
Abstract
The study aimed to assess the effect of chronic diseases on health-related quality of life (HRQoL) among university students. A cross-sectional analytic study was conducted at King Abdulaziz University, involving 1173 students. Questionnaire on chronic diseases, HRQoL using the 36-item Short Form Health Survey (SF-36), alongside other factors was distributed electronically. Regression analysis was used to identify factors associated with HRQoL. The mean ± SD scores across SF-36 dimensions varied, with physical functioning scoring the highest (74.81 ± 27.82) and energy/fatigue the lowest (38.52 ± 24.03). The physical and mental component summary scores were 68.07 ± 18.67 and 49.20 ± 23.17, respectively. The study found a 23.1% prevalence of multimorbidity. Multimorbidity was associated with significantly lower HRQoL across all dimensions. Female sex, low family income, and lack of exercise were predictors of poor HRQoL. High-impact diseases were strongly associated with poorer physical health. The study revealed significant burden of multimorbidity that demands targeted interventions. Focus on modifiable risk factors, such as exercise and socioeconomic support, could enhance overall well-being and prevent negative health outcomes.
Introduction
Population aging is one of the humanity's greatest achievements, yet it presents complex challenges that require a multifaceted approach, including promoting healthy lifestyles early in life, adapting healthcare systems, and fostering social inclusion. 1 Multimorbidity, which is the co-occurrence of 2 or more chronic conditions in the same individual, is one of the challenges threatening aging societies.2,3 It is characterized by the accumulation of chronic comorbidities over the lifespan and adverse health trajectories, necessitating urgent preventive measures.4,5 International studies indicate a global prevalence of multimorbidity estimated at 37.2%, with significant regional variations, both in prevalence rates and morbidity patterns, as well as consistently increased risk with the individual's age.6,7
Multimorbidity significantly affects overall quality of life (QoL) and health-related quality of life (HRQoL). A systematic review and meta-analysis revealed a linear decrease of approximately 1.6% to 4.4% in HRQoL scores for each additional comorbidity, depending on the HRQoL scale used, impacting physical and mental health components. 8 Multimorbidity also induces a significant burden on the economy and healthcare systems, which is expected to rise with the aging population. The annual cost for a multimorbid person varies significantly, with estimates from high-income countries ranging from I$800 to I$150 000 per person associated with increased utilization across various healthcare services.9,10 Although multimorbidity and its impact of the HRQOL have been extensively researched in the elderly and institutional populations, it remains inadequately explored in youth. Nonetheless, available data indicate significant rates of multimorbidity among children and youth, highlighting certain typical, physical and mental comorbid associations. 11 This is associated with severe impacts on HRQoL. Moreover, the accumulation of both physical and mental disorders leads to an even more profound effect, demonstrating a dose–response relationship and a worsening trajectory with advancing age. 12 This impact extends to several life domains including school environment and academic achievement. 13
In a preventive approach, studying multimorbidity among youth and its impact on HRQoL holds greater relevance in modern societies than focusing on adults or the elderly. Such research provides critical insights for shaping policies and long-term strategies to improve health trajectories earlier in life, mitigating the lifelong burden and cascading effects of multimorbidity on health, well-being, the economy, and healthcare systems. 14 Through the Quality-of-Life Program, the Kingdom of Saudi Arabia aims to enhance the well-being of residents and visitors by fostering a dynamic environment. 15 For the young population, measuring HRQoL is crucial for monitoring and improvement, especially among university students who are at higher risk of HRQoL deterioration due to academic stress, insomnia, and burnout. Students with multimorbidity face greater risks to their HRQoL, potentially leading to inequalities in healthcare, health outcomes, academic performance, and overall well-being. However, regional data on the specific impact of multimorbidity in this group is lacking. 16
Focusing on university students in Jeddah is contextually important. Jeddah hosts a large and sociodemographically diverse student population drawn from different regions of Saudi Arabia, providing a pragmatic window into Saudi youth. University settings are also where health promotion, mental-health support, and preventive services can be delivered at scale through campus programs; therefore, quantifying multimorbidity and its association with HRQoL in this population has immediate relevance for student health services and aligns with national priorities for early prevention and well-being. Additionally, the high digital literacy and centralized campus communication channels facilitate robust sampling and high-quality data collection, enhancing feasibility while supporting reproducibility and future surveillance.
