
Abstract
Patient satisfaction is a key determinant of healthcare quality; however, its assessment in stroke prevention clinics (SPCs) remains inadequate. This quality improvement (QI) project aimed to establish a baseline for patient experience at an SPC in Northeastern Ontario. Our QI team developed a satisfaction survey based on the Donabedian Model. Conducted over 30 days in July 2025, 43 of 51 invited patients completed the survey, resulting in an 84% response rate. Qualitative feedback was gathered for the thematic analysis. Patients reported high satisfaction across the Donabedian framework domains, with over 90% understanding their care steps and feeling dignified. Pareto analysis identified discharge education as a key area for improvement. Despite an 88% satisfaction rate, this domain was prioritized to enhance post-discharge patient preparedness, potentially reducing readmission risk. A limitation of this study was the small, single-site, and brief data collection period. This initiative established a baseline for patient experience and highlighted post-discharge education as a critical area of improvement.
Background
Stroke ranks as the second leading cause of death worldwide and the third when considering both mortality and disability together. 1 Preventing stroke, especially through secondary measures following a transient ischemic attack (TIA) or minor stroke, is a crucial priority for contemporary healthcare systems today.1,2 Outpatient stroke prevention clinics (SPCs) play an essential role in this preventive approach by providing rapid diagnostic assessments, optimizing medical management, and educating patients on modifiable risk factors, which include the adoption of healthier lifestyles. The demonstrated effectiveness of SPCs in reducing stroke recurrence is a key performance indicator for these specialized services.3,4
Beyond traditional clinical metrics, patient experience has gained global recognition as a vital dimension of healthcare quality. 5 For stroke survivors, the quality of their experience is strongly associated with measurable health outcomes. 6 Patients who perceive their care as respectful, attentive, and well-coordinated are more likely to adhere to complex medication regimens and manage their long-term health, which is critical for reducing recurrent risk.7,8 This approach emphasizes patient-centered care, aligning with the Institute for Healthcare Improvement's Triple Aim, which highlights patient experience as a core component of high-quality healthcare. 9
Health Sciences North (HSN), a comprehensive stroke center in Northeastern Ontario, is dedicated to providing patient-centered care. 10 However, within its SPC, patient experience is captured only informally, limiting its consistency and reliability for quality improvement (QI) services. 11 The absence of a systematic approach represents a significant gap, as the formal assessment of patient satisfaction is essential to align clinical quality with patient-perceived outcomes. To address this gap, we undertook a structured QI initiative to develop, implement, and evaluate a standardized patient experience survey. This initiative aimed to establish a reliable baseline, generate actionable patient-reported data, and provide a framework for ongoing QI efforts, ultimately strengthening the alignment between clinical effectiveness and patient-centered care.
Methods
Study Design
This QI initiative, part of the MOTIVE (MObile TIA and Stroke with AdaptiVE Workflow) Project, was guided by the IHI Model for Improvement.12,13 This QI project was reported in accordance with the Standards for Quality Improvement Reporting Excellence (SQUIRE) guidelines. 14
Ethics
The HSN Research Ethics Board granted exemption from formal review in accordance with the Tri-Council Policy Statement 2 (TCPS 2), as its purpose was to improve healthcare services rather than conduct research.
Aim Statement
The first Plan, Do, Study, Act (PDSA) cycle aimed to establish a structured process for collecting patient feedback at the SPC, with the goal of achieving a baseline satisfaction rate of at least 80% across surveyed domains and identifying at least one priority area for improvement.
Setting and Participants
The QI project was implemented at HSN, Ontario, Canada. Data were collected over a 30-day period in July 2025. Patients diagnosed with TIA or stroke who attended the SPC were eligible for participation. In instances where patients were unable to complete the survey due to cognitive, speech, or physical impairments, such as aphasia, a primary family member or caregiver was invited to respond on behalf of the patient.
Intervention
The QI team comprised of a stroke neurologist, an advanced practice physiotherapist, a stroke nurse, and administrative leaders from the SPC, Medicine Program and Regional Stroke Program who developed a concise and pertinent patient experience survey tool. Through a series of brainstorming sessions and iterative refinements, the team crafted a questionnaire reflecting the typical journey of a patient at the SPC. 15 The final survey consisted of 11 questions using a 4-point Likert scale (definitely = 4; mostly = 3; somewhat = 2; definitely not = 1) to quantify responses, supplemented by two open-ended questions to capture qualitative feedback, thereby acknowledging the importance of insights beyond structured data. 16 The draft survey was reviewed by two patients for relevance and clarity, both of whom affirmed the content without suggesting modifications. The survey (Table 1) was subsequently implemented at the SPC, available in both English and French, with stroke nurses inviting patients to participate in a brief, anonymous online survey, on a voluntary basis, upon completion of their initial visit to the SPC.
