
Abstract
Patient and family advisory councils (PFACs) are a key strategy in advancing patient-centeredness, heralded by the Institute of Medicine as a goal to improve healthcare quality. Although PFACs have been around since the 1980s, they exist in only 54% of US hospitals, according to the American Hospital Association's annual survey of 6100 hospitals. This research aimed to identify key predictors of PFAC effectiveness, since previous studies had lacked descriptions of these factors. Using the C-OAR-SE theory, this quantitative, validated survey of 60 questions was answered by 203 respondents who worked or had worked with PFACs in US hospitals. The results revealed that leadership support was significantly associated with increased meeting content, stronger measurement practices, and more frequent decision-making and involvement with policies and procedures. PFACs, focused on conditions or patient types rather than general PFACs, scored higher on multiple factors, including meeting content, measurement practices, level of engagement, and coaching and training members. This study highlights the key drivers of effective operations and reinforces the value of patient-centeredness in integrating the patient and family voice into hospital initiatives through PFACs.
Introduction
Patient and family advisory councils (PFACs) are rooted in patient-centeredness, spawned, in part, by the Institute of Medicine's (IOM) report, Crossing the Quality Chasm, released in 2001. 1 Citing the gap in quality, the IOM, now known as the National Academy of Medicine, called on the healthcare industry to embrace 6 goals to improve quality, 1 of which was patient-centered care. One strategy for improving patient-centered care is through PFACs, which advise hospitals on a broad range of initiatives to improve care design and delivery. Typically comprised of members who have used the hospital's services within the past few years, PFACs serve as a consumer research group for hospitals. 2 Although the first US PFAC was implemented at Boston Children's Hospital in 1982, 3 according to the American Hospital Association's (AHA) annual survey of approximately 6100 hospitals in 2023, only 54% of responding hospitals, reported having a PFAC, which was down from 55% in 2019 before the pandemic. 4
The literature review was bifurcated into the survey format and questions and a PFAC literature review. 5 These, coupled with the authors’ qualitative study involving 20 hospitals and their PFACs, served as antecedents to developing this quantitative questionnaire. The PFAC literature review analyzed 143 articles, which revealed the prevalence of PFAC characteristics and became the basis for identifying the independent, dependent, and control variables in this study.
The literature review identified 3 major gaps: no research focused on the qualities that contributed to an effective PFAC; the studies lacked quantitative and qualitative metrics to monitor departments’ and members’ feedback about the meetings and gauge the departments’ initiative outcomes, although potential measurement was plausible in several studies; and the description of governance qualities was minimal. The study objectives were to examine PFAC functions and characteristics across US hospitals and analyze the relationships among variables.
A second scoping study on the survey format added a further dimension to confirm and define constructs and survey scales. The aim of the second literature review was to research survey characteristics, plus the advantages and disadvantages of an online convenience questionnaire. Nine terms were searched in a literature review using 5 databases, including CINAHL, Cochrane, Medline, PubMed, and Scopus, which yielded 38 articles for in-depth review.
The literature review supported the use of an online convenience survey to collect large amounts of data efficiently and economically. 6 Plus, online surveys were also easier to deploy and analyze than mail or telephone surveys. Online surveys may appear more anonymous than other types of surveys, which inspired candor in responding to questions. 6 Another advantage was that survey hyperlinks could be easily embedded in emails, facilitating access to the survey instrument. 7
The literature review also acknowledged the limitations of a convenience sampling. These drawbacks included the generalizability of the study and the validity of the results. Self-selection bias was a concern, since individuals who chose to respond may have differed from those who did not. 8 Duplicate responses could have posed risks to data integrity, requiring stringent design and screening procedures. 9 However, this survey design accounted for duplicate responses by requesting respondents indicate their hospital and PFAC names.
This quantitative study aims to understand the drivers of PFAC functions and characteristics of effective PFAC partnerships. One of the primary objectives of this study was to assist hospitals in implementing effective PFACs and enhancing existing ones with empirical evidence that provides guidelines for increasing patient-centeredness by incorporating the patient and family voice into hospitals. To our knowledge, no study has analyzed these specific data about hospital PFACs.
Method
The study examined relationships among variables and predictors captured from 60 questions answered by employees who worked or had worked with PFACs at US hospitals to determine the drivers and barriers.
