
Abstract
Physical exercise and cognitive training have the potential to enhance cognitive function and mobility in older adults at risk of dementia. However, little is known about the experience of receiving such interventions in the home settings of older adults. Fifteen participants (mean age 70.8 years) who completed the 16-week interventions of SYNERGIC@Home feasibility trial were interviewed to understand participants’ engagement in home-based physical and cognitive exercise interventions delivered one-on-one through videoconferencing. Grounded theory data analysis was completed collaboratively by qualitative researchers. Results show that participants’ engagement was driven by personal connection to dementia and mediated by relationships fostered largely with individual exercise trainers. Participants were also invested in the greater good (wanting their participation to make a difference to dementia research), their own outcomes, or their family's and society at large. Overall, they reflected on their participation as a rich learning experience. We propose that the quality of interpersonal connections and personalized support are of primary importance for older adults to stay engaged in physical exercise and cognitive training programs delivered remotely.
SYNERGIC@Home trial registration number: NCT04997681, https://clinicaltrials.gov/study/NCT04997681
Keywords
Introduction
Prevention of Alzheimer's disease and related dementias (ADRD) is of great interest to governments, healthcare providers, and communities worldwide. Physical inactivity, impacting nearly 80% of Canadians, is one of the most important modifiable risk factors of dementia.1,2 Often, interventions aiming to lower dementia risk take place in clinical or academic settings. However, limited reach and capacity, transportation challenges, and the COVID-19 pandemic have accelerated the spread of remotely delivered care and interventions. While home-based exercise interventions tend to have high retention rates in older adults, 3 little is known about how participants of this age group describe their experience. In two studies reporting high retention and adherence, virtually delivered home-based exercise programs lasting 4 or 12 weeks in duration were respectively rated as enjoyable by most participants 4 with an appreciation for flexible delivery. 5 To our knowledge, no qualitative study has explored the experience of older adults in remotely delivered interventions composed of physical exercise and cognitive training.
We explored participants' experience in a randomized controlled trial (RCT) examining the feasibility and acceptability of a remotely delivered ADRD prevention program to older adults. This trial, registered as SYNERGIC@Home, consisted of a 16-week one-on-one physical exercise and cognitive training intervention 3 times a week with trained assistants through Zoom for Healthcare™ to one of four possible intervention arms, including pre- and post-neuropsychological assessments. 6 Retention and overall adherence rates were 86.7% and over 81%, respectively.7,8 This nested qualitative study aimed to understand the experience of older adults who are at risk for dementia and participate in a remotely delivered, home-based intervention aimed at improving mobility and cognition.
Methods
Design
A grounded theory qualitative design9,10 was used to collect and analyze the data obtained from semi-structured interviews with study completers of the 16-week interventions and first post-assessments (T4 assessments, 4 months after randomization) of the SYNERGIC@Home feasibility trial. This design was adopted to uncover how the participants adhered to and completed the trial. Details about the interventions and feasibility outcomes examined in this double-blinded RCT have been reported earlier. 6 The COnsolidated criteria for REporting Qualitative research (COREQ) Checklist 11 (Supplemental Material S1) was used for reporting the qualitative study, which was approved by the Research Ethics Boards of Horizon Health Network, Réseau de santé Vitalité, University of New Brunswick, and Université de Moncton.
Assumptions
As a discovery method, grounded theory is valuable in exploring little-studied phenomena 9 such as the experience of older adults in a home-based dementia prevention study. While no systematic literature review was undertaken in planning this study, as per grounded theory approaches, 10 some assumptions were implied in its design. Firstly, the researchers assumed, prior to commencing the study, that remotely delivered interventions may influence dropout rates. Second, they were aware that COVID-19 pandemic mitigation measures increased the use of remote visits in healthcare and other sectors, and this ignited curiosity about the experience of older adults in remote clinical interventions. Finally, while blinded, researchers knew that RCT participants had been allocated to different intervention arms prior to participating in the qualitative study.