This study fills this gap by estimating the prevalence and impact of multimorbidity on HRQoL among students at a university in Jeddah, Saudi Arabia. It also analyzes the factors associated with students’ HRQoL.
Methods
A cross-sectional analytic study was conducted between June 26, 2022 and December 25, 2022.
The study targeted all students enrolled at the university. Sample size was determined using OpenEpi, open-access software for epidemiologic statistics using 95% confidence level and an expected prevalence of 0.50. The calculation yielded an initial required sample of n = 1092, calculated for 4 specialty categories, we applied a 10% inflation to account for potential nonresponse and missing data, setting a final target of n = 1201 participants.
Data Collection Tool
A structured questionnaire was used to collect the following data: (1) sociodemographic data; (2) academic data including college, educational level, and current academic year; (3) medical history, exercise frequency; and (4) HRQoL using the 36-Item Short Form Health Survey (SF-36), which is a validated, reliable, and widely used, 36-question survey designed to assess an individual's HRQoL. It covers 8 key dimensions of health, including physical functioning (10 items), role limitations due to physical health problems (4 items), role limitations due to emotional problems (3 items) bodily pain (2 items), general health perceptions (5 items), energy/fatigue (4 items), and social functioning (2 items). Additionally, the scale has 2 summary dimensions: the physical component summary (PCS) and the mental component summary (MCS). Each of the SF-36 dimensions and summary measures has a score calculated using a specific method, scaled from 0 to 100. 17
Procedure
The questionnaire was designed and adapted for online self-administration. We deployed the questionnaire via Blackboard. Minor wording localization, and pilot testing (25 students) were undertaken to optimize readability and reduce completion time; no content or scale structure was changed. Internal consistency was high (overall α = .93; domain α ≥ .74).
The questionnaire link was also disseminated via students’ emails and social media groups and sent directly to phone numbers obtained from the university administration after ethical and official approval.
The questionnaire included a consent statement explaining the study objectives and participants’ rights prior to the start of the survey. The confidentiality of all participants was protected, and all personal information was irrelevant to unique identifiers. No compensation, financial or otherwise, was provided to the participants.
Data management and duplicate prevention: To minimize duplicate submissions, we implemented 3 safeguards. First, the survey link distributed via the university learning management system (Blackboard) was tied to single sign-on and restricted to 1 submission per university account. Second, for invitations sent by email, social media, or phone, the survey platform enforced 1 response per device/browser and automatically logged submission timestamps and nonreversible hashes of IP addresses to help detect duplicates. Third, we screened records with identical response patterns; when potential duplicates were flagged, we retained the earliest complete record and excluded the remainder prior to analysis. No direct identifiers were collected, and the technical hashes used solely for quality control were not retained in the final analytic dataset.
Statistical Methods
Data were analyzed using SPSS version 21 for Windows (IBM Corp., Armonk, NY). Descriptive statistics were used to present mean ± SD scores for SF-36 dimensions scores and frequencies and percentages for categorical variables. Cronbach's alpha was calculated to assess the internal consistency of the SF-36 scale and its subscales. Bivariate correlations were analyzed using Spearman's correlation to examine relationships between different SF-36 dimensions. Pearson's chi-square tests were used to assess associations between QoL domains and multimorbidity, as well as other factors. When ≥20% of cells had expected counts <5 (or any cell <1), 2-sided Fisher's exact test was used (α = .05).
The scores were categorized into poor (0-25), below average (26-50), above average (51-75), and excellent (76-100). We define “suboptimal health” as PCS/MCS ≤50 (combining “poor” and “below average”), versus >50 (“above average/excellent”). This binary definition used for the logistic models to reflect clinically relevant impairment. High-impact disease operationally defined as any condition that showed significant bivariate association with suboptimal PCS/MCS multivariable logistic regression was performed to identify predictors of poor physical and mental health. Dummy variables were created for factor categories that showed significant differences from other categories. Results were presented as odds ratios with 95% confidence intervals, and the goodness-of-fit was assessed using the regression coefficient (R2). Age, marital status, education level, and job status were omitted from the poor physical health model and family income from poor mental health because they were not significant in bivariate screening
Results
Out of 1201, the study included 1173 participants who completed the questionnaire yielding a completion rate of 97.7%. The majority of the participants being female (60.3%), aged 20 to 29 years (69.9%), and Saudi citizens (93%). Over one-quarter of participants reported low income, while 11.9% were classified as high-income. Most participants were unemployed (84.3%), and the majority had living parents. Regarding academic data, 26.5% of participants were from Humanities & Social Sciences college and 11.3% from Health Sciences. Most students were pursuing bachelor's degrees (78.9%) (Table 1).