Survey Theory
The survey instrument was developed using the C-OAR-SE theory, which includes 6 procedural steps to guide the creation of effective and reliable measurement scales (C—construct definition, O—object classification, A—attribute classification, R—rater identification, S—scale formation, and E—enumeration and scoring). 10 This framework ensured that the survey elements were clearly defined—the object, the attribute classification, and how the rater interacted with the measurement tool, which helped to validate the survey. Each survey question had 2 parts: the query and the return. The query can be a statement or a question that provides information about the object being measured and the attribute of interest. The return can be open, prompting raters to use their own words, or close, listing response or answer options for the rater to select. All dimensions in this survey were close. Dolnicar 11 offered recommendations to reduce interpretation variability. Using this framework, each survey question was reviewed for plain language, and short and specific queries. The survey was pretested.
Survey Design
The development of a validated instrument was critical in this quantitative exploratory study to ensure accurate construct measurement. The importance of query clarity was supported by Artino and colleagues, 12 who proposed a systematic, 7-step process for developing effective questionnaires, which included defining constructs, writing clear questions and responses, and ensuring scale reliability. This process facilitated internal consistency and content validity.
These practices guided the development of a survey instrument for the study, which was validated through reviews by 10 subject matter experts (SMEs), pretesting, and the adoption of readability and design standards.4,13 By grounding the PFAC survey in both theoretical and empirical literature, this study enhanced the reliability of its findings and contributed to the growing field of PFAC research.
Survey Validation
The survey validation included 3 phases. In phase 1, a draft survey instrument was created incorporating the framework from the scoping review 5 and the authors’ qualitative study. 14 In phase 2, the survey was submitted to 6 SMEs for face validity, as recommended by Rubio and colleagues. 14 The SMEs included 3 academicians—an expert in survey valuation, 1 in public health research, and another in public health education—plus 3 nonacademic experts who worked with hospital PFACs for at least 10 years, with an average of 18 years. They were asked to review the instrument for validity independently.
The first round of SME reviews yielded 5 recommendation types: add or revise a question, format the instrument, clarify a question or a response, add a response choice, and revise the introduction, which were incorporated. In the second round, the revised instrument was sent to the same SMEs to review again for face validity, plus 4 public health education academicians. In phase 3, 3 SMEs were sent a link to the Qualtrics survey, timed at less than 10 min to complete, to pretest before survey distribution. This pilot did not reveal any issues with the Qualtrics survey. The Institutional Review Board approved the final survey as a modification of the authors’ qualitative study (UNLV-2024-122).
The final survey consisted of 60 questions, including 5 mandatory questions with forced responses and 6 questions with skip logic. The survey was segmented into the following domains: Demographics, Leadership engagement, Recruitment and onboarding, Meetings and engagement, Content and agenda management, Feedback and evaluation, Accomplishments and impact, Budget and resources, and Patient experience scores. The survey captured the hypotheses research questions about leadership support, metrics, meetings, content amount, and patient experience star ratings.
Data Collection
Using a convenience sampling strategy, the survey was conducted in February and March 2025. Inclusion criteria were those participants who were employees of US hospitals and who worked or had worked with PFACs. Participants were excluded if they were PFAC volunteers, since they may not have had direct knowledge of hospital policies, governance, budgets, and performance metrics. The survey was distributed 4 times to databases, industry listservs, LinkedIn groups, and 50 state hospital associations, plus the District of Columbia.
This online survey was created in Qualtrics (Version 2025), which enabled the data to be downloaded as CSV, Excel, and SPSS files. The latter file format allowed the data to be easily uploaded to the SPSS platform (IBM SPSS Statistics, v 29.0.2.0) for analysis.
Hypotheses
The hypotheses were developed from 3 sources: partnership theory, 15 literature review, 5 and the authors’ exploratory qualitative interviews, which preceded this quantitative survey, and which identified drivers for effective PFACs. Parent and Harvey 16 created the partnership model, which defined the relationships among the variables and informed the hypotheses creation. The model constructs include communication, conflict resolution, process, outcome metrics, and so on.
Three directional hypotheses were formulated to explore factors influencing the patient experience and answering the overall research question, “What are the drivers and barriers of an effective PFAC?”
Hypothesis 1: High leadership support for the PFAC positively influences patient experience star rating scores.
Hypothesis 2: Frequent premeetings with departments positively influence the frequency of measurement.
Hypothesis 3: High leadership support for the PFAC positively influences the amount of meeting content.
Results
A total of 330 people responded to the survey; however, 36 did not enter any data, 84 did not work for a US hospital, and 7 were duplicate PFACs, leaving 203 respondents for analyses. Ninety-one respondents listed their hospitals, which allowed the number of beds, financial structure, and locale to be appended from 2023 AHA data. 4 Hospital Consumer Assessment of Healthcare Providers and Systems patient experience scores were appended from Centers for Medicare and Medicaid Services data.