Setting and Participants
Participants in SYNERGIC@Home were community-dwelling alder adults (60-90 years old) at risk of dementia living in urban and rural settings across the province of New Brunswick, Canada. Recruitment for this trial was performed from July 2021 to July 2023 using posters and announcements on community and healthcare provider websites, on public and social media, and in physician offices. Interested individuals were screened for eligibility using predefined inclusion and exclusion criteria (Table 1). All study activities took place exclusively online through Zoom for Healthcare™ (Zoom Video Communications, 2021). Sixty participants were randomized to one of the four intervention arms (Table 1), 57 initiated the interventions, and 52 participants identifying as White completed the intervention program and T4 assessments (mean age 68.8 ± 5.7 years, 41 women). 8 They all had at least a high-school-level education. The research coordinator invited 20 participants who completed the interventions and T4 assessments between October and December 2022 to participate in the qualitative study. Purposive and convenience sampling was used to help ensure diverse representation across intervention arms, location of residence (rural/urban), preferred language (English/French), and sex at birth (Table 1). Fifteen consented to participate and were interviewed (mean age 70.8 ± 6.3 years, 11 women). Their anonymized sociodemographic characteristics are presented in Table 2.
Participation Criteria for SYNERGIC@Home RCT 6 and Sequential Grounded Theory Study.
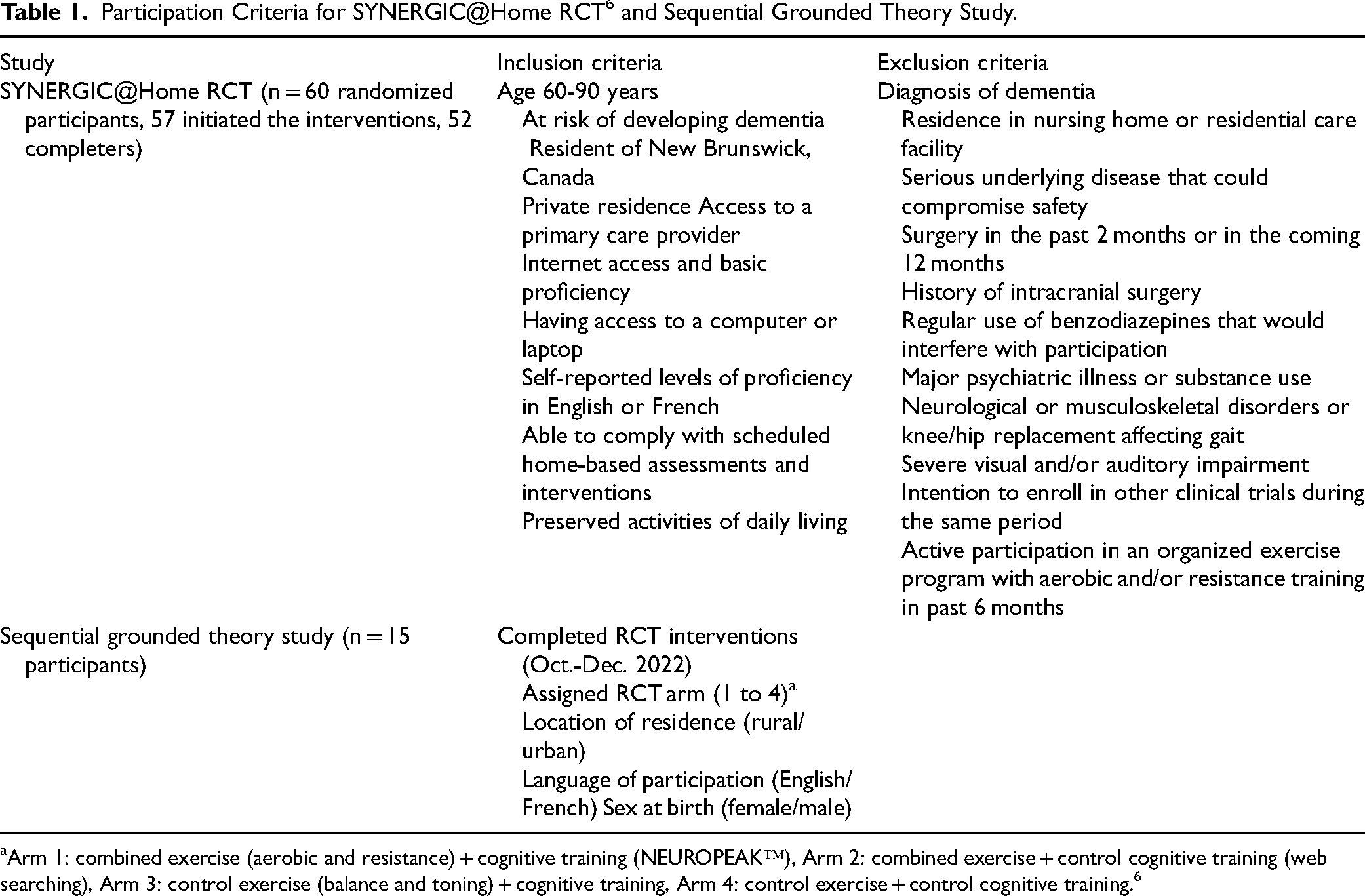
Arm 1: combined exercise (aerobic and resistance) + cognitive training (NEUROPEAK™), Arm 2: combined exercise + control cognitive training (web searching), Arm 3: control exercise (balance and toning) + cognitive training, Arm 4: control exercise + control cognitive training. 6
Sociodemographic Characteristics of Participants in the Grounded Theory Study.

F: female, M: male.
According to Statistics Canada (2023). 27
Arm 1: combined exercise (aerobic and resistance) + cognitive training (NEUROPEAK™), Arm 2: combined exercise + control cognitive training (web searching), Arm 3: control exercise (balance and toning) + cognitive training, Arm 4: control exercise + control cognitive training.
Data Collection
Semistructured interviews (45-90 min) were conducted in participants’ preferred language by bilingual research team members (LY, CCT, MG), following an interview guide (Supplemental Material S2) that was previously piloted in two mock interviews (English and French). Interviewers were blinded to the intervention arm and had no prior relationship with participants. Field notes were taken after each interview, which was conducted via Zoom for Healthcare™ and audio-recorded. Transcripts were prepared using intelligent verbatim transcription 12 and analyzed in their original language in NVivo 12 (QSR International Pty Ltd, Doncaster, Australia). Each participant was assigned a study number to maintain confidentiality. Sociodemographic characteristics and intervention arm were recorded as part of the RCT but were unblinded only after qualitative analysis. Observations from the larger RCT informed analytical memos to contextualize findings.