Development of a Patient Satisfaction Questionnaire Utilizing the Donabedian Framework. 18

Data Analysis
At the end of 30 days, the data were systematically compiled into an Excel spreadsheet for detailed analysis. The response percentages for each survey question were calculated and represented using bar charts. A Pareto chart was constructed to prioritize the survey domain based on the proportion of “defects,” enabling quick identification of strengths and areas needing enhancement. 17 Responses labeled “Not applicable” were omitted from the percentage calculations for relevant items (eg, test or medication explanations) to ensure that the analyses accurately represented only pertinent responses. This methodological choice minimized potential bias and avoided the underestimation of satisfaction scores for items that were not relevant to all participants.
Qualitative data obtained from the open-ended survey questions were transcribed and subjected to thematic analysis to identify recurring patterns and insights. The analysis followed Braun and Clarke's six-step framework, which includes familiarization, coding, theme generation, review, definition, and reporting. 19 One reviewer (V.R.) independently coded the data, organized the quotations, and developed the initial thematic diagram. Two additional reviewers (C.L. and S.B.) assessed the coding structure and validated the emerging themes using the validation form. Consensus on the final themes was achieved through team discussions.
Results
Participant Characteristics
In July 2025, 51 patients attending the SPC were invited to complete a patient-experience survey, and 43 participants (84%) completed the survey. The survey was designed to establish a baseline understanding of patient satisfaction and identify areas for QI. Table 2 presents respondents’ characteristics.
Participant Characteristics n = 43.

Referral to the SPC
The majority of patients were referred to the SPC by their family doctor (n = 12), followed by a stroke neurologist (n = 6) and the Emergency Department at HSN (n = 5). Additional referrals were made by specialists (n = 3), nurse practitioners (n = 2), or other sources (n = 1).
Care Experience
As shown in Table 3, overall, the patients reported high levels of satisfaction with the care they received. A significant number of patients indicated that they “Definitely” understood the next steps in their care (91%), received sufficient information about what to do if they were concerned about their condition after returning home (88%), and found the instructions for preparing for their appointment clear and understandable (90%). All respondents (100%) felt that doctors and nurses treated them with dignity and respect. Furthermore, 93% of the patients felt that the doctor explained things in an easy-to-understand manner, and 95% stated that the doctor provided clear instructions about their follow-up care. Similarly, all patients (100%) felt that the nurse explained things in an easy-to-understand manner, and 95% received clear instructions about follow-up care from the nurse.
Patient Satisfaction Survey Results.

A total of 79.1% of participants reported that the physician or nurse “definitely” clarified the rationale behind the ordered tests, while 18.6% chose “not applicable.” Similarly, 60% of participants reported that the explanations concerning medications were “definitely” clear, whereas 37% selected “not applicable.” These findings indicated that certain questions were not relevant to all patients, as some did not require new tests or medication modifications during their visits. As a result, “not applicable” responses were omitted from the denominator calculations to ensure that satisfaction percentages accurately reflected only pertinent responses. Consequently, the QI team did not view lower percentages in these areas as signs of dissatisfaction but rather as indicative of the relevance of the questions.
Qualitative Feedback
The survey was completed by 43 patients, among whom 19 provided qualitative comments, 21 offered no feedback, and three explicitly stated that they had no additional remarks. The qualitative responses (n = 19) were analyzed thematically by one reviewer (V.R.) using Braun and Clarke's six-step framework, resulting in the development of themes (Table 4). The analysis identified three major themes: compassionate care, trust and confidence, and effective communication, and 13 subthemes: empathy, respect, professionalism, teamwork, comfort, reassurance, gratitude, pleasant environment, timeliness, efficiency, relief, listening, and informativeness. To ensure analytic rigor, two additional reviewers (C.L. and S.B.) independently reviewed and voted on the thematic map, confirming the clarity and representativeness of the study's final framework (Figure 1). Patients frequently described their care as “excellent,” “caring,” and “compassionate,” reflecting their strong trust and reassurance in the clinical teams. They valued professionalism, timely access, and clear communication, all of which collectively reduced their anxiety and enhanced their satisfaction. These findings align with Donabedian's quality of care framework, where compassionate and communicative processes of care contribute to trust and confidence and satisfaction in the SPC.
