
Abstract
Professionals in intensive care units (ICUs) should increasingly consider digital innovation in high-quality specialized recovery programs that are easily accessible for ICU survivors and their family members. However, a gap in the literature exists on what is known about the perspectives among the expected users for these digital applications in different healthcare systems. This study explores the differences in perspectives toward digital interventions in post-ICU support among ICU survivors across 4 European countries. A quantitative cross-sectional study was conducted using an investigator developed questionnaire to assess perspectives on digital interventions across Croatia, Germany, the Netherlands, and the United Kingdom. Among 106 ICU participants, the majority was female (63.0%) and aged between 46 and 55 years (36.8%). Three key factors related to digital post-ICU support were identified: perception (ie, perceived effectiveness and relevance of digital health program content), accessibility, and openness to digital health technologies. Interestingly, no significant differences across countries or demographic groups were found. Digital health interventions can provide effective and personalized support to individuals facing similar health challenges across different countries.
Introduction
Adoption of digital health service delivery, including smart phones, social media, and web-based applications, has been growing in recent years, with significant consequences for healthcare users and providers. A transition to digital healthcare might offer several benefits such as better access to reliable health information, offering a more personalized approach, and limiting inefficiencies and costs. 1 From this viewpoint, professionals in intensive care units (ICUs) should increasingly consider digital innovation in high-quality specialized recovery programs that are easily accessible for ICU survivors and their family members.
Surviving a critical illness, and being hospitalized in an ICU has a significant impact on short- and long-term quality of life. Besides physical and cognitive impairments related to their illness, up to 50% of survivors encounter psychological challenges with symptoms of anxiety, posttraumatic stress, and depression.2–4 Emotional processing of a life-threatening event, coupled with frightening memories or delirious experiences, is challenging. Return to work and societal participation may take years with profound economic consequences and burdens for family members and the whole society. Although several approaches in post-ICU care have been developed, digital interventions could improve further patient reported outcomes. 5 Digital post-ICU care could also raise efficacy and attendance rates of outpatient clinics, treatment adherence, and health outcomes by enabling patients to self-engage meaningfully with their care processes.6,7
Fatehi et al established a widely accepted definition of “digital health,” describing it as the strategic application of technology to enhance the health and well-being of individuals and populations, as well as to improve patient care through the intelligent processing of clinical and genetic information. 8 However, the spread, accessibility, and use of digital health applications differ across European countries. 9 Several national healthcare systems strive both to accelerate and to regulate the pace of innovation and commercialization of digital interventions to support individual health and potentially improve the prevention or treatment of illness. 10 An important pillar is the degree to which the information is presented to individual users. For example, an ICU nurse running an inpatient post-ICU clinic might benefit from a digital tool integrated with the electronic health record and tailored to individual patient characteristics, whereas ICU survivors tend to prefer certified websites and applications for health information and improving wellness related to their specific conditions. However, most end-user interfaces have been found underdeveloped. 10 Moreover, there is a notable gap in the literature concerning the perspectives of expected users of digital applications across different European healthcare systems and particularly in the domain of post-ICU care. 11 In the current study, we focus on the perspectives of ICU survivors regarding the types of digital health applications that suits them best.
Aim and Research Question
The aim of this study is to explore differences in perspectives related to digital interventions for post-ICU support among ICU survivors across 4 European countries. The research questions are: (1) “Are perspectives on digital post-ICU support among ICU survivors different across European countries (ie, Croatia, Germany, the Netherlands, and the United Kingdom)? and (2) “Which factors shape ICU survivors’ perspectives on digital post-ICU care interventions?”