Data Analysis
Thematic analysis13,14 was used by the qualitative team (first five authors) as a common coding strategy. The positionality statement of these researchers noted that they had different occupations as health professionals, in either academia or healthcare settings, and were based in different regions of New Brunswick. They identified as cis-women and came from diverse cultural and linguistic backgrounds. Three reported having connections with Alzheimer's disease. Analysis took place in four phases, beginning after the first interview in the fall of 2022. In the first phase, the first 8 transcripts (all English) were divided among the qualitative researchers (HO, LY, CCT, MG, JH) for open coding, which was completed individually. In phase 2, researchers discussed the emerging codes to determine the most pertinent themes observed in the data to refine the codebook. In phase 3, French transcripts were divided among three French-speaking researchers (CCT, MG, and JH) for analysis in the original language using the codebook created in phase 2, while also looking for emerging codes. Simultaneously, LY and HO continued to analyze the English transcripts for further codes and to compare text within codes. In the fourth and final phase, the five analysts revisited the codebook to compare text by attributes (such as demographics) and emerging categories.
Data saturation was reached during phase 4, when consensus was achieved among analysts that no new codes were emerging. For instance, participants consistently described the interventions as convenient to access remotely. This code appeared in the first 5 transcripts and continued to recur without contradiction across subsequent interviews, demographic subgroups (eg, gender, rural/urban, treatment arm), and across coders’ files. At this point, researchers determined that additional data would not generate new themes regarding the remote delivery of the intervention. Throughout analysis, a theory grounded in the data was proposed and refined. The team continued looking for data that challenged the developing theory to help refine the analysis. In the final model, 70 concept codes were grouped into 6 higher-order codes by comparing the text coded under each concept, researcher's analytical memos, and the raw transcripts. 15 Second-order codes were summarized and presented to participants during member check, which took place in May 2023 to triangulate findings and get feedback on the developing theory. 16 After sending a description of the main themes to each participant, 12 provided feedback by email or videoconference with researcher MG, supporting the developing theory. We organized the 6 second-order codes into 4 axial categories describing conditions influencing participant experience in the RCT. Finally, through constant comparison,9,15 we uncovered the core category around which the 4 axial categories and 11 higher-order codes were organized.
