
Abstract
Telehealth tools can enhance health-related information access and self-management for individuals with multiple sclerosis (MS). However, successful integration of telehealth services depends on acceptance by individuals with MS, which is influenced by their Technology Readiness Level. A 2-part questionnaire was administered: demographic information and the readiness level to use telehealth services based on the Technology Readiness Index (TRI 2.0) with 4 scales of optimism, innovativeness, insecurity, and discomfort. Data from 120 participants were analyzed using descriptive and inferential statistics. The mean readiness score was 3.266 (SD = 0.421, P < .01), optimism 3.633 (SD = 0.790, P < .01), and innovativeness 3.273 (SD = 0.699, P < .01), all significantly above the midpoint. However, insecurity (M = 3.031, SD = 0.608, P = .574) and discomfort (M = 3.127, SD = 0.773, P = .074) were not significant. No significant associations were found between readiness and demographic or disease-related factors (P > .05). Given the benefits of telehealth tools in MS care, it is crucial to implement targeted interventions to enhance readiness and engagement in telehealth adoption.
Introduction
Multiple sclerosis (MS) 1 is a chronic autoimmune disease of the CNS, leading to various motor, visual, cognitive, and sensory symptoms, as well as fatigue. The onset of MS is typically between 20 and 40 years of age, and women are more frequently affected than men. 2 Globally, approximately 2.5 million people worldwide suffer from MS. 3 Iran has consistently reported the highest incidence of MS in the region, with the rate rising from 51.9 per 100 000 in 2010 to 148.06 per 100 000 in 2017. Tehran, the capital of Iran, is among the regions with the highest MS prevalence in Asia (184.88 per 100 000 in 2019). 4
Despite the unknown etiology and lack of a definitive cure for MS, self-management remains essential in disease control. 5 Telehealth, as a key component of digital health, has been shown to enhance treatment adherence, self-management skills, psychological support, and fatigue management in individuals with MS.2,6–8 Several mHealth interventions empower individuals with MS by enhancing self-management and reducing dependence on direct consultations. 9 These self-guided tools help manage fatigue, depression, and cognitive impairments. Systematic reviews confirm their effectiveness, particularly through CBT-based digital programs. 9 One of the advantages of telehealth is its ability to integrate multiple digital tools for remote monitoring of mobility in individuals with MS. For instance, open-access digital applications such as Google Maps Timeline have shown potential in tracking real-world walking activities, offering a cost-effective alternative to traditional clinical assessments. 10 Telehealth facilitates patient-provider interactions, from basic consultations to more advanced interventions, using digital platforms. 11 According to the definition of the World Health Organization, telehealth means the provision of healthcare services when distance is a critical factor by professionals who use information and communication technology (ICT) to exchange credible information for the diagnosis, treatment, and prevention of diseases, as well as for research and continuous education of specialists 12 In general, telehealth is a combination of convenience, low cost, and convenient access to health information and communication using the Internet and relevant technologies. 13
Telehealth tools help improve convenient access to physicians, thereby controlling the symptoms, disseminating accurate information about the disease, and remotely managing the exercise of people with individuals with neurological conditions. 14 In addition to individual disabilities, there are other barriers that make face-to-face visits more challenging for individuals with MS, including long distances from specialists, especially in rural areas, and certain crises such as the recent COVID-19 pandemic that complicate care for individuals with MS.1,9 Telehealth overcomes geographical barriers, ensuring timely and high-quality healthcare delivery for individuals with MS.1,15–17
Many individuals with MS experience cognitive, sensory, or physical problems that may hinder their use of certain telehealth tools. 18 Furthermore, the perspectives of people and healthcare professionals in different communities about these solutions are one of the most important issues to consider. Evidently, successful provision of any care, including telehealth, highly depends on the expectations, satisfaction, and acceptance of people and healthcare providers.19,20 Many studies have provided evidence that individual acceptance of new technologies depends on the technology readiness level (TRL). Technology readiness reflects an individual's willingness to adopt new technologies, shaped by both positive (optimism, innovativeness) and negative (discomfort, insecurity) factors. Higher TRL is associated with greater adoption of digital solutions, while lower TRL may lead to resistance. Since TRL influences technology acceptance, assessing it can help predict engagement with telehealth tools. 21
Given the benefits of telehealth tools for individuals with MS, it is essential to conduct comprehensive studies on these opinions of individuals with MS, readiness level, level of use, and expectations. Various factors, including social, economic, motivational, political, and even geographic characteristics, can influence the readiness to use telehealth services. As there has been no similar research in Iran, the results of the current study can fill the gap in the literature by answering the following question: What is the readiness level to use telehealth services for MS care among individuals with MS and the relationship between demographic factors and the disease on this readiness level? The findings can help medical informatics experts to help provide and build better user-oriented telehealth services and products to improve the quality of life and comfort of individuals with MS during treatment.