Sociodemographic Data (N = 1173).

Chronic diseases were reported by 45.3%, with 23.1% having ≥2 conditions. Anxiety (25.4%) and depression (17.5%) were the most common medical conditions, followed by asthma (10.8%). The majority exercised less than 60 min weekly (68.6%). Most participants were nonsmokers (81.5%) (Table 1).
The reliability of the SF-36 questionnaire in this study was excellent, with a Cronbach's alpha of .931 for the overall scale, and values ranging from .928 to .931 when any item was deleted. Subscale reliabilities varied, with Physical Functioning showing the highest Cronbach's alpha of .917, and Social Functioning the lowest at .736.
HRQoL Assessment
Mental health was lower than physical health (MCS 49.2 vs PCS 68.1). The weakest domains were Energy/Fatigue and Role-Emotional, whereas Pain and Physical Functioning were highest.
Above-average/excellent scores were 77.8% for Physical Functioning and 80.0% for Pain, with General Health 69.0%. PCS performance was strong (81.7% above/excellent), while emotional domains and to a lesser extent Social Functioning (57.1%) were comparatively lower, consistent with a pronounced mental–physical gap (Table 2).
Quality of Life Levels by SF-36 Domain and Subscale.
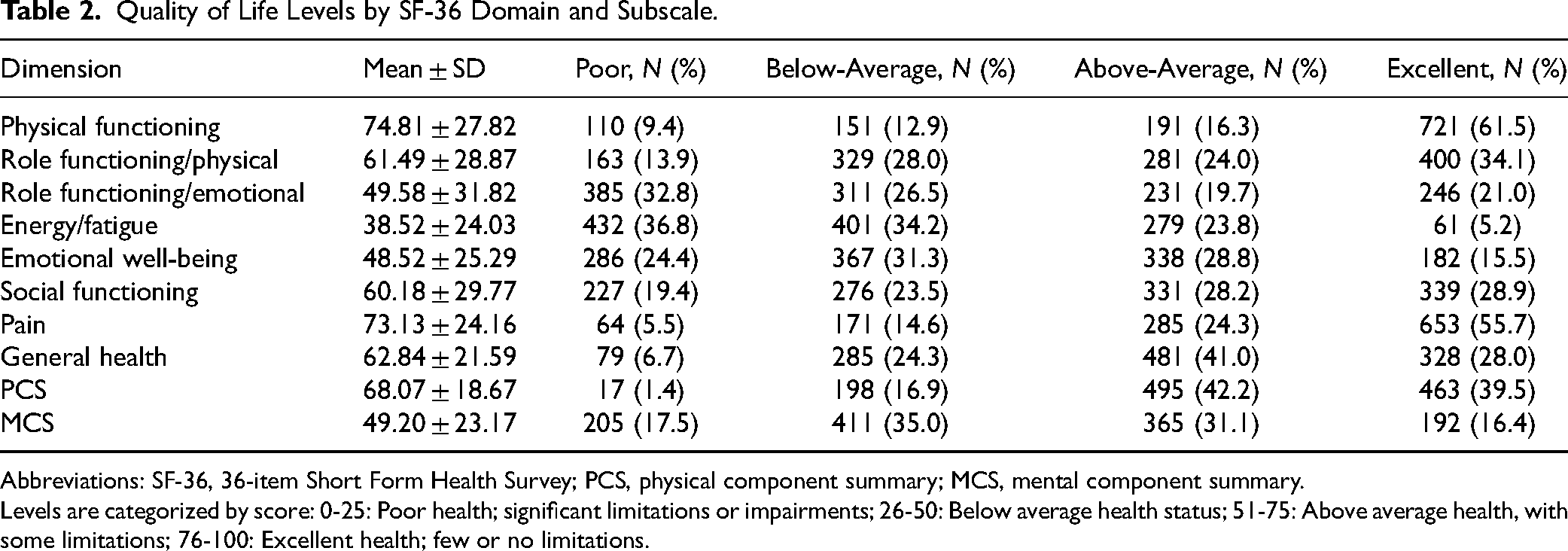
Abbreviations: SF-36, 36-item Short Form Health Survey; PCS, physical component summary; MCS, mental component summary.