Results
The resulting grounded theory (Figure 1) proposes that older adults engaged with the remotely delivered intervention program of physical exercises and cognitive training through finding meaningful personal connections with the overarching study goal (prevention of ADRD), protocol, personnel, and technology used to deliver the intervention. The finding of making meaningful connections emerged as a central phenomenon (core category), which was related to 4 main axial categories: “ADRD connection,” “Study protocol,” “Technology,” and “People.” As Gisèle described it, “It's about connections.” We defined meaningful connections as ways that participants build a relatable connection with various aspects of the study, including study personnel during the study. Higher-order codes (e.g., family history) describing connections to axial categories were organized around these in the visual and textual descriptions of the theory. Ubiquitous concepts describing outcomes of experiencing the study in participant interviews are represented by clouds in Figure 1 and discussed below. These findings are supported by the data, with clear links maintained between participants’ accounts and the categories identified. Pseudonyms are used to maintain anonymity.

“It's about connections”: A grounded theory of older adults’ engagement in a remotely delivered, home-based intervention with physical and cognitive exercises aimed to reduce the risk of dementia.
ADRD Connection
Connection to ADRD, defined as having personal experience or being touched by ADRD, was a driver of participation in the RCT. Participants wanted to make a meaningful impact on dementia research and contribute to benefiting themselves, their families, and the broader community. Lisa stated: My Mom had dementia and my stepdad had it. So, it was all around me and I wanted to do whatever I can to help basically. People that you listen to or talk to that have had situations with people that have suffered with dementia and that, and I thought “Is that going to be me a few years down the road?” (Michael) So, to me it's good and it's learning something new, it's being challenged, it's doing something for the greater good versus just my personal gain. Like, somebody is going to benefit from this somehow. So, all those things bring me enjoyment. (Karen) I thought well, if there are some things that I can do that would benefit the research community, but also that I can keep doing to benefit me, then that's great. (Louise) I did it for my mother-in-law, and I also because I know it's important. (Michelle)
Study Protocol
When describing their experience with study assessments and interventions, overall, participants viewed their involvement as an enriching learning experience rather than merely a volunteer or service experience. They describe study procedures as activating learning and lifestyle introspection, alluding to subtle behavioral changes such as rising early and consuming less alcohol. Participants described gaining awareness of body mechanics as they lift everyday items, such as grocery bags. Some learned new information about dementia and the importance of exercise for older adults who might be at risk for dementia. This new learning is evidenced in the following quote: I think I learned so much. I learned why it was so important for me to be stretching, (…) and you know, the importance of all of that stuff as we age. (Donna) Gaining my upper body strength from resistance training when I lift things and, when I do certain things, I’m mindful of the strength that I have in my upper body now. Which helps save my back. (Lisa) I liked the repetitiveness because we would build a little bit on that, and it was a very gradual change. So, I didn’t come away saying “Oh, I can hardly move.” It went very well. (Brenda) You don't have to lift weights or do, what do you call that, push-ups on the ground, but we will arrive at the same result. (Authors’ translation) (André) I won’t be sorry when this [cognitive assessments] is over [laughter]. I knew it was part of it, and I knew it had been explained. I knew what I was in for, but it does get tedious. (Karen) It gets pretty monotonous. It's the same thing over and over again. (Michelle)
Technology
Technology, for the purpose of our study, refers to tools and equipment (software, hardware, exercise equipment, synchronous videoconferencing) used to facilitate a particular activity. Some participants credited technology with being an important factor in being able to join and continue in the study due to their distant location from an urban center. One participant identified online communication as a new frontier for research that she felt compelled to help investigate as a platform: It's probably nice to have the COVID as the point to make people try different things so that it might make for interesting research in the future, and it might broaden the ability to do research. So, there is definitely some benefits to trying online research and doing this kind of stuff. (Tammy) It was a real learning curve for me. And as a result of this, I am now doing more online banking than I ever did and. I can do e-transfers now [laughs].
