare, such as, for “groups with increased requirement for the provision” (6 comments), “patient expression” (4 comments); “communication” (5 comments); “comfort” (2 comments); “improving the patient-clinician bond” (2 comments); one comment each regarding “understanding,” “support,” “relief,” “being judged on their English,” “the explanations of the patient being disregarded by English speaking clinicians,” “a reduction in language barrier,” “difficulties using translators” and “improved quality of care.” There was also one comment regarding being unsure of the impact of receiving treatment in Welsh.
It is clear from the responses that the Welsh language provision in primary care is an important issue. Overall, 73% of respondents felt that Welsh language services is an important aspect of their care, with 44% considering it very important. This increased to 89% in Welsh-speaking regions, but this opinion was also shared by a majority from non-Welsh areas (61%).
To facilitate an “active offer” of Welsh provision in primary care (rather than being requested) patients would need to make their preference clear on their medical records. We found almost complete support for this, 86% would be happy for their language preference to be recorded in their medical records, and a further 14% were unconcerned by this. Only one survey respondent was opposed to this.
Thematic Analysis Results of Free Text Responses
Many respondents shared in-depth comments, overall, 298 comments were recorded, suggesting that many felt passionate about this topic. Nine key themes emerged: “Vulnerable groups,” “language choice,” “effect of using a patients first language,” “patients’ priorities,” “the presumption that everyone can and is happy to communicate in English,” “use of Unofficial translators,” “current services,” “challenges facing the NHS,” and “feelings of stigmatisation” (Table 3). Five of these themes overlapped with themes from the focus groups.
Themes and Sub-Themes Emerging From Free Text Boxes in the Questionnaire With Examples of Their Associated Quotations.

Discussion
Effective communication is essential for quality healthcare, yet the impact of limited bilingual provision on first-language Welsh speakers remains underexplored. This mixed-methods study aimed to assess public awareness, experiences, and perceptions of bilingual care in primary healthcare settings.
Awareness of language rights was low, only a third of respondents were aware that WLS apply to hospitals but not most GPs. Given that the WLS were implemented in 2016, this suggests a slow dissemination of public information. Interestingly, awareness of language rights increased with age. Focus group comments (Table 2: A change in personal perspectives over time) suggested that younger generations often face social pressures at school, where English is the dominant social language, but perspectives can shift over time. Personal experiences such as caring for children or older relatives, or developing a stronger sense of identity, could heighten awareness. This is consistent with themes from the questionnaire's free-text comments. Growing awareness may prompt some to engage with regulations and policies which may have previously been overlooked. Overall, the lack of clarity regarding language rights in healthcare highlights the need for a Welsh Government public campaign across all age groups to improve understanding.
Participants from Welsh-speaking regions were more likely to perceive benefits to Welsh-language healthcare and actively choose GPs offering Welsh provision. While 84% preferred speaking Welsh with reception staff, Welsh provision is inconsistently promoted. Free-text comments highlighted feelings of stigmatization, injustice, and frustration (Table 3) with bilingual services resembling a “postcode lottery,” “No one ever offers a Welsh language service. Sometimes it's available but not promoted.” This observation raises concerns that services may exist but go underutilized due to a lack of active offer, promotion, or visibility. The Iaith Gwaith (Working Welsh) logo, launched in 2005 by the Welsh Language Commissioner, identifies Welsh-speaking staff. Its aim is to facilitate the normalization of the “active offer” of Welsh, making its availability visible, reducing stigma and awkwardness when requesting Welsh services. However, the logo's promotion and consistent use in GPs is limited, and it's meaning not widely understood. Greater awareness and consistent use of the Iaith Gwaith logo could empower patients to identify and request services in their preferred language.