Method and Materials
A quantitative cross-sectional design was used as part of a broader research program in the development of digital post-ICU support for survivors and family members. 12 The current study employed an investigator-developed questionnaire to assess perspectives on digital interventions across Croatia, Germany, the Netherlands, and the United Kingdom. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines were used to report this study. 13
Setting and Participants
The study was undertaken in 4 European countries: Croatia (HR), Germany (DE), the Netherlands (NL), and the United Kingdom (UK). Adult ICU survivors were approached from the ICUs of 2 hospitals (HR and NL) and 2 patient self-help groups running peer support with volunteers: Sepsis-Help (DE) and ICUsteps (UK). Convenience samples were used in all settings without predetermined selection criteria based on age, gender, education level, or cultural background to ensure diversity in the study group, data collection, and analysis.
Eligible participants were ICU survivors who had undergone mechanical ventilation for more than 48 h, were aged 18 years or older, and had sufficient proficiency in the respective local language to discuss, read, and interpret the study information and questionnaires. They were also required to be in a stable physical, mental, and cognitive state. This criterion was based on the participant's own assessment of whether they felt ready to participate, recall, and discuss their ICU experience. ICU survivors with pre-existing psychological or cognitive impairments were excluded from the study.
Study Procedures
Eligible ICU survivors were invited to participate by the local study coordinators (AF, CJ, MvM, PN) by sending a blast email. Interested individuals received a written patient information brochure with details on the study aims and procedures. After return of a signed informed consent statement, participants received an email with a link to the online questionnaire or a paper version on request. The questionnaire was designed to be completed in 15 min and was made available on a single web page using the SurveyMonkey© platform. Possibility to review and change the answers by the participants was enabled through a “back button” until finalizing the questionnaire. Log files, IP-address, cookies, view rates, and time of completing the questionnaire were not archived.
Measuring Instrument
The questionnaire was developed by members of the research team, who initially drafted items related to post-ICU support and the use of digital applications in healthcare. These items underwent multiple revisions for accuracy, grammaticality, and cultural relevance. A pilot test with patient experts evaluated the clarity and structure of the questionnaire, leading to further refinements and the addition of items sensitive to cultural differences. This was mostly done across NL, 14 before being translated into English with help of a native speaker. Thereafter, professional language services from DE and HR provided translations, adapting the questionnaire to ensure clarity and accessibility in their respective languages. This multistep translation process was undertaken to accommodate the diverse linguistic backgrounds of the study participants, aiming to foster a more inclusive and comprehensive understanding of their perceptions and needs.
The questionnaire itself consisted of 4 main parts with a total of 35 items all of which are presented in Supplemental File 1. The first part gathered demographic data such as age, gender, educational level, country of birth, and country of hospitalization, which helped contextualize the subsequent responses within specific participant backgrounds. The second part addressed experiences related to ICU admissions, with various response formats including dichotomous (Yes/No) and multiple-choice options. The third part explored digital access and means regarding health information, while the fourth part delved into perspectives regarding a digital post-ICU program. These parts used a Likert-type scale for responses, ranging from “Strongly agree” to “Strongly disagree.” In particular, items such as “I would use a digital health program because it helps me with lifestyle interventions (eg, being active, a healthy diet, quitting smoking)” (Item 20) and “I would use a digital health program, which could help me manage emotional distress and stress” (Item 21), were designed to gauge participants’ perspectives and expectations regarding the use of digital applications in their lives.
Statistical Analysis
Participants who completed less than 90% of the items were deleted from the data analysis for which the Statistical Package for the Social Sciences (SPSS) version 28.0 (Chicago, IL, USA) was used. Data were checked for normality with kurtosis and skewness between −2 and 2 considered as near normal. 15 The 5-point Likert answer categories were recoded, when appropriate, so that the lowest score was 1 and the highest score was 5. This coding was maintained consistently to ensure that lower scores indicated stronger agreement with the statements.