People
Experiences with study personnel and support people were frequently discussed as facilitating connection with and completion of the study. The meaning of people connections to study participants was generally described in terms of support from study staff and through their personal network that provided positive reinforcement to help sustain participation. In one case, a participant felt connection to concerned people (family members) created a sense of obligation to participate. A consistent key finding was the meaningful connections participants established with their assigned exercise trainers due to the participant-centered and synchronous nature of the physical exercise intervention. [Trainer’s name] was able to show me how to do it without it hurting my knees. I learned so much from him I can’t even tell you. Unbelievable personality, like amazing. He would answer any questions; he just told me anything I needed to know… I was gaining confidence. (Donna) I looked forward to the exercise sessions. I really did. I loved them. That was great. And I would be excited about doing that and wondering “What is she going to ask me to do?” (Janet) I’m not one to do a lot of physical exercise like, go to a gym or an exercise program on my own. Having someone like [trainer's name] and doing it over Zoom as well. Somebody to guide me. (Michael) Well, there was a lot, like [trainer’s name] gave a lot of feedback about posture and the correct way to do it and what to watch for and all that. They were very thorough about that. So, it was good to have this one-on-one. And they would do it along with me, so it was good. And I could see what their posture was, or movements were, and that worked out really well. (Tammy) We started off at a slower pace. [Trainer’s name] and I, she was just getting used to what my abilities were. [Trainer’s name] set the pace, and I was able to maintain that pace. And towards the end of it, I think we were going at a pretty good clip. (Michael) It's like we were more on our own. I think human connection was missing for this part. But there was a lot of it during the physical exercises. (Authors’ translation) (Louise) I have a daughter who, when she calls, I usually jump, and it seemed like every time she called, I was on with [Trainer’s name]. And it was annoying to her and my sisters. I’d tell them “Don’t call me at 1:00” or whatever, but they just called every time they needed me. (Lisa)
Discussion
The SYNERGIC@Home RCT experienced a high retention and compliance rate, which seems to be typical for the population and physical exercises involved.4,17,18 The present qualitative study focused on the experience of participants who completed the remotely delivered cognitive and physical exercises in this feasibility trial. We explored participant experience through a grounded theory qualitative study and found that it was the establishment of meaningful connections to the study that facilitated their journey through study completion. The resulting grounded theory and participant-identified conditions facilitating participation expand the existing literature, which is currently limited for the at-risk population, multimodal intervention, and remote participation being considered in this study. Examining participant experience is critical to understanding feasibility, efficacy, and challenges in RCT, but this is not systematically investigated or reported. 19 In particular, the present findings could inform future remotely delivered programs in attaining higher engagement and retention.