Only 18% of respondents felt their need to use Welsh was taken seriously in healthcare settings. Some described relying on unofficial interpreters, for example, bilingual staff, family members or the need for “internal” translation (when switching from first to second language) (Table 3). Although no comments described health carers as translators, this is known to occur. 24 One participant reported being questioned for translating for their child during a consultation, highlighting stigma, discomfort, and cultural insensitivity. Respondents also noted the presumption that English is the default language, despite Welsh-speaker rates of 52% to 76% in North and West Wales (ONS, 2021). The General Medical Council (2013) emphasizes that healthcare providers must communicate in a way patients understand, while translation is helpful, 24 there is a risk of miscommunication, particularly when handling complex medical terms. 25 Research supports the use of trained interpreters, but direct communication in a patient's first language remains safest. One participant also raised child-safety concerns when communication with a health visitor was not possible. Overall, these situations increase stress for both patients and their carers. For Welsh speakers, using their first language can improve communication, enhance comfort, clarity, and relief, particularly in vulnerable situations. This is consistent with international research showing that first-language care can foster trust, alleviate stress, and improve patient–physician relationships.26,27 This can lead to more accurate diagnoses and improved outcomes. 28
About 32% from Welsh-speaking regions reported feeling restricted when unable to communicate in Welsh. This finding is consistent with other Welsh research, a pharmacy study reported 54% of respondents struggled to find English words for symptoms. 28 Research also shows that Welsh speakers describe pain using unique terms and metaphors not captured by English-only tools like the McGill Pain Questionnaire. 29 This highlights the need for culturally and linguistically appropriate assessment tools. Evidence suggests that language concordance may also improve physical health outcomes. For example, Diabetic Latino patients in the United States showed improved glycemic control when switching to Spanish-speaking physicians. 30 Similarly, Welsh-speaking physiotherapy patients had better outcomes with bilingual therapists. 31 These findings highlight that language use in healthcare affects both emotional wellbeing and clinical outcomes.
Respondents expressed dissatisfaction with having to forgo their right to use their preferred language for faster healthcare access. However, they also acknowledged NHS staffing challenges and a shortage of Welsh-speaking professionals. Recruiting and retaining GPs is particularly challenging in rural areas. 32 Research also shows that although the WLS exist, Welsh is often missing from health boards’ well-being objectives, limiting their implementation. 33 The Welsh Government's “More Than Just Words” strategy promotes an “active offer” approach, but more robust infrastructure and training are needed. 34 Respondents supported recording their language preference in medical notes. However, one expressed concern that records must remain accessible to all doctors, regardless of language. There is indeed a need for guidance on safe communication in multilingual contexts. International models, such as those developed for Chinese patients in Australia 35 and Euskara speakers in the Basque Country 36 could inform future frameworks in Wales, as examples of how we might deliver healthcare in a language that is considered a minority in a mainly English or Spanish setting respectively.
Importantly, some bilingual individuals, such as people with dementia, may lose fluency in their second language, 37 highlighting the need for language-sensitive assessments. While many Welsh speakers are fluent in English some may struggle to express themselves fully, particularly during emotionally charged or complex medical consultations.15,29 Participants’ comments revealed themes of frustration, unmet needs and emotional strain, particularly among vulnerable groups. These findings reflect tensions between language rights and service accessibility.
Limitations and Conclusion
This questionnaire targeted Welsh speakers which may have introduced responder bias, as they may be more likely to engage with the topic. Nonetheless, capturing their experiences remains relevant and valuable. We also acknowledge that the questionnaire was not expert-reviewed and some wording could be considered “leading,” for example, “having to sacrifice their preferred language.” However, this reflects perceptions expressed by Welsh speakers, and this language was also used in the focus groups (Table 2: A patient's priorities/1. Quality of healthcare). The Welsh Government also recognizes the risks of inadequate first-language provision. 34 Notably, several respondents expressed passion for the topic, emphasizing its importance and thanking us for conducting the research. Overall, our findings show that while Welsh speakers value bilingual healthcare, many are not offered the use of Welsh. The resulting disparity in service availability affects comfort, communication, and care quality. There is a need to improve awareness, enable active offers, and strengthen rights to support care in a patient's preferred language.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735261417165 - Supplemental material for Patient Experience and Perception of First Language Usage in Healthcare: The Welsh Perspective
Supplemental material, sj-docx-1-jpx-10.1177_23743735261417165 for Patient Experience and Perception of First Language Usage in Healthcare: The Welsh Perspective by Maisie E. Edwards, MSc, Owen Bodger, PhD, Menna Brown, PhD, Llinos Roberts, MD, Luke D. Roberts, PhD, Jeffrey S. Davies, PhD, and Alwena H. Morgan, PhD in Journal of Patient Experience
Footnotes
Consent to Participate
Respondents of the survey gave digital (“written”) consent before starting the survey. Participants of the focus groups gave written consent before starting the focus group. All consent documents are available for review.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
The Swansea University Medical School Research Ethics Review Committee approved our study (Ref:2021-0089) on 18/11/2021.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.