To ensure the reliability of the questionnaire items, internal consistency was measured using Cronbach's alpha (α), with a threshold of 0.7 to ensure an acceptable level of reliability. Principal component analysis (PCA) was employed to explore how different items grouped together, indicating underlying components and factors. Eigenvectors and eigenvalues were derived from the covariance matrix to determine the principal components, which should reduce the dimensionality of the original dataset while preserving significant patterns. The principal components were selected based on an eigenvalue cut-off of 1.0, following Kaiser's criterion, which suggests retaining components that account for more variance than accounted for by one of the original variables. 15 A varimax rotation was applied to clarify which variables grouped together under each component, enhancing the interpretability of the data. Components above 0.500 in the rotated component matrix were considered significant and named based on the most prominent theme emerging from the items. Separate Kruskal–Wallis tests were conducted for each identified component to determine if there were statistically significant variations in perceptions and needs based on the country of origin.
Sample characteristics, including means, proportions, or range as appropriate, and histograms were used to analyze demographic variables (ie, age, gender, educational level, and country of origin). Fisher's exact test was employed to identify any significant differences in these demographic variables across groups. This test was selected due to the presence of cells with expected counts less than 5, a condition that violates chi-square test assumptions. 15 All statistical tests were bilateral with a significance level set to P < .05.
Ethical Considerations
Ethical approval for this study has been granted by the Erasmus MC's Medical Ethical Review Committee, which determined that the research poses no risk to participants (MEC-2022-0153). Thereafter, Institutional Review Boards of the 3 participating countries have waived dispensation from statutory obligation to provide insurance for subjects participating in medical research. Participation in the study required obtaining consent from participants before completing the questionnaire. Participation was voluntary and confidential, with no incentives provided. Participants were assured that their identities would remain anonymous and that they could withdraw from the study at any time.
Results
Demographic Characteristics
In total, 106 participants completed the questionnaire. The majority were female (63.0%) and aged between 46 and 55 years (36.8%). This trend was consistent with no statistically significant differences across countries (Table 1). NL had the highest percentage of participants with a bachelor's degree (46.3%), while UK showed highest percentage with a master's degree (30.8%).
Demographic Characteristics of Participants by Country.

Abbreviations: DE, Germany; HR, Croatia NL, the Netherlands; UK, United Kingdom; n, number.
A sensitivity analysis was conducted to assess the impact of including or excluding Croatian data due to the low number of participants. The frequency distributions showed overall consistency.
Reliability and Components of the Measuring Instrument