Materials and Methods
This was a descriptive cross-sectional study. This study adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for the reporting of cross-sectional studies. As the research was conducted anonymously, autonomously, and voluntarily using an online questionnaire, there was no intervention, no deception, and no potentially undesirable or burdensome questions or tests. Ethical approval was obtained from the relevant institutional ethics committee***. No monetary compensation was provided to the participants. The participants had to declare that they met the inclusion criteria before completing the questionnaire. They were also informed about the study objectives and provided informed consent by selecting the option “I agree.” It was not possible to check whether the respondents completed the electronic questionnaire more than once since IP tracking was not enabled to protect their anonymity.
Participants and Data Collection
The participants were all individuals with MS who had visited a referral MS clinic in Tehran during 6 months (from October 2022 to March 2023). They could complete online or paper-based surveys. The web-based questionnaire was developed using the Porsline platform and sent to participants via text messages, WhatsApp, and Telegram. Paper-based questionnaires were distributed in-person at the clinic. Responses from online and paper-based questionnaires were pooled without weighting or subgroup analysis, as preliminary testing revealed no significant differences between administration methods (P > .05). This approach aligns with standard practices for Technology Readiness Index (TRI 2.0) validation studies. If participants were unable to complete the questionnaire due to low education level or illness or needed help, the researcher would read the questions to the participant and complete the questionnaire based on their responses. The sample size was determined based on a convenience sampling approach, considering the accessibility of participants within the study time frame. Given the lack of similar studies in Iran, a sample of 120 participants was deemed sufficient for descriptive analysis. Following TRI 2.0 validation protocols, 22 our sample of 120 participants exceeds the threshold (n = 100-150) required for reliable psychometric evaluation.
Instrument
The TRI 2.0 developed by Parasuraman and Colby 22 was administered. The TRI 2.0 is a validated index assessing the drivers and inhibitors of technology readiness, including telehealth services. The TRI 2.0 was first translated into Persian, and experts in medical sciences and English language and literature approved the translation. Then, to check cross-cultural reliability, the Persian version was backtranslated into English and compared with the original version by a bilingual expert. Twelve experts evaluated the index's content validity. The minimum acceptable CVR according to Lawshe's formula is 0.56. 23 The average CVR of the index was 83% and was estimated to be highly optimal. To determine its reliability, 30 people were selected from the statistical population, and the index was administered to them; then, Cronbach's alpha was used to determine reliability. A Cronbach's alpha of 0.83, which was higher than 0.7, indicated the acceptable reliability.
The questionnaire used in this study included 2 parts and 26 questions. The first part involved 10 questions about demographics and disease status (sex, age, marital status, occupation status, education level, type of MS, duration of MS, level of mobility, 24 disease symptoms, 25 and the impact of MS on people). Sixteen questions of the second part, based on the TRI 2.0, tapped into 4 dimensions of technology readiness, that is, optimism and innovativeness as drivers and insecurity and discomfort as inhibitors (4 items per dimension). The items of this index are answered on a 5-point Likert scale (from completely agree to completely disagree).