Variables
Table 1 describes the variables used in the regression analysis, with the number of responses (N), the mean, and standard deviation (SD) where applicable. The dependent and independent variables were informed by the authors’ qualitative exploratory study and were further developed through the literature reviews. The control variables were prevalent in the literature review. 5
Regression Variables.

Abbreviation: PFAC, patient and family advisory council.
The Appendix includes descriptive statistics on all the variables. Here is a summary of demographic data: 71.10% of respondents were from hospital systems with more than 1 hospital as opposed to stand-alone hospitals; 76.81% of hospitals were nonprofits, 1.45% for-profits, and 21.74% represented nonfederal government hospitals; 78.30% of hospitals were urban as opposed to rural; and 41.60% of PFACs had been in existence for 5 years or less, 29.70% for 6 to 10 years, and 28.70% for more than 10 years.
Pearson Chi-Square Test for Independence
The Pearson chi-square test examined whether there was a statistically significant association between 2 categorical variables. To measure the strength of this relationship a posthoc test was performed. Nine sets of variables were evaluated using Cramer's V for nominal variables or Somers’ d for 2 sets of ordinal values with independent and dependent variables.
Four sets of variables had a statistically significant relationship. Here is a summary of the statistically significant findings.
As support from executives and champions increases, PFACs are more likely to report having enough content to fill PFAC meeting agendas. PFAC members are more likely to receive regular training if they are also part of other hospital committees. Greater executive support is associated with higher levels of PFAC decision-making involvement. Greater executive support is related to more frequent input on hospital policies and procedures.
Mann–Whitney Test
In examining the cross-tabulated data of 60 questions with 20 data columns, 1 question appeared to exhibit significant differences between the 2 responses—Does the PFAC have a focus (a condition such as cancer or patient such as youth) or is it a general PFAC with no focus, and could this be a predictor of PFAC effectiveness? Using the nonparametric Mann–Whitney test for nominal and ordinal data, 10 questions demonstrated a statistically significant difference between the PFAC with a focus and 1 without a focus, as exhibited in Table 2.
Mann–Whitney Test Results.
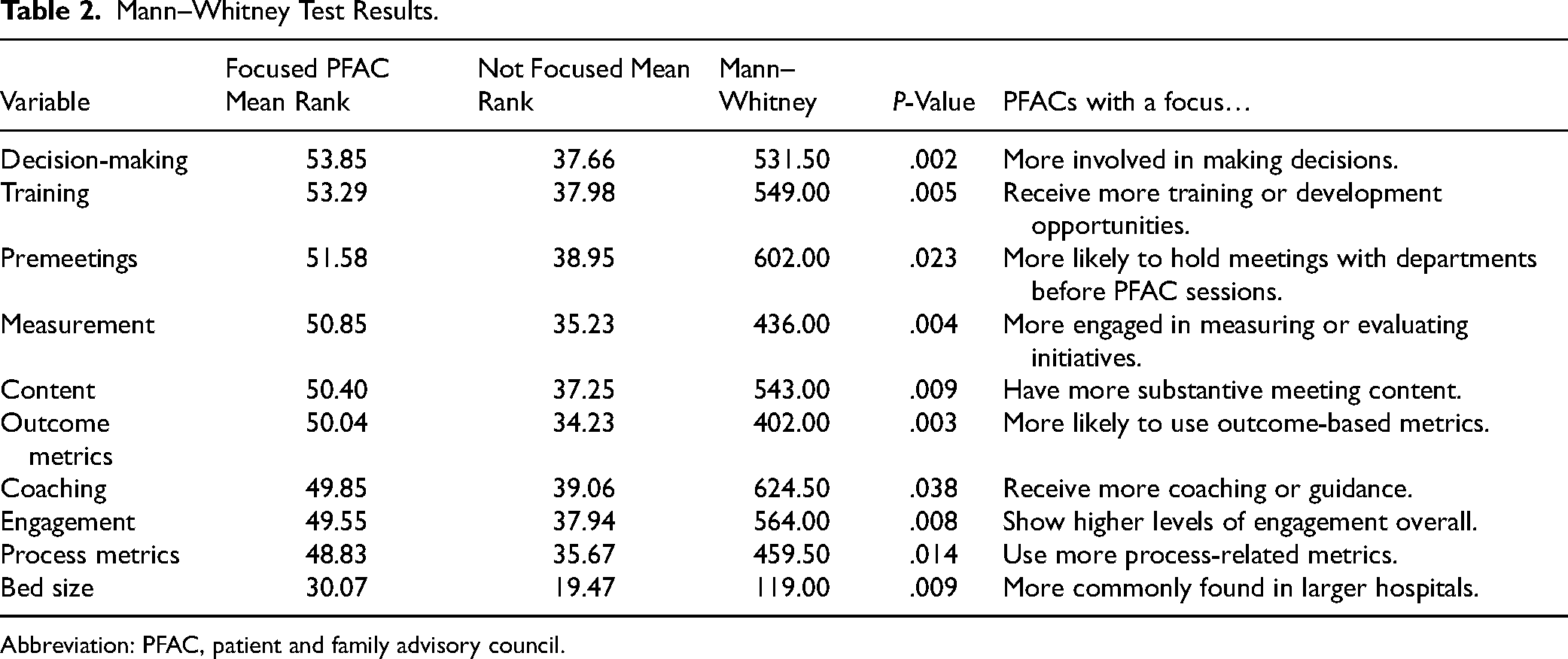
Abbreviation: PFAC, patient and family advisory council.