Levels are categorized by score: 0-25: Poor health; significant limitations or impairments; 26-50: Below average health status; 51-75: Above average health, with some limitations; 76-100: Excellent health; few or no limitations.
Suboptimal mental health was significantly associated with female sex, older age, nonmarried status, college type, lower education level, job status, and lower exercise minutes.
Suboptimal physical health was associated with female sex, college type, current study year, lower family income, and lower exercise minutes. The direction of effects was consistent with expectations: female sex, lower income, and less weekly exercise corresponded to higher proportions of suboptimal outcomes, whereas greater exercise was associated with better HRQoL (Supplemental Table 1).
Strong and consistent associations with both suboptimal physical and mental health were observed for depression and anxiety, and for the cumulative count of high-impact diseases, which showed a clear dose–response (poor physical: 13.3%-73.9% from 0 to 3+; poor mental: from 44.9% to 82.6%). Suboptimal physical health was additionally associated with hypertension, heart disease, asthma, rheumatoid arthritis, osteoarthritis, and sickle-cell disease (all significant), whereas most of these conditions did not show parallel significance for mental health. Cardiometabolic risks such as type 2 diabetes and hypercholesterolemia were not significant in this unadjusted analysis, and several conditions with very small cell counts (eg, Chronic Obstructive Pulmonary Disease [COPD], cancer, thalassemia, epilepsy) yielded nonsignificant Fisher tests interpret with caution due to low number of cases. Overall, the pattern suggests that psychiatric comorbidity and greater multimorbidity burden drive poorer MCS, while specific cardiovascular, respiratory, musculoskeletal, and hemoglobinopathies contribute more to PCS impairment (Supplemental Table 2). In multivariable models, female sex, lower income, studying other than health sciences, advanced study year (sixth), low physical activity, and greater high-impact disease burden were associated with higher odds of suboptimal physical health, whereas greater weekly exercise was protective. For mental health, female sex and high-impact multimorbidity showed strong adverse associations, while greater exercise remained protective; most other demographics were not independently associated (Table 3).
Predictors of Suboptimal Physical and Mental Health (Multivariable Logistic Regression).

Multivariable logistic regression. Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; Ref: category used as reference to calculate the OR;
Dummy variable.
*Statistically significant variable (P < .05).
Discussion
The study assessed the prevalence and impact of multimorbidity on HRQoL among university students in the western region of Saudi Arabia, highlighting the importance of addressing the complex interplay of physical, mental, and sociodemographic factors in improving students’ overall well-being. The study included 1173 participants, from varying socioeconomic and academic backgrounds.
While the university students showed overall good physical health, their mental well-being is significantly compromised, with the majority displaying poor or below-average summary scores for mental health. The most impacted dimension was Energy/Fatigue, which may indicate a combination of physical and psychological strain, possibly due to academic stress and other pressures.