Statistical Analyses
Descriptive and inferential statistics were used to analyze the data. At the descriptive level, frequency and percentage tables were used, and at the inferential level, t tests and analysis of variance (ANOVA) were performed. Before analysis, the assumption of normal distribution of the quantitative variables was confirmed by the nonparametric Shapiro-Wilk test. To test the individuals with MS’ readiness to use telehealth services, we used the t test. This statistical test compared the mean readiness score of participants against a predetermined value of 3. Analysis of variance was used to test the relationship between the variables. The answers to the questions about optimism, innovativeness, insecurity, and discomfort were scored from 1 to 5 (1 = completely disagree, and 5 = completely agree). To calculate the final score of readiness, the reverse scoring method was used for 8 items of insecurity and discomfort, so that a score of 5 was assigned to completely disagree and a score of 1 to completely agree. Given the descriptive cross-sectional nature of this study, statistical adjustments for potential confounders such as socioeconomic status and disease severity were not performed. While these factors may influence telehealth readiness, our study aimed to provide an initial exploration of the overall readiness level rather than establishing causal relationships. Future research utilizing analytical methodologies, such as multivariate regression or propensity score matching, is recommended to further delineate the impact of these variables and strengthen causal inferences. For all statistical tests, a confidence level of 95% and an acceptable margin of error of 5% were considered. All preprocessing and statistical analyses were performed in SPSS 26 and Microsoft Excel 2020. No missing data were observed, as all participants completed the questionnaire entirely. Therefore, no data imputation or deletion techniques were required.
Results
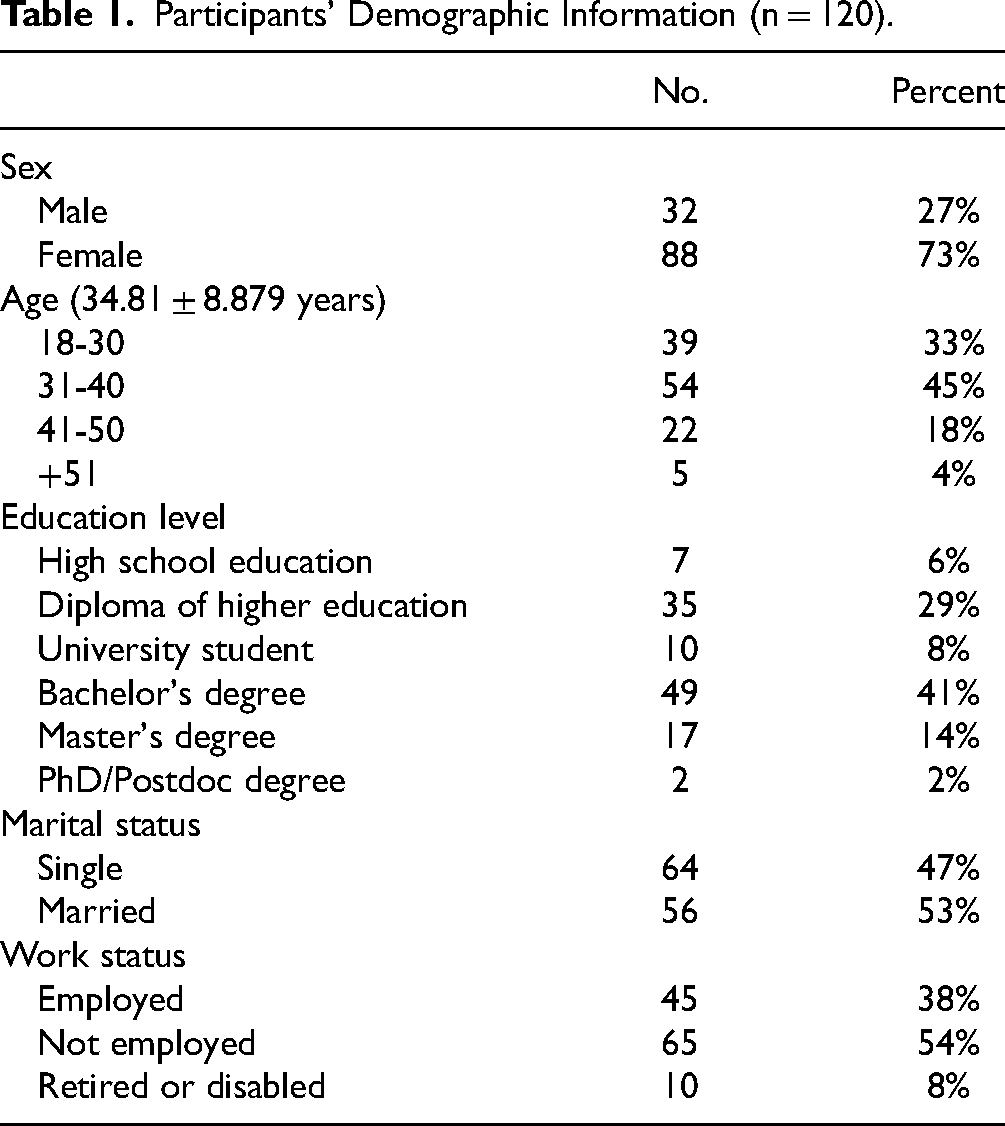
A total of 120 individuals with MS participated. No age limit was set when enrolling people (mean age: 34.81 ± 8.88 years). Moreover, 72% (87 out of 120) of the questionnaires were collected electronically and 28% (33 out of 120) were collected manually. The findings obtained by the 2 administration methods did not differ significantly (P > .05). Most of participants were female (73%), married (53%), with the age range of 31 to 40 years (45%), and had a bachelor's degree (41%). The demographic information of the participants is presented in Table 1.
