
Abstract
Tribal communities face barriers to care. This is especially true for American Indian Alaskan Native children needing pediatric-subspecialty care. We created a new pediatric rheumatology hybrid clinic using telemedicine to enhance access. A combination of telemedicine clinics and face-to-face clinics onsite at the Northern Navajo Medical Center was offered. The new clinic reduced the wait time for care for pediatric rheumatology conditions by 95%.
Introduction
The Indian Health Service (IHS) is a United States Federal Agency within the Department of Health and Human Services charged with providing healthcare services to tribal communities. Healthcare is to be delivered based on respect, tribal consultation, and honor of native identity. Health inequities in tribal communities have been well documented. 1
Overall life expectancy for American Indian Alaskan Native (AIAN) adults is up to 13 years shorter than that of the U.S. Caucasian population. 2 Factors that influence the health of AIAN communities include: food insecurity, limited access to health insurance, multigenerational historical trauma, medical mistrust, exposure to violence, and chronic disease. 3 AIAN communities have greater mortality rates due to diabetes (207%), suicide (64%), and pneumonia and flu (50%). 4 The top factors for years-of-potential-life-lost among the AIAN population include unintentional injuries, COVID-19, liver disease, suicide, heart disease, and cancer. 4 In 2020, infant mortality was 60% higher for AIAN populations than the overall U.S. population. 3 AIAN people have worse access to care than other populations. 5 Barriers to care due to long travel distances are common in tribal communities. IHS has ongoing difficulties with retaining and recruiting staff at its facilities, especially in remote locations. Vacancy rates are highest for nurses, physicians, and dentists. 6
Timely access to care is one aspect of health inequity. An opportunity to improve care within tribal communities is to enhance access for AIAN children to pediatric subspecialty care. AIAN communities have a higher prevalence of autoimmune conditions, such as rheumatoid arthritis, systemic lupus erythematosus, Sjogren's syndrome, connective tissue diseases, and spondylarthropathies, compared to other populations, and have worse outcomes.7–10 AIAN adults have 10 times higher prevalence of rheumatoid arthritis. One study estimates the prevalence of juvenile ididopathic arthritis (JIA) in the U.S. general population of 57 per 100,000, 11 compared to AIAN children, who have an estimated prevalence of JIA of 79 per 100,000. 12
The largest Federal Indian reservation is the 16 million-acre Navajo Reservation spanning across Arizona, New Mexico, and Utah. The Shiprock Service Unit (SRSU) serves the Northern Navajo population. The social determinants of health that impact the area include unemployment, lack of transportation, limited access to fresh food and water, social isolation, and limited access to reliable broadband. The Northern Navajo Medical Center (NNMC) is located in Shiprock, New Mexico (see Figure 1). It provides inpatient care (60 beds), intensive care, labor and delivery, emergency and urgent care, ambulatory services, mental health services, optometry, dental services, traditional medicine, and disease prevention, along with x-rays, computed tomography scans, physical and occupational therapy, laboratory services, and pharmacy services. Primary care services include general pediatrics and family medicine.

View from Northern Navajo Medical Center, Shiprock, New Mexico.
Methods and Process
In December 2023, we started the first subspecialty pediatric service as a hybrid clinic offering telemedicine and face-to-face visits at NNMC. The hybrid pediatric rheumatology service featured monthly telemedicine clinics (11 4-h telemedicine clinics) and bi-annual face-to-face clinics (2 8-h in person clinics) in 2024. There was a total of 60 h of clinic time available for the year. There were 44 h of telemedicine clinics and 16 h of in-person clinic, making a telemedicine: in-person clinic ratio of 2.75:1. The pediatric rheumatologist lived in the mid-Atlantic region, 2100 miles from the medical center. The primary care physicians from general pediatrics and family medicine at NNMC made referrals to pediatric rheumatology. There were no restrictions or criteria for referral to telemedicine. Patients were scheduled in the next opening for pediatric rheumatology, regardless of telemedicine versus on-site location. For telemedicine visits, AA ring software was used. Encounter documentation was created using the NNMC electronic health record. The physician completed training in cultural humility, tribal context, trauma-informed care, and historical trauma.