Regression
Based on themes identified in the literature review 5 and the authors’ prior qualitative study, 3 directional hypotheses were developed to explore potential relationships among key variables (Tables 3 to 5).
Hypothesis 1: High Leadership Support for the PFAC Positively Influences Patient Experience Star Rating Scores.

Abbreviations: PFAC, patient and family advisory council; CI, confidence interval.
Model summary: R = 0.607, R2 = 0.369, Adj. R2 = 0.021, SE = 0.619, F = 1.062, P = .435; N = 30.
There were no statistically significant variables.
Hypothesis 2: Frequent Premeetings With Departments Positively Influence the Frequency of Measuring Initiatives.

Abbreviations: CI, confidence interval; PFAC, patient and family advisory council.
Model summary: R = 0.442, R2 = 0.195, Adj. R2 = −0.022, SE = 0.195, P-value = .889, F = 0.544; N = 46.
Results: As the frequency of premeetings increases, hospitals are moderately more likely to engage in PFAC measurement activities. Adjusted R2 is negative due to the low sample size and the high number of predictors.
Bold indicates statistically significant.
Hypothesis 3: High Leadership Support for the PFAC Positively Influences the Amount of Meeting Content.

Abbreviations: PFAC, patient and family advisory council; CI, confidence interval.
Model summary: R = 0.663, R2 = 0.440, Adj. R2 = 0.269, SE = 0.598, P-value = 0.016, F = 2.574; N = 46.
Results: Both leadership support and PFAC longevity were independently associated with increased meeting content. Councils with strong support from leaders demonstrated significantly greater meeting content, even when accounting for the age of the PFAC. Likewise, PFACs that had been in operation for 11 years or more showed a significant increase in content compared to those 5 years or younger, regardless of support levels. The model explains 27% of the variation in the amount of meeting content.
Bold indicates statistically significant.
Discussion
The study objectives were to examine PFAC functions and characteristics across US hospitals, and analyze the relationships among variables captured in a 60-question survey for people who worked or had worked with PFACs at US hospitals. The findings highlighted important correlations and predictors. One of the most prominent was the association of leadership support, from both the executives and the champions involved with PFACs, and operational practices. Another significant association was the relationship between a focused PFAC, such as cancer or youth, as opposed to a general PFAC with no focus, and variables, such as content amount, feedback, and measurement frequency, as well as training and coaching. Training includes skills development such as how to tell the patient story, for example, and is different from onboarding or orientation for volunteers, which includes issues such as confidentiality, Health Insurance Portability and Accountability Act, and so on.
While leadership support has been touted in the literature,2,17,18 this study examined both executive sponsorship and champion support as moderately correlated variables in the bivariate correlation analysis and then later combined in the principal component factor analysis. The association indicated that when 1 leader exhibited strong support, the other often did as well. The implication was that a patient-centered culture that comes from the top echelons of executive management can influence the champions, who regularly work with PFACs. Existing literature did not discriminate between executives in the C-suite and champions who are closely involved with PFACs.
Leadership support was also statistically significant in 3 key factors of PFAC operations—amount of meeting content, PFAC member decision-making, and input on policies and procedures. One factor was the amount of content brought to the PFAC by hospital departments seeking input on initiatives or programs. The regression indicated that hospitals with higher levels of leadership support were more likely to report having sufficient content to fill PFAC meeting agendas. This correlation revealed that a culture of support for the PFAC motivated departments to bring their patient-facing initiatives to the council for input. In the authors’ qualitative survey, some interviewees mentioned that they did not have enough content for meetings, leaving leaders scrambling to fill the agenda.