Participants’ Demographic Information (n = 120).
Fifty percent (50%) of participants (60 out of 120) had relapsing-remitting MS. For 34% (41 out of 120) of the individuals with MS, more than 10 years had passed since their diagnosis. Besides, 46% (55 out of 120) of the participants reported that their MS had not impacted their ability to walk, and 33% (40 out of 120) stated that the disease had impacted them but they could still walk independently. More than half of the participants (63%, 75 out of 120) noted that among the common symptoms of MS, fatigue had the greatest impact on their lives, and 30% (36 out of 120) reported that the disease had no impact on their lives. Table 2 lists the information about the participants’ disease status.
The Participants’ Disease Status (n = 120).

The number, percentage, and mean of answers to questions related to the individuals with MS’ readiness to use telehealth are listed in Table 3. The mean scores of all questions related to optimism were higher than 3. The highest mean score (3.74 ± 0.87) related to the item “Telehealth services help people have more control over their daily lives” for optimism. The lowest mean score (2.72 ± 0.95) belonged to the item “When I receive technical support services from a provider of high-tech health products or services, I sometimes feel that someone who knows more than me is taking advantage of me” for discomfort. Participants’ responses to TRI 2.0 items are detailed in Table 3.
Means of Items About the Individuals With MS’ Readiness to Use Telehealth Services.

The mean scores of readiness to use telehealth services, optimism, innovativeness, insecurity and discomfort were 3.266, 3.633, 3.273, 3.031, and 3.127, respectively. The results of the one-sample t test revealed that the mean value of readiness to use telehealth services was above 3 and significant (P < .01). For the subscales related to the readiness to use telehealth services, the mean level of optimism and innovativeness was higher than 3 and significant (P < .01). Nevertheless, the mean of the subscales of insecurity and discomfort was at a moderate level (P > .05). Statistical comparisons of readiness dimensions are presented in Table 4. See Figure 1 for a visual summary of the TRI subscale means:

Mean scores of the 4 Technology Readiness Index (TRI 2.0) subscales among individuals with multiple sclerosis (MS).