Overall, good internal consistency was found across all items of the measuring instrument (α = 0.79), although there was variation between countries. For DE, the internal consistency showed the lowest reliability (α = 0.570, improving slightly to 0.662 with standardized items), followed by HR with moderate internal consistency (α = 0.695, which increased to 0.754 for standardized items). UK showed strong internal consistency (α = 0.837 and 0.825 for standardized items), while NL demonstrated excellent reliability (α = 0.853, and slightly less at 0.846 for standardized items).
Following the PCA, the rotated component matrix showed 3 major components, reflecting factors that significantly influenced the perspectives of participants related to digital post-ICU support (Figure 1).
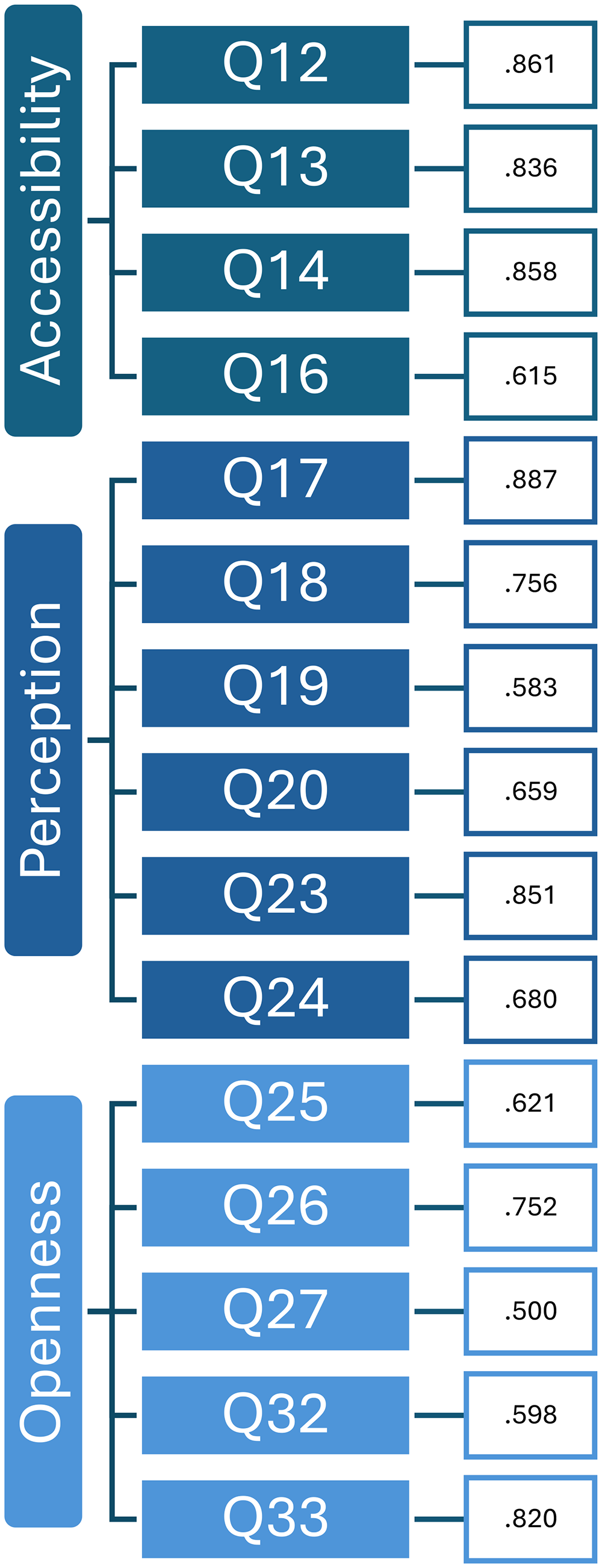
Visual representations of principal component analysis (PCA).
The first factor, “Perception” referred to the perceived effectiveness and relevance of digital health program content. This factor showed variation among participants regarding the expected effectiveness and relevance of digital health programs, thus, indicating different views across countries on how these programs could meet their needs. The second factor is “Accessibility” of digital health, which assessed participants’ access to and ability to use digital health tools. This component reflected moderate variation in participants’ access, thus, highlighting disparities in digital literacy and resource availability. The third factor was “Openness” to digital health interventions, which indicated diverse attitudes toward adopting digital health technologies, suggesting a mix of enthusiasm and resistance among the study participants. The Kruskal–Wallis test results showed no significant effects of demographic variables (age, gender, and educational level) on the factors identified in the PCA (perception, accessibility, and openness). More details on the PCA are available in Supplemental File 2). Descriptive statistics for each factor across the 4 countries varied, with highest means in NL (Table 2).
Descriptive Statistics for Relevant Factors in Digital Post-ICU Care by Country.

Abbreviation: ICU, intensive care unit.
Differences and Similarities Across Countries
Boxplots illustrate the differences and similarities in perceptions, accessibility, and openness toward digital health tools among the surveyed countries (Figure 2). Regarding perceptions of digital health interventions, some variation was observed, particularly in NL, which had the highest number of responses. However, the similarity in median values suggests relatively consistent perceptions among participants across countries. Once again, NL showed a broader range of accessibility scores, with several higher-than-average values, indicating both accessible digital infrastructure and sufficient digital literacy among participants. HR, which had fewer responses, displayed the narrowest distribution of scores. Overall, willingness to use digital programs appeared to be similar across countries. Given the unequal group sizes and the non-normal distribution of the data, the Kruskal–Wallis test was chosen for the analysis of differences among countries. The perceived usefulness of digital health interventions/digital support (perception) did not significantly differ between countries (χ2(3, N = 106) = 3.629, P = .304). Similarly, the ability to access and engage with digital health tools (accessibility) (χ2(3, N = 106) = 6.105, P = .107) and the willingness to adopt digital health technologies (openness) (χ2(3, N = 106) = 2.228, P = .526) were relatively uniform across countries.