The second factor where leadership support was statistically significant in impacting PFAC operations was in decision-making by PFAC members, coupled with input on policies and procedures. This finding was not evident in the literature and has important implications for hospitals in partnering with patients not only to improve patient-centered care and delivery, but also for governance. Creating a culture that is inclusive and empowers patient and family advisors to engage meaningfully in decisions suggests that leadership engagement is not merely a facilitator but may be a critical factor for embedding PFAC contributions into core hospital practices.
One of the most significant findings was that a defined focus (eg, a specific patient type or condition) scored significantly higher than general PFACs on 10 variables, suggesting that hospitals should consider establishing a focused PFAC in a department rather than a general PFAC across the entire hospital. The operational variables included the amount of content; the level of engagement, including the lowest level stamp of approval, feedback, and the highest level of codesign; the frequency of premeetings; the involvement in decision-making; the frequency of initiative measurement; and the use of process and outcome metrics. Other variables in the focused PFACs that scored higher than nonfocused PFACs included the frequency of coaching and training council members. Finally, focused PFACs were likelier in hospitals with 500 or more beds. These results suggest that larger hospitals with focused PFACs are more operationally advanced than general PFACs without focus. The implication is that large hospitals interested in starting a PFAC should consider a focused PFAC. No existing literature delineated between focused and nonfocused PFACs.
Other variables were correlated as well. Chi-square analysis revealed that council members, who served on other hospital committees, were more likely to receive training. This suggests that hospitals interested in partnering with patients and families across the organization are motivated to train the council members to integrate them into committees. If members were trained, they were more likely to receive private coaching about their meeting participation, indicating that certain PFACs invest in training and coaching their members.
Another impactful finding was that PFACs that had premeetings with the departments that planned to obtain input from the council about their initiatives or programs were more likely to engage in measuring those initiatives’ results. Premeetings with presenting departments were a springboard for PFACs to ensure that the meeting content was aligned with their goals and that the partnership with the members was meaningful. As a result, departments were more likely to invest in planning for the premeeting and the council presentation, including questions that would be posted to the members.
Except for hospitals with 500-plus beds, the control variables were not significant. These variables included the rural and urban locale; the financial structure of profit, nonprofit, and nonfederal government hospitals; and the longevity of the PFAC, indicating that new councils can be just as effective as more mature councils.
This study contributes to the evidence-based research about PFACs by highlighting important factors related to their operation and personnel. Leadership support consistently emerged as an impactful variable, suggesting that hospital leaders seeking to start and strengthen PFACs should visibly support partnering with patients and families embedding patient-centeredness into the hospital culture.
Limitations
There were several limitations to this research. The study did not include patient and family volunteers or hospitals worldwide where PFACs have been prevalent, such as Canada. The high number of 60 questions and a 10-min survey duration, as listed, may have discouraged people from responding to the questionnaire. As a convenience survey, there could be sampling bias since respondents participated based on availability, plus self-selection bias. The small sample size in some categories may have decreased the statistical power. Also, the results may have limited generalizability to the broader population of hospital PFACs.
Conclusion
This national study provided new empirical evidence about the operational characteristics and drivers that impact PFACs in US hospitals. Leadership support from executives and champions was a key factor associated with higher involvement of PFAC members in decision-making and in policies and procedures, more frequent measurement practices, and more meeting content. Focused PFACs representing specific conditions and patient types demonstrated more advanced operations across several areas, including coaching and training council members, the amount of meeting content, the level of engagement, premeeting frequency with departments, increased measurement frequency of initiatives, and the use of metrics. While hospital size showed limited significance, other control variables such as locale, financial structure, and PFAC longevity were not significant predictors, suggesting that even small, rural, or newly formed PFACs can be effective with robust leadership support.
Launching a PFAC or strengthening an existing one depends on strong leadership support, coupled with a structure that is embedded into hospital initiatives in a culture that values partnerships with patients and families. For hospitals interested in improving the patient experience, investing in the operational design and providing strong leadership support of PFACs can be a critical strategy in delivering patient-centered care.
Footnotes
Acknowledgments
The authors would like to acknowledge Kavita Batra, PhD, MPH, BDS, FRSPH, Assistant Professor, Medical Research Biostatistician, and Executive Director of Research and Scholarly Activity, Office of Research with the Kirk Kerkorian School of Medicine at the University of Nevada, Las Vegas for her help in validating the survey.
Data Availability
The data is included in the Appendix.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was exempted by the University of Nevada, Las Vegas, Institutional Review Board (UNLV-2024-122) for patient consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.