Data on pediatric referral wait time from 2019 to 2024 were analyzed from the medical records at NNMC.
Results
The wait time range for 2019–2023 (n = 15 patients), before the presence of an in-house pediatric rheumatologist, was 3–386 days with a mean wait time of 114.2 days. Pediatric patients needing subspecialty care could travel 3–8 h away by vehicle. In the practice's first year (2024), there were 9 referrals. Six referrals were seen via telemedicine. Three referrals were seen face-to-face. Three patients were seen in follow-up (both via telemedicine and in the clinic) for management of arthritis. Six patients were returned to primary care for management of nonrheumatologic conditions (see Figure 2).
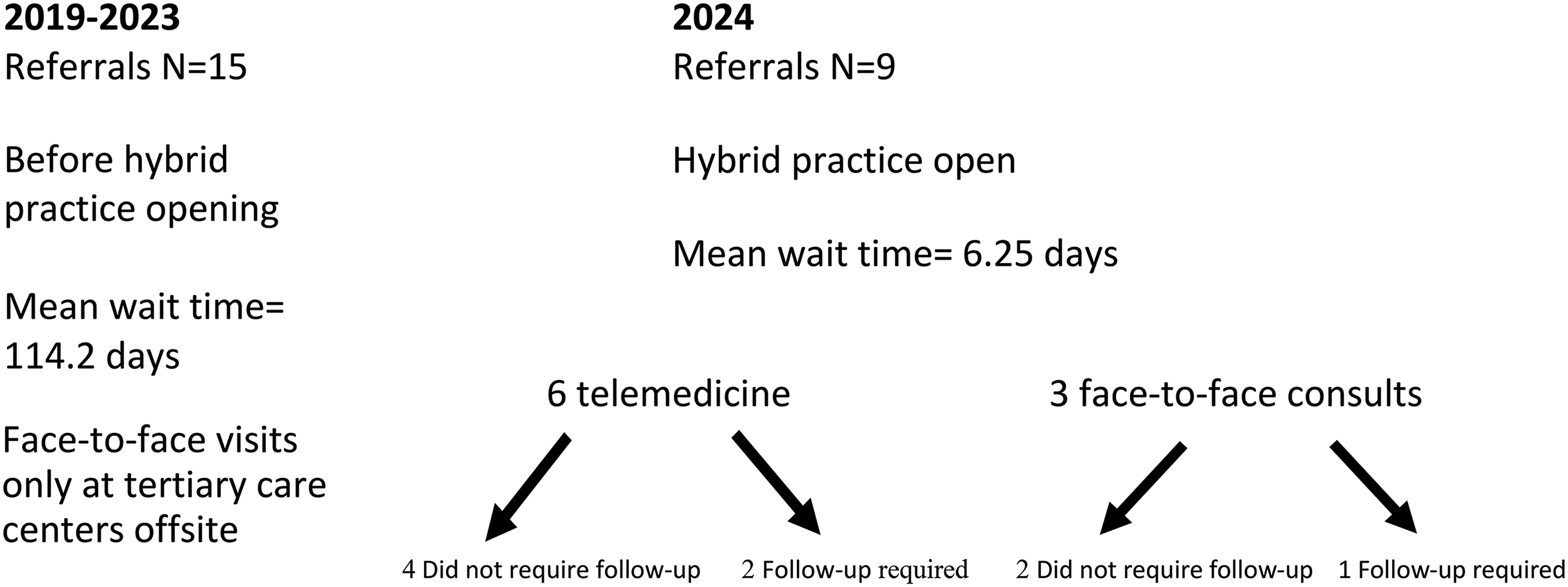
Pediatric rheumatology referrals from the Northern Navajo Medical Center 2019–2024.
Opening a new pediatric subspecialty hybrid telemedicine clinic reduced patient wait time (by 95%) from a mean of 114.2 days (2019–2023) to a mean of 6.25 days (2024) (range 1–22 days).