Boxplots summarizing perception, accessibility, and openness.
Perspectives on Digital post-ICU Support
Due to unequal numbers of participants across countries, item responses were analyzed for the entire sample. The majority of participants felt satisfied with the treatment they received during their ICU stay (47.2% strongly agreed, 32.1% agreed). While 81.1% felt a need to contact a healthcare professional for support or treatment of symptoms after ICU discharge, 27.4% received a rehabilitation plan and half of them reported difficulty in reaching appropriate professional support (51.0%). Participants consistently viewed digital health interventions positively—for example for providing an overview of relevant professionals for follow-up services (90.6% agreed or strongly agreed), offering videos with information on symptoms (87.7 agreed or strongly agreed), and supporting health monitoring and personalized care (85.8% agreed or strongly agreed). Table 3 provides a summary on participants’ perspectives regarding digital post-ICU support.
Item Responses on Digital Post-ICU Support.

Abbreviation: ICU, intensive care unit.
Digital access and means regarding health information.
Perspectives regarding a digital post-ICU program.
Discussion
This study explored differences in perspectives related to digital interventions for post-ICU support among ICU survivors across 4 European countries. Three key factors were identified as central to the ICU survivors’ perspectives: perception, accessibility, and openness to digital health technologies. No significant differences in these aspects between HR, DE, NL, and the UK were found, thus, showing comparable perspectives across countries. A general willingness to adopt digital health technologies and the ability to access and engage with digital health tools were found among ICU survivors.
The observed similarity in perceptions may be attributed to the universal challenges experienced by ICU survivors, including psychological distress, cognitive impairments, and the need for long-term support, which transcend cultural and healthcare system differences.3,5,16 At the same time, it may also reflect a broader global trend toward the acceptance of digital health technologies, reinforced by their successful implementation in diverse healthcare contexts. Digital tools, such as mobile applications, can help address gaps in traditional care by offering accessible information on treatment and recovery.17,18 The globalization of healthcare and the broad availability of digital technologies may contribute to converging expectations among ICU survivors across countries. 19 With a widespread access to smartphones and the internet, digital health interventions can be delivered across borders, helping to standardize support and reduce variability in perceived needs. Approaches using virtual reality and mobile applications may further enhance understanding of the ICU experience and support mental health recovery.20,21
Country-Specific and Cultural Differences
The landscape of digital health implementation across different countries emphasizes the importance of tailoring digital health interventions to fit the unique healthcare infrastructures of each country. In HR, the Croatian Health Insurance Institute and the Ministry of Health have implemented projects to build an integrated e-Health system. 22 However, issues such as incompatibility of digital solutions and lack of connection between different healthcare institutions may hinder the progress. The approach in DE includes the “Digital Supply Act,” which allows digital health applications to be prescribed and covered through by statutory health insurance. 23 This policy has made it easier to access digital health solutions, thus, stimulating their adoption across the healthcare system. In NL, many efforts promote the implementation of digital technologies in healthcare organizations. 24 These initiatives have been well-received, with healthcare professionals and patients supporting the use of digital technologies to improve accessibility and self-management. The National Health Service (NHS) in the UK has been committed to a digital future through initiatives such as “NHS Digital” and the “NHS Long Term Plan.” 19 These efforts aim to transform healthcare delivery by integrating digital solutions, and help with the system's increasing complexity and demand. Despite challenges such as resource limitations and digital literacy issues, the NHS has made big steps in adopting digital health technologies. Overall, however, digital interventions targeting post-ICU care remain limited and new developments are still in their infancy. 11
Our findings indicate relatively consistent perceptions across countries; however, cultural values may still influence openness to digital post-ICU tools. For instance, UK and DE seemed to lag in openness. Stigma surrounding mental health persists in many societies and may discourage survivors from engaging with digital interventions that explicitly address psychological recovery. 25 Similarly, in healthcare systems characterized by higher power distance, as described by Hofstede's cultural dimensions, patients may defer to medical authority and be less inclined to use self-directed digital resources. 26 By contrast, in lower power distance or more individualistic contexts, survivors may show greater willingness to adopt autonomous digital support. Beyond these cultural aspects, differences in digital trust and literacy further shape engagement. The eHealth literacy framework27,28 emphasizes not only functional and critical skills but also contextual and cultural determinants of how patients access, evaluate, and act upon digital health information. Consequently, while digital tools hold promise for improving recovery after ICU, future cross-cultural studies should examine how factors such as stigma, trust, and hierarchical norms interact with survivors’ adoption and sustained use of these technologies.