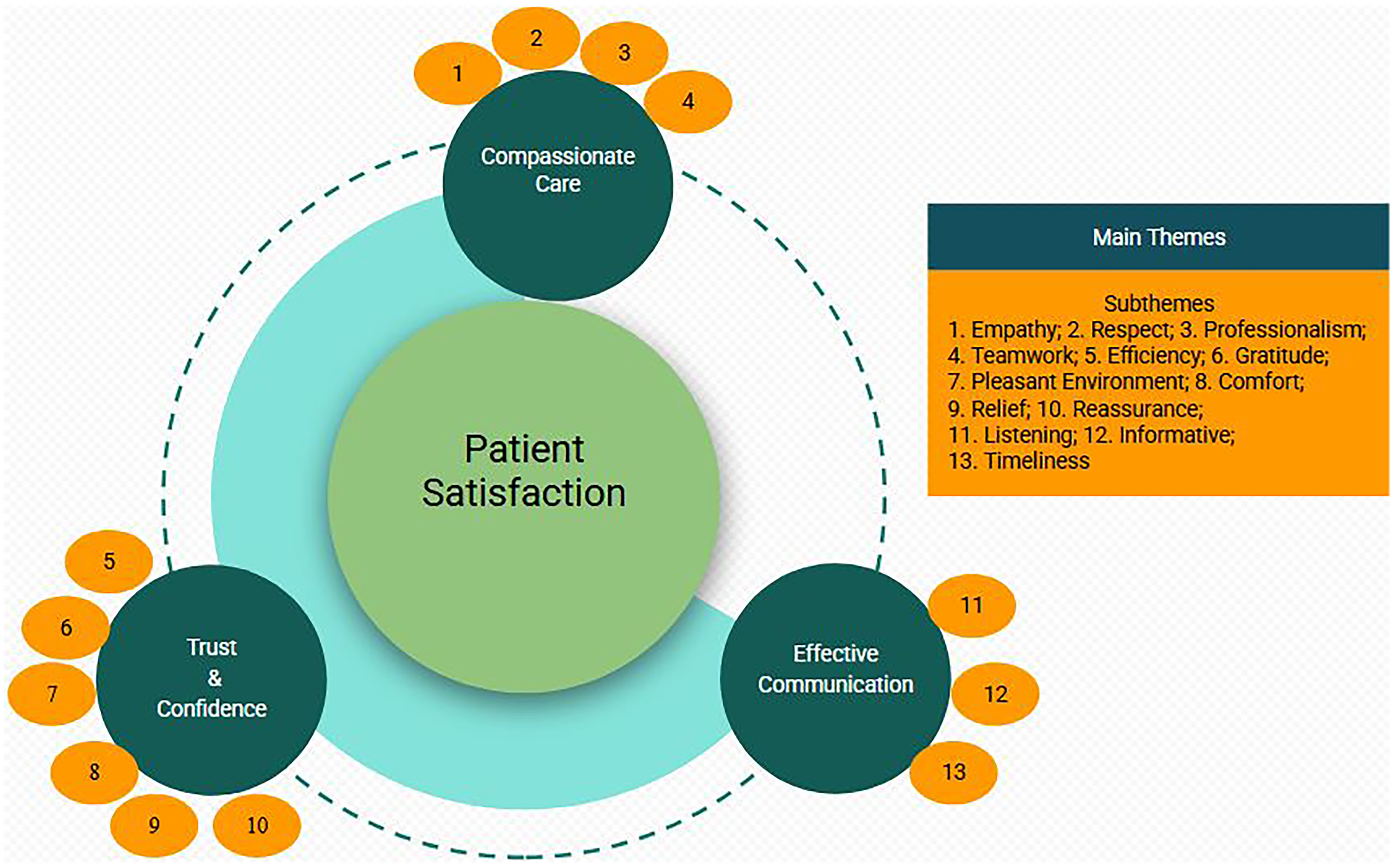
Thematic Conceptual Model of Patient Satisfaction in the Stroke Prevention Clinic.
Main Themes, Subthemes, and Patient Quotes From Stroke Prevention Clinic Survey.