Discussion
We introduced a pediatric rheumatology hybrid clinic using a mix of telemedicine visits and face-to-face visits to address barriers to patient access. This enabled shorter wait times for subspecialty care with limited travel burden on the family and on the physician. Rheumatology services are important to provide to AIAN communities, as diseases of the musculoskeletal system and connective tissues are the leading cause of ambulatory medical visits among IHS patients. Because AIAN populations carry a greater burden of autoimmune diseases, patients should have access to adult rheumatology and pediatric rheumatology services.
In pediatric rheumatology, it is estimated that 1 pediatric rheumatologist is needed to provide services for a population of 1 million people. The IHS eligible service population is estimated to be 2.7 million people. Approximately 3 full-time pediatric rheumatologists would be needed to address the needs of the entire pediatric AIAN population. Telemedicine could increase access to remote areas and stretch the impact of a single specialist. This model could be replicated for other pediatric subspecialties. Based on our experience, we feel that the pediatric rheumatology hybrid model could be expanded to other tribal communities. In addition, this model could be piloted across the pediatric subspecialties (ie, pediatric developmental medicine, pediatric neurology, and pediatric endocrinology) to provide access to subspecialized care for AIAN children. Pediatric specialists who would like to make a positive impact on the lives of AIAN children, but are hesitant to frequently travel long distances may find this kind of hybrid model effective. We piloted a ratio of 2.75 telemedicine hours for every in-person clinic hour. Other clinicians may find other ratios more effective. Clinicians should be aware that each tribe has its own accreditation process, so that accreditation at one tribal facility does not cross over to other tribal facilities.
Any intervention should be planned in partnership with local tribal communities. This includes consultation with tribal leaders, healthcare administrators, and local patients and families. Services should be trauma-informed and culturally appropriate. 1 Indigenous ways of knowing and traditional healing practices are to be respected. Setting up a hybrid clinic in the SRSU was challenging due to the unreliable internet available. Many families had to drive from their homes on the reservation to the medical center to access the hospital's Wi-Fi. While the travel time could be an hour or longer, this was still easier than driving to the surrounding tertiary care centers. A telemedicine visit could be supplemented with an in-person visit as needed. In this limited experience, work-up and diagnosis could be made via telemedicine, with the option of in-person consultation as needed. There were technological challenges in setting up a de novo telemedicine practice. This included a range of issues from securing equipment, building the correct back-end referral workflows, and accessing the help desk.
Limitations
This was a retrospective look at the impact on patient access after a new subspecialist was introduced to an IHS Medical Center. We were not able to control for variables such as referral patterns, family preferences, or clinical care pre- versus post-COVID-19 pandemic. The intervention was limited to just 1 year of the specialist's presence in the clinic. In the first year, it took time for referring physicians to become aware of the availability of the consultant. In addition, families needed education on the availability of a new specialist and a new telemedicine service. This study did not formally collect patient experience data. An area of future study would be to collect quantitative patient satisfaction data about the hybrid model.
Conclusions
Using telemedicine can expand access and reduce wait times for AIAN communities (see Media 1). In pediatric rheumatology, early diagnosis and treatment are essential to avoid long-term complications from autoimmune diseases. This hybrid model could expand access to other pediatric subspecialties and enhance care for AIAN children. We were able to reduce the wait time for pediatric rheumatology care by 95% with our telemedicine hybrid model. A hybrid telemedicine pediatric subspecialty model is a viable option to reach rural tribal communities.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251383594 - Supplemental material for Enhancing Access to Pediatric Subspecialty Care for American Indian Alaskan Native Children
Supplemental material, sj-docx-1-jpx-10.1177_23743735251383594 for Enhancing Access to Pediatric Subspecialty Care for American Indian Alaskan Native Children by Tommie Begay, Loeretta Christensen and Paul Rosen in Journal of Patient Experience
Footnotes
Author Contributions
Tommie Begay, Loretta Christensen, and Paul Rosen conceptualized and designed the study, drafted the initial manuscript, and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not applicable to this article
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Informed consent for patient information to be published in this article was not obtained because there is no patient information in this article.
Statement of Human and Animal Rights
This study is not human subject research. This study contains no animal subjects.
Supplemental Material
All supplemental material mentioned in the text is available in the online version of the journal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.