Although the study included participants from various countries, cultural sensitivity and the need for customization in digital health tools were not fully explored. Cultural factors might influence how ICU stays are perceived. 29 For example, communication styles can affect how patients and family members interact with healthcare providers, impacting their psychological and emotional experience.30,31 In some cultures, patients may be less forthcoming about negative emotions like fear or anxiety due to cultural norms that discourage discussing mental health openly. 30 This may lead to underreporting of psychological distress and unmet needs for support. To maximize the effectiveness and acceptance of digital health interventions, it is essential to develop culturally adapted and personalized approaches for post-ICU care targeting both ICU survivors and their relatives. By considering cultural differences, including country-specific characteristics, future research can ensure that digital health interventions are both effective and culturally sensitive, improving patient outcomes.
Strengths and Limitations
One of the strengths of this study is the cross-country comparison. By including participants from HR, DE, NL, and UK, this study captures geographic diversity reflecting ICU survivors’ perspectives across different healthcare settings. Another strength is the PCA technique, which enhances the robustness and validity of the findings, ensuring that the key components are meaningful constructs. Using PCA simplified complex data by identifying underlying factors that identified the perspectives of ICU survivors for developing digital health interventions. Several limitations of the study should be noted. First, the study's sample size was relatively small and unevenly distributed across the 4 countries, with a notably larger number of participants from the NL compared to HR, DE, and UK. We acknowledge that this imbalanced distribution may affect the comparability and robustness of the results. Future studies should aim for a larger and more balanced sample size across countries to ensure more reliable and representative results. Increasing the overall sample size would also enhance the statistical power of the study. Another limitation in sample balance is the perspectives from only 4 European countries. Future research should expand with a more global inclusion, for example, southern Europe, to explore differences in digital infrastructure or cultural contexts. Second, the measurement instrument was developed and tested in NL. Although professional translators were consulted for the forward translations and native researchers (AF, CJ, PN) performed back-checks, cross-cultural reliability was not formally tested in the other countries. This may have elicited culturally sensitive challenges impacting the participants’ perspectives, as subtle linguistic or cultural differences may have influenced how respondents interpreted the Likert-scale items. Future validation studies could include cognitive interviewing and pilot testing to reduce the risk of linguistic or conceptual drift during translation. This issue has been noted as a limitation of the study. Third, the recruitment strategy may have introduced bias. ICU survivors were recruited from 2 hospitals and 2 patient self-help groups, which may have skewed the sample toward individuals who are more proactive in seeking support and engaged in their recovery. As a result, the findings may not reflect the broader population of ICU survivors, potentially leading to an overestimation of the positive effects of post-ICU support. Future research should include a more diverse sample by recruiting participants through broader national networks and community outreach to better represent the general ICU survivor population. Furthermore, the participants may have been particularly interested in digital techniques, which could have resulted in a more positive bias in their responses regarding the use of digital health programs. The recruitment process did not implement strategies to control for participants’ predisposition toward positive views or openness to digital interventions. Despite these limitations, this study offers fundamental insights into ICU survivors’ perspectives, which can inform the development of future digital post-ICU support interventions.