HRQoL has been extensively explored among university students in Saudi Arabia across various colleges and faculties. Consistent with our findings, Malibary et al observed that self-reported overall HRQoL was good or very good in 73.3% of medical students at King Abdulaziz University in 2016, using the World Health Organization Quality of Life-brief version (WHOQOL-BREF) questionnaire. However, the study found the lowest HRQoL score was for physical health followed by social relationships, while the mean score for psychological health was optimal. 18 Similarly, in Riyadh, Talakey et al observed poorer physical well-being scores among students from various healthcare colleges at King Saud University, using the WHOQOL-BREF questionnaire. 19 In contrast, a study at King Khalid University in Asir, encompassing various colleges and using the SF-36 questionnaire, showed findings similar to ours. The authors reported the highest scores for physical functioning and lower scores for Role limitation/Emotional and Energy/Fatigue, with the Pain domain showing the lowest scores (38.47 ± 25.58). 20 Internationally, a study by Milic et al that used SF-36 showed lower MCS scores than PCS scores among students in Serbia. 21
These discrepant findings are probably related to the difference in the scale used, with SF-36 likely being more sensitive to mental well-being than the WHOQOL-BREF. Another explanation for this difference is the specific characteristics of the population, particularly the students’ field of study. Overall, these observations indicate poor HRQoL among university students, notably regarding psychological well-being. Further analysis from the study by Malibary et al showed a negative relationship between psychological health scores and Grade Point Average (GPA) among medical students, likely reflecting the effect of academic pressure on mental well-being. Several mechanisms may underlie the compromised mental well-being. University students face converging stressors, academic load, sleep disruption, financial pressures, and social transitions that can depress mood, energy, and emotional role performance without necessarily impairing mobility or pain. 18 This is consistent with international data showing the substantial effect of academic stress and burnout on students’ HRQoL. 16
These findings highlight the importance of considering the psychological well-being of university students. 22
Our study found a high prevalence of multimorbidity with anxiety and depression being the most frequent conditions, followed by asthma. While multimorbidity has been scarcely explored in the specific population of university students, findings from comparable populations showed similar conclusions, data from a longitudinal study, the 1993 Pelotas Birth Cohort, showed a higher prevalence of multimorbidity among children and young adults, with a continuous increase in prevalence risk with age, from 26.3% at 11 years to 37.9% at 22 years. 23 In Kuwait, Ziyab estimated the prevalence of allergic multimorbidity among 1154 students, focusing on allergic diseases. The author found that 7.9% of the students had allergic multimorbidity, with asthma and rhinitis being the most frequent pattern observed in 5.1%. 22 In youth, international literature highlights the frequent co-occurrence of anxiety and depression with certain physical chronic diseases, notably asthma, allergies, and epilepsy. 11
The observed high rates of depression and anxiety are concerning, as they may increase the risk of developing physical multimorbidity in adulthood, predicting poorer health outcomes. A cohort study from the United Kingdom showed that the presence of depressive symptoms in early adult life is associated with an odds ratio of 1.58 to 1.67 for developing physical multimorbidity later in life. 24 In Saudi Arabia, data from a national population-based study showed a high prevalence risk of major depressive disorder and generalized anxiety disorder (12.7% and 12.4%, respectively), with no differences observed across all adult age groups. The authors emphasized the substantial gap between these figures and the actual number of diagnosed and treated individuals. 25 A systematic review of local studies on students observed even higher rates of depression, ranging from 30.9% to 77.6%, depending on the study, due to methodological variations. The review also found differential rates across colleges, with medical students experiencing the greatest burden. 26 Internationally, a systematic review and meta-analysis of 64 studies showed comparable figures for depression and anxiety (pooled prevalence of 33.6% and 39.0%, respectively) among college students, with higher rates in the African region, lower-middle-income countries, and among medical students. The authors observed higher rates in studies conducted after the COVID-19 pandemic outbreak, indicating an increasing trend of psychiatric morbidity among this population. 27
This data highlights the importance of early identification and intervention for both mental and physical health conditions among university students to prevent the escalation of multimorbidity. Addressing the co-occurrence of psychiatric and physical disorders is crucial for enhancing patient outcomes and treatment strategies through integrated care approaches.
Multimorbidity significantly impacted students’ HRQoL, affecting all domains and showing a dose-dependent effect, particularly the accumulation of certain specific high-impact diseases. This is consistent with reports from children having different physical conditions, showing the severe impact of multimorbidity on physical and psychological well-being as well as school environment, with fair-to-good agreements between parent and children reported HRQoL scores. The dose-dependent effect was also demonstrated notably for mental disorders. 13 This is also further consistent with studies among adults showing a linear correlation between the number of comorbid diseases and the percentage decrease in HRQoL scores, ranging from 1.6% to 4.4% for each additional comorbidity, depending on the HRQoL scale used. 8
Other comorbidities showed a relatively greater impact on HRQoL. These include asthma, COPD, sickle-cell disease, thalassemia, and cardiovascular diseases. More specifically, thalassemia, asthma, COPD, and osteoarthritis showed an independent relationship with the physical component of HRQoL, but not with the mental component, indicating the significant impact of these morbidities on physical well-being. Both asthma and COPD are associated with poor HRQoL, impacting various domains. These conditions are also linked to a high risk of mental comorbidities, notably depression and anxiety, as well as reduced quality of sleep, which further affects HRQoL.28,29 Regarding thalassemia, a study showed that children with thalassemia had the lowest HRQoL scores compared to children with cancer and those undergoing hemodialysis, indicating that thalassemia has a more profound impact on overall well-being in this population. 30
In addition to multimorbidity and health-related factors, students’ HRQoL is impacted by other socioeconomic factors. In the present study, male gender, high family income, and regular exercise were protective factors of physical and mental well-being. This is consistent with reports of QoL studies showing the significant contribution of environmental and behavioral factors in shaping physical and mental well-being among university students and the general population.13,1618–21,31 The cumulative effect of these factors with multimorbidity indicates the relevance of addressing socioeconomic and behavioral factors, such as promoting regular exercise, supporting low-income students, and considering gender-specific interventions, can significantly improve students’ physical and mental well-being. By focusing on modifiable risk factors, such as lifestyle habits and social determinants, universities and public health authorities can help mitigate the negative effects of multimorbidity on QoL. Moreover, integrating these protective factors into public health strategies may contribute to reducing health disparities and fostering a more supportive environment for students. Furthermore, universities must establish robust mechanisms to ensure access to healthcare services, enabling timely interventions and comprehensive support for students facing complex health challenges.