Results of One-Sample T Test.

** Significant at .01 level.
Supplementary1 Table (S1 Table) presents the effect of age, sex, marital status, education level, employment status, type of disease, duration of the disease, and mobility on people's readiness level to use telehealth. Based on the ANOVA results, none of the investigated variables affected the individuals with MS’ readiness level to use telehealth (P > .05). See S1 Table for additional statistical analysis.
Discussion
This study examined readiness to use telehealth services among individuals with MS. It also assessed how demographic and disease-related factors influence this readiness. The standard TRI 2.0 was administered to measure the readiness level of individuals with MS.
The mean scores for optimism and innovativeness were above 3 and statistically significant, while the average scores for insecurity and discomfort were above 3 but not statistically significant. Therefore, individuals with MS demonstrated a somewhat positive view of telehealth tools in the dimensions of optimism and innovativeness, which act as drivers of technology readiness. However, the dimensions of insecurity and discomfort regarding telehealth tools, which act as inhibitors of technology readiness, were at a moderate level. Overall, the participants’ readiness level to use telehealth services was slightly higher than mean significantly. As other studies have suggested,18,26 increasing the readiness level of individuals with MS requires planning for user-oriented designs suited to their different needs, as well as education and information to increase various aspects of optimism and innovativeness and reduce insecurity and discomfort.
Our findings revealed that age, sex, marital status, education level, employment status, type of disease, duration of the disease, and mobility did not affect their readiness level to use telehealth services, and all the investigated groups had an acceptable level of readiness to use these services. One possible explanation for the lack of significant demographic or disease-related predictors is the relatively uniform familiarity with telehealth concepts across the studied population. The Iranian context—especially during the COVID-19 era—saw a rapid expansion in digital communication platforms and health-related messaging. Public campaigns, increased smartphone usage, and greater reliance on online services may have collectively contributed to reducing variation in telehealth readiness across different demographic subgroups. Furthermore, centralized healthcare service structures and similar access channels across socioeconomic groups in urban areas may have led to more consistent user experiences. This finding aligns with expectations, given the widespread media coverage and the obvious benefits of telehealth tools during the COVID-19 pandemic. 27 While prior research in high-income countries 6 has identified demographic factors like age and education as significant predictors of telehealth adoption, our study in the Iranian context reveals no such associations. This divergence may reflect post-pandemic normalization of digital health technologies across all demographic groups. Importantly, our findings contrast with Western studies 17 that report higher readiness among younger, more educated populations, suggesting that global health crises may have accelerated technology acceptance uniformly. However, the moderate scores in insecurity and discomfort dimensions highlight persistent barriers that require culturally adapted solutions, particularly in regions with infrastructure limitations like Iran. The effectiveness of treatment programs for individuals with MS aimed at controlling symptoms and complications and delaying the progression of the disease depends on patient participation in self-management. 28 Furthermore, different studies have shown that the use of telehealth tools such as applications can help increase the health-related information and self-management capacity of individuals with MS and can help prevent disease progression.5,18 Given the readiness level to use telehealth tools in different groups of this population and the current need for telehealth and home monitoring devices, healthcare institutions should provide different telehealth tools for physical, social, and psychological support of individuals with MS.
Our findings suggest a stratified implementation approach: (1) patients with high optimism scores (M = 3.633) should be prioritized for immediate telehealth adoption, while those with elevated discomfort (M = 3.127) require preparatory technical training; (2) interface designs must accommodate the 63% reporting fatigue (Table 2) through simplified navigation and voice-command features to reduce cognitive load.