The initial objective of achieving an 80% satisfaction rate across all three domains was achieved. However, a subsequent Pareto analysis was conducted to identify areas that still required QI (Figure 2). Survey items were prioritized based on the proportion of “defects” (responses below “Definitely”) to determine key areas for intervention. The 95% confidence intervals for all proportions were calculated using the exact binomial method and are detailed in Table 3. The analysis identified the post-discharge information domain as having the highest concentration of defects (12%) with an 88% satisfaction rate. Given that clarity of post-discharge instructions is associated with better patient preparedness and continuity of care, the QI team will focus on improving this metric to exceed 90% satisfaction in the next PDSA cycle. The team plans to develop standardized educational materials tailored to patients’ needs to enhance their comprehension of post-discharge care instructions.

Paretochart % Defects by Survey Category.
Discussion
This QI initiative demonstrated the feasibility of conducting patient surveys in ambulatory SPCs, with a high participation rate (84%). This study also highlights the value of systematically evaluating patient satisfaction in assessing healthcare services within the Donabedian framework. The survey results revealed high satisfaction rates, particularly in communication, respect, and follow-up care, highlighting the central role of patient-centered interactions in stroke care quality. The survey also identified targeted opportunities for improvement, particularly in post-discharge education. The Donabedian framework provides a structured foundation for survey development, ensuring that the structural, process, and outcome domains are addressed. 18 This approach allows the QI team to move beyond anecdotal impressions, establish a baseline dataset, and guide further improvement cycles. Embedding patient-reported experience measures into routine SPC practice is also consistent with Canadian Best Practice Recommendations, reinforcing the importance of integrating patient voices into quality monitoring. 2
Although the goal of achieving an 80% or higher level of patient satisfaction was met, Pareto analysis identified a key area for improvement: enhancing post-discharge education, especially regarding steps patients should take if concerns arise after their clinic visit. Addressing this gap is clinically significant, as providing patients with thorough post-discharge information is associated with fewer hospital readmissions, higher treatment adherence, and higher patient satisfaction. 20
Previous research has demonstrated a correlation between enhanced post-discharge education and improved patient outcome. Previous studies have demonstrated enhanced adherence to treatment recommendations with positive care experiences. 8 However, our QI project did not collect data on adherence to treatment recommendations or readmissions during the first phase of this project. Therefore, we were unable to assess the correlation between post-discharge education level and these outcomes. To enhance the evidence base in future iterations, we plan to incorporate follow-up metrics, such as treatment adherence and readmission rates. This methodology will allow the QI team to evaluate whether improved post-discharge education leads to tangible system-level benefits. We will also assess its applicability beyond a single site in the next phase of this project. Future work will also assess the impact of standardized educational tools on patients’ confidence in self-management and patient experience. Thematic analysis of our survey was encouraging with team being described as “caring,” “compassionate,” and “excellent.” Such feedback highlights the relational aspects of care that foster trust and satisfaction, echoing the broader literature on the importance of dignity and respect in patient–provider interactions.
Limitations
The QI initiative had several limitations. The small sample size (n = 43), single-site design, and short 30-day data collection period limit the generalizability, although the primary aim was to establish a baseline for future improvements. Underrepresentation of individuals with cognitive or communication in the present survey make generalizability of the study finding to this population. Also, survey might require reliance on caregiver or proxies in this population who may perceive empathy differently from that of patients. High satisfaction ratings may suggest ceiling and social desirability effects influenced by the Likert scale and may reflect local workflows. A gratitude bias was also evident in the qualitative comments expressing appreciation for the staff, possibly inflating satisfaction ratings. The survey instrument was not psychometrically validated and baseline measurements were prioritized over instrument validation. Future PDSA cycles will expand to additional SPC in northeastern Ontario and extend data collection and analysis of relationships between patient experience, post-discharge education, and clinical outcomes, such as readmissions and treatment adherence.
Conclusion
The implementation of a structured patient experience survey in an SPC is feasible and valuable for guiding service improvements. The initiative established a baseline for patient-reported data which confirmed high levels of patient satisfaction with the care received within the SPC. It identified targeted opportunities for improvement, particularly the area of post-discharge education.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This innovative quality improvement project was exempted by the Health Sciences North Research Institute in accordance with TCPS2 Article 2.6 p.20.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is a component of the MOTIVE project, which has received funding from Ontario Health's Models of Care Innovation Fund (grant number 25-21).