Study Goal as Motivation
While the specific aim of the SYNERGIC@Home study was to measure the feasibility of a remotely delivered ADRD preventative intervention, participants deeply connected with a broader goal of preventing ADRD. Most interviewees who were personally touched by the disease felt motivated to participate to benefit themselves, their loved ones, and society at large. A sense of social responsibility supports participant engagement and continuation in research, even when it is understood that the individual participant may not benefit directly from the research. 20 This finding has important practical implications. It suggests that by nurturing a sense of ownership and personal connection with study goals, clinicians and researchers could help promote recruitment, retention, and satisfaction. In practice, the co-design of study goals in collaboration with potential participants could help promote these and other outcomes of relevance to participants, consistent with the rationale underlying patient engagement in the design of clinical trials. 21 Further, participants valued their role in participating in a study examining the feasibility of completing interventions that are home-based and virtual, as an approach to maintaining support for older adults during COVID-19 pandemic restrictions and afterwards. This finding is unique to our study as far as authors are aware and a phenomenon that warrants further study. In the context of a cohort study, others found that wanting to make a contribution was one of the main themes underlying participants’ attitudes towards participation. 22
Study Protocol as a Facilitator of Participation and Enjoyment
The study protocol, specifically the personalized nature and schedule of exercise and cognitive intervention, were described favorably by participants. While some participants found the repetitive nature of the cognitive intervention monotonous, others enjoyed the routine and challenge of beating prior sessions’ performance. Mixed reactions to cognitive exercises should be investigated further to address monotony and sustain engagement for diverse participants. Approaches involving potential participants in designing and implementing the intervention would be critical in helping improve the cognitive stream of the program to make it more attractive and engaging. To our knowledge, the co-creation of cognitive interventions with older adults at risk of dementia has not been reported and should be considered. Co-creation methods such as community-based participatory research (CBPR) ensure that interventions are tailored to the target group by incorporating their insights and preferences and facilitate implementation.23,24 Likewise, the exercise program design can influence motivation to complete intervention. 5 When discussing the physical exercise intervention, participants described being motivated to learn about its importance to physical and brain health and ways to incorporate it into their lifestyle, though it was not clear to all participants whether they experienced any change because of the program. They also appreciated the frequency and length of the sessions, contrary to what Jansen et al. 5 found in an exercise intervention delivered by an Alexa device, suggesting that personalization and one-on-one support are key factors to older adults’ satisfaction with combined cognitive and physical exercise interventions. The practicality of delivering such personalized interventions on a larger scale should be examined further in future studies to assess the potential benefits for diverse participants at risk of dementia. In practice, given potential resource constraints, it may be advantageous to offer the proposed interventions in priority to high-risk people or people living in remote locations, pending demonstration of positive effects on cognitive function and/or mobility by longitudinal follow-up studies. In our work, real-time interactions with their assigned exercise trainer stood out as an important facilitator. The convenience of remote visits was brought up by several participants and may have been influenced by various factors. Firstly, most participants (13/15) in the qualitative study were retired, making it possible to have the time to join, and this was observed by others as well. 18 Secondly, the study took place well into the COVID-19 pandemic restriction measures, when, like many, participants had to learn to communicate and conduct business and social visits through virtual conference media.
People
Study personnel and participant family and friends played an important role in study participation and adherence, as described by participants. The personalized nature of the intervention likely promoted participation, consistent with previous reports,5,17,18 as many participants described the accountability and supportive relationship with the trainers in their narratives, which helped to increase enjoyment, overcome technical and other challenges, and encourage behavioral modification. The importance of quality interpersonal connections evidenced in our study supports the recommendations made by Modic et al. 25 for creating relationship-centered care during virtual visits. Further, support from family, as well as having a family history of dementia, reinforced participant motivation to complete study interventions. The proposed grounded theory underscores the importance of study staff and participants’ relatives in establishing a supportive environment that facilitated engagement and completion of the 16-week program. This form of social support should not be underestimated as it probably contributes health-promoting effects other than those expected from physical exercise and cognitive training.
Technology
While participants in our study did not find technology a barrier to continued participation, this may have been a result of a combination of internal and external factors to the study. Firstly, inclusion criteria necessitated that participants have access to their own device for remote intervention, which resulted in a sample demographic that was more likely to be familiar with technology, especially during the COVID-19 pandemic restrictions imposed during the period of the study. 26 The self-selecting nature of participants is another factor that could have influenced their digital literacy level. Second, enjoyment of interventions and support from staff when technological difficulties were faced may have facilitated working past the technological challenges.4,26 Finally, participants’ description of their experience with technology suggested they looked beyond the inconvenience of a temporary glitch and viewed technology as an important vehicle for facilitating access for older adults who may not otherwise have an opportunity to access research. This view may have resulted partially from the sense of ownership participants expressed in describing their study experience. This attitude may be fostered through a CBPR approach by designing future programs with this population. 24 While most of the reported challenges with technology were directly related to technology itself, some participants described health-related challenges such as back pain that required specific adjustments facilitated by study staff. While it is not clear how specific technology challenges influenced participation, a salient finding was that they were not experienced as a major hurdle, possibly because participants perceived greater benefits from engaging in the study.