The limitation of this study is the cross-sectional design, as it prevents establishing causal relationships between multimorbidity and HRQoL. Additionally, the reliance on self-reported medical history and SF-36 may introduce reporting bias. Use of an open survey link prevents precise calculation of a standard response rate and may introduce selection bias; findings should be generalized primarily to similar student populations. Another limitation is the lack of additional factors that could help explain HRQoL. Despite these limitations, this study is one of the few addressing multimorbidity among university students and its impact on HRQoL. Future studies should consider longitudinal designs, incorporate objective health measures, and explore additional factors influencing HRQoL, such as environmental, access to health services, and behavioral aspects.
Conclusions
University students exhibit lower mental health well-being and a high multimorbidity burden that require urgent attention and targeted interventions. With a prevalence of 23.1%, multimorbidity was significantly associated with poorer QoL across both physical and mental health dimensions, with a dose-dependent effect observed. In addition to the most common comorbidities such as anxiety, depression, and asthma, certain conditions have been shown to have a greater effect on HRQoL. This emphasizes the need for early identification and intervention, stressing the importance of integrated care approaches that address both physical and mental health in university students.
The study also highlighted the crucial role of sociodemographic factors such as gender, family income, and exercise habits in shaping both physical and mental well-being, reinforcing the importance of addressing modifiable risk factors in student populations. Targeted interventions are required, including implementing support programs and developing campus-based wellness programs that address the physical, psychological, and social factors of student well-being.
Future studies should explore the long-term effects of multimorbidity on HRQoL among students through longitudinal design studies and consider incorporating objective health measures. Additionally, expanding research to address the environmental and behavioral factors will provide a more comprehensive understanding of how to mitigate the adverse effects of multimorbidity, ultimately improving student well-being and academic outcomes.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251413851 - Supplemental material for Health-Related Quality of Life and Its Association With Multimorbidity Among University Students in Jeddah, Saudi Arabia: A Cross-Sectional Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735251413851 for Health-Related Quality of Life and Its Association With Multimorbidity Among University Students in Jeddah, Saudi Arabia: A Cross-Sectional Study by Rajaa Mohammad Al-Raddadi, Abdullah Aburass, Musab Abdulbasit Bukhari, Owiss Hassan Alzahrani, Sulhi Ali Alfakeh, Moroj Ahmad Aldarmasi, Shaymaa Abdalal, Maha Alattas and Fouad Abolaban in Journal of Patient Experience
Footnotes
Acknowledgments
The authors acknowledge with thanks DSR for technical and financial support, and Dr Hanan Basheir for her assistant in data collection.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Rajaa Al-Raddadi, Abdullah Aburass, and Musab Bukhari. The first draft of the manuscript was written by Rajaa Al-Raddadi and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of KAU (Date June 2022/No287-22), and informed consent was obtained from all individual participants included in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah under grant no (GPIP: 1414-140-2024).
Informed Consent
The questionnaire included a consent statement explaining the study objectives and participants’ rights prior to the start of the survey. The confidentiality of all participants was protected, and all personal information was irrelevant to unique identifiers. No compensation, financial or otherwise, was provided to the participants, mentioned in the manuscript (Method section, Procedure).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.