To further enhance patients’ readiness and willingness to use telehealth tools, several interventions can be implemented. Engaging individuals with MS and healthcare providers in the user-centered design of telehealth tools ensures that these solutions align with their specific needs. Additionally, comprehensive educational programs can help inform patients about the benefits and functionalities of these services, addressing common concerns and reducing insecurity. Establishing peer support networks and incorporating feedback mechanisms for continuous improvement can further encourage engagement. Moreover, integrating telehealth into existing care frameworks can facilitate adoption and routine use. Implementing these interventions can enhance patients’ confidence and comfort with telehealth, ultimately improving their self-management and health outcomes. Individuals with MS and healthcare providers should also be involved in the development of new telehealth tools to ensure that the final product meets their needs.
Limitations
There were limitations in this study that should be kept in mind when interpreting the results. First, this was a cross-sectional analytical study; at the time of data collection in Iran, there were restrictions on Internet bandwidth due to political reasons, which may have affected the users’ opinions about the readiness to use telehealth tools. Therefore, the results should be interpreted with caution. Second, while this study provides valuable insights into the telehealth readiness of individuals with MS, it is important to acknowledge that data were collected from a single referral MS clinic in Tehran. Although this setting allowed for a focused and in-depth analysis, the findings may not fully capture the diversity of experiences across the broader MS population, particularly those in rural areas or with varying levels of healthcare accessibility. To enhance generalizability, future research should incorporate multicenter studies with more heterogeneous populations, ensuring a more comprehensive understanding of telehealth adoption among individuals with MS. Third, although content validity was assessed by experts, face validity was not tested directly with individuals with MS. This means we did not assess how understandable or relevant the items were from the participants’ perspective, which may affect the interpretability and contextual relevance of the instrument in this population. Future studies should include cognitive interviews or pilot testing with target users to improve face validity.
Conclusion
To promote the acceptance of health tools among individuals with MS, technology and service must be in line with their actual demands; therefore, the weaknesses and strengths inherent in the use of health tools in reference to users and their needs must be taken into account. The present study provides theoretical understanding of the readiness level of individuals with MS to use health tools, demonstrating that their readiness is slightly higher than average. Three actionable recommendations emerge from our findings: (1) tiered training programs addressing technical discomfort (M = 3.127) for patients with lower innovativeness scores (M = 3.273), (2) fatigue-optimized interface designs for the 63% reporting fatigue as a primary symptom, and (3) prioritized device distribution for the 46% with mobility limitations (Table 2). These interventions directly respond to the identified readiness profile while aligning with Iran's healthcare infrastructure needs. Self-management is crucial for these individuals with MS and requires receiving information from reliable sources; telehealth tools also have unique potentials for sending high-quality and timely information. Thus, necessary interventions to improve and facilitate individuals’ readiness to use these tools should be administered. Healthcare officials and policy-makers should plan to invest more in providing telehealth tools with the development of ICT infrastructure according to the readiness level and specific conditions of individuals with MS.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251383247 - Supplemental material for Examining the Telehealth Readiness Among Individuals With Multiple Sclerosis
Supplemental material, sj-docx-1-jpx-10.1177_23743735251383247 for Examining the Telehealth Readiness Among Individuals With Multiple Sclerosis by Farnaz Zare, Rezvan Rahimi, Hanieh Zehtab Hashemi, Leila Faghani, GholamHosein Ghaedi and Seyed Massood Nabavi in Journal of Patient Experience
Footnotes
Acknowledgments
The authors express their gratitude to the patients who participated in this study.
Author Contributions
The study was designed by RR, FZ, HZH, and SMN. Data collection was carried out by FZ and LF. Analysis of the data was performed by RR, HZH, and GHG. The paper was written and edited collaboratively by RR, FZ, and HZH. SMN, LF, and GHG contributed to the editing of the final version. All authors have read and approved the manuscript for publication.
Data Availability Statement
The data generated in this study are not publicly available as they consist of survey responses used for analysis and are presented in summary form within the article's results section. The data are available upon request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and Consent Statement
This study was approved by the Ethics Committee of Tarbiat Modares University, Tehran, Iran (IR.MODARES.REC.1404.059). Participation was entirely voluntary and anonymous, and no personally identifying information was collected.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.