Conclusion
Digital health interventions can provide effective and personalized support to individuals facing similar health challenges across different countries. From the perspectives of ICU survivors regarding digital post-ICU, 3 key factors emerged as central to post-ICU support: perception, accessibility, and openness to digital health technologies. These aspects between HR, DE, NL, and the UK were found comparable across countries. By understanding and integrating the local nuances, future research should examine how digital health interventions function in different healthcare systems to develop more effective post-ICU care strategies.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251414753 - Supplemental material for Digital Postintensive Care Support: A Comparative Survey Study Among Survivors Across Four European Countries
Supplemental material, sj-docx-1-jpx-10.1177_23743735251414753 for Digital Postintensive Care Support: A Comparative Survey Study Among Survivors Across Four European Countries by Esra van Olst, Anna Zacharelou, Friganovic Adriano, Christina Jones, Peter Nydahl and MMC van Mol in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251414753 - Supplemental material for Digital Postintensive Care Support: A Comparative Survey Study Among Survivors Across Four European Countries
Supplemental material, sj-docx-2-jpx-10.1177_23743735251414753 for Digital Postintensive Care Support: A Comparative Survey Study Among Survivors Across Four European Countries by Esra van Olst, Anna Zacharelou, Friganovic Adriano, Christina Jones, Peter Nydahl and MMC van Mol in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735251414753 - Supplemental material for Digital Postintensive Care Support: A Comparative Survey Study Among Survivors Across Four European Countries
Supplemental material, sj-docx-3-jpx-10.1177_23743735251414753 for Digital Postintensive Care Support: A Comparative Survey Study Among Survivors Across Four European Countries by Esra van Olst, Anna Zacharelou, Friganovic Adriano, Christina Jones, Peter Nydahl and MMC van Mol in Journal of Patient Experience
Footnotes
Abbreviations
Acknowledgments
We thank all participants for dedicating their time contributing to the study, thus; sharing their experiences on being critically ill and providing their valuable expectations on digital delivery of follow-up services. We also thank Foundation Family and patient Centered Intensive Care for their support in providing the software to conduct the study.
Author Contributions
Conceptualization: Adriano Friganovic, Christina Jones, Peter Nydahl, and Margo van Mol; methodology: Esra van Olst and Margo van Mol; software: Foundation FCIC; validation: Adriano Friganovic, Christina Jones, and Peter Nydahl; formal analysis: Esra van Olst and Margo van Mol; investigation: Christina Jones, Peter Nydahl, and Anna Zacharelou; resources: Adriano Friganovic, Christina Jones, Peter Nydahl, and Margo van Mol; data curation: Esra van Olst and Margo van Mol; writing—original draft preparation: Esra van Olst and Margo van Mol; writing—review and editing: Adriano Friganovic, Christina Jones, Peter Nydahl, and Anna Zacharelou; visualization: Margo van Mol; supervision: Margo van Mol; project administration: Anna Zacharelou; funding acquisition: Margo van Mol.
All authors have read and agreed to the published version of the manuscript.
Ethical Considerations
This study was conducted according to the principles of the Declaration of Helsinki and in accordance with the Dutch Medical Research Involving Human Subjects Act. The Medical Research Ethics Committee of Erasmus Medical Center (MEC-2022-0153) granted approval for the study. Thereafter, Institutional Review Boards in the 3 participating countries waived from the requirement to provide insurance for subjects participating in medical research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the European Society of Intensive Care Medicine (ESICM, no grant number; Multidisciplinary Care Award 2022). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Informed Consent
The authors affirm that informed consent was obtained from all subjects involved in the study. All agreed to use their data and publish anonymized group-level results. No material from other sources has been used.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized data gathered and analyzed during the study will not be available publicly due to legal and ethical restrictions. These will be freely available at a reasonable request to any scientist wishing to use them for noncommercial purposes as well as text and photo material of the developed intervention. The results of the study will be disseminated to healthcare professionals, health services authorities, and the public via presentations at national and international meetings and published in peer-reviewed journals.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.