Strengths and Limitations
Study design, participant recruitment, data collection, and analysis followed rigorous criteria. While sample size was typical of grounded theory research, it consisted predominantly of women, and it did not include participants who dropped out of the RCT before completing the 16-week interventions, which may have uncovered additional learnings. In addition, several RCT inclusion criteria such as living in own residence, language fluency, and having access to own computer and internet limit the diversity of respondents. Moreover, the self-selecting nature of study participation means that participants’ views may not reflect those of individuals who dropped out or did not volunteer to take part in the study. Individuals who withdrew or chose not to be interviewed may have different, potentially more critical perspectives, which could inform improvement of the cognitive and physical exercise program to make it more engaging and accessible. As mentioned above, most participants were retired and had exposure to using online communication platforms prior to participating in the study by virtue of social distancing protocols during the COVID-19 pandemic. Thus, the present findings should be viewed primarily within the scope of older adults who have the luxury of time and a basic level of digital literacy. Further research will be required not only to establish the effectiveness of the interventions but also to examine how it could benefit more diverse participants at risk of dementia. Scalability of the person-centered, personalized interventions will require specific consideration given potential resource constraints.
Conclusion
The proposed grounded theory offers valuable insights into how older adults at risk for dementia engage in and experience interventions where videoconferencing enables personalized physical exercise and cognitive training from home. By identifying with the study's goals on a personal level and building relationships with exercise trainers who personalized their intervention, participants not only adhered to the study until completion but also transferred learning to other aspects of their life outside the study. Overall, findings suggest that a person-centered approach was key to nurturing meaningful connections between participants and the study. Learnings from participants’ experiences in this study can inform the design, implementation, and scaling up of remotely delivered physical exercise and cognitive training programs in older adults. In developing interventions remotely, as researchers and clinicians alike increasingly rely on videoconferencing technology, it is important to examine and further understand how interpersonal connections facilitate positive and productive experiences.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251392324 - Supplemental material for “It's About Connections”: A Grounded Theory of Older Adults’ Engagement in Remotely Delivered Home-Based Physical and Cognitive Exercise Interventions Aiming to Reduce the Risk of Dementia
Supplemental material, sj-docx-1-jpx-10.1177_23743735251392324 for “It's About Connections”: A Grounded Theory of Older Adults’ Engagement in Remotely Delivered Home-Based Physical and Cognitive Exercise Interventions Aiming to Reduce the Risk of Dementia by Hanin Omar, Linda Yetman, Carole C. Tranchant, Molly Gallibois, Josée C Haché, Karla Faig, Grant Handrigan, Chris McGibbon and Pamela Jarrett in Journal of Patient Experience
Footnotes
Acknowledgements
The authors are grateful to the participants who took part in this study. They acknowledge the in-kind contributions of the Canadian Consortium on Neurodegeneration in Aging, which received funding from the Canadian Institutes of Health Research, with additional funding from several partners, including the Alzheimer's Society of Canada.
Ethical Approval
This study was approved by the Research Ethics Boards of Horizon Health Network (file number 2020-2954), Réseau de santé Vitalité (2020-35), University of New Brunswick (2020-168), and Université de Moncton (2021-049). All the procedures were conducted in accordance with the protocol approved by these boards. The manuscript conforms to the COREQ Research Reporting Guidelines for qualitative studies (Tong et al., 2007).
Authors Contributions
LY, HO, CCT, MG, and JH conceptualized the grounded theory study, collected, and analyzed the data. All the authors contributed to the larger RCT, co-led by CMG and PJ and coordinated by MG, and they advised with the design of the present study and interpretation of the results. The first draft of the manuscript was prepared by HO, CCT, and LY, and all authors commented on subsequent versions. All authors reviewed and approved the final manuscript.
Funding
The study received funding from the New Brunswick Healthy Seniors Pilot Project and the Public Health Agency of Canada (funding application C0042). PJ received funding from ResearchNB through a Clinical Research Scholarship. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Informed Consent
Participants provided written informed consent to participate in the study and for their anonymized information to be published.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.