
Abstract
Although differences between males and females in the diagnosis and management of cardiovascular diseases are well recognized, there is a paucity of studies evaluating the impact of sex on the perception and satisfaction of cardiovascular care. The purpose of this study is to evaluate potential sex-based disparities in patient experiences with their postoperative care after cardiac surgery. Responses from Hospital Consumer Assessment of Health Care Providers and Systems surveys from patients who underwent open cardiac surgery at a single institution were compared based on sex. Propensity-score matching was performed based on age, race, and type of operation. Answers to survey items were compared between male- and female-matched cohorts. Female patients gave lower overall hospital rankings than their male counterparts (P = .005). Female patients also gave lower scores for questions regarding room cleanliness (P = .02), staff working together (P = .01), and health management education for discharge (P = .02) compared to male patients. Our study demonstrates that there is a disparity in patient satisfaction between males and females among patients undergoing cardiac surgery. Females undergoing cardiac surgery report worse experiences than their male counterparts.
Keywords
Introduction
There is an abundance of literature addressing disparities in access to and delivery of healthcare between males and females. However, literature examining sex-based disparities in patient satisfaction is less robust. Females have been shown to have less positive experiences than males across different patient care settings, including inpatient care, care received in the Veterans Affairs (VA) system, and care for atherosclerotic cardiovascular disease than males.1–3
Differences in perceptions of care between males and females have also been described in surgical patients. Studies demonstrate that females report lower overall satisfaction with surgical outcomes from spinal surgery for lumbar spinal stenosis, elective lumbar spinal surgery, and bariatric surgery than males.4–6 While sex differences in access, diagnosis, and treatment for cardiovascular care have been extensively studied, there is a paucity of studies looking at sex-based disparities in patient satisfaction in cardiovascular care and cardiac surgery care in particular.
Results from studies conducted in cardiac surgery patients have yielded mixed findings. King et al studied the effect of male-female differences on early recovery from cardiac surgery and found that postoperatively, females reported lower life satisfaction than males. 7 However, Sido et al found no significant difference in the level of satisfaction with postoperative treatment between males and females after resection of left atrial tumors. 8 Vitomskyi et al also found no significant sex-based differences in patient satisfaction after cardiac surgery. 9 The limited literature on male-female differences in patient satisfaction in cardiac surgery consists of small studies that offer disparate results.
Sex-based differences in patient satisfaction may be relevant to cardiac surgery patients because males more commonly undergo cardiac surgery than females: among patients who were 18 years or older, Newell et al found that fewer females had cardiac surgeries, including coronary artery bypass graft (CABG), surgical aortic valve replacement, mitral valve repair, and ascending aorta surgery. 10 In addition, females undergoing CABG surgery have a higher operative mortality rate and are at an increased risk of postoperative adverse cardiac outcomes. 11 Thus, it is worth looking for sex-based differences in patient satisfaction and whether there is any correlation between patient satisfaction and postoperative complications.
Furthermore, few studies have investigated specific factors that may contribute to such disparities. Otani et al collected Hospital Consumer Assessment of Health Care Providers and Systems (HCAHPS) survey responses from regular patient experiences at US hospitals and found that nursing care, physician care, staff care, room, and help were positively associated with patient satisfaction. 12 They also reported male-female differences in ratings of the importance of attributes: female patients rated the relationship with nurses as more important to overall satisfaction, whereas male patients rated the relationship with the doctor as more important to overall satisfaction. 12 This suggests that there are sex differences in specific factors that contribute to patient satisfaction with hospital care. Therefore, it is worthwhile to investigate sex-based differences in specific factors for patients undergoing cardiac surgery, as these may impact patient satisfaction ratings.
Overall, the existing literature indicates that there are disparities between males and females in patient satisfaction, with females often reporting less favorable experiences. Our goal is to determine whether there are sex-based disparities in patient satisfaction among cardiac surgery patients and to identify specific aspects of the patient experience that may contribute to such disparities.
Method
This study received approval from the Northwell Health Institutional Review Board (IRB#:23-0755), and patient consent requirements were waived.
Responses from HCAHPS and Northwell Hospital surveys from patients who underwent open cardiac surgery at a teaching hospital in a suburban location in New York between 2019 and 2022 were collected. Out of a total of 3341 patients who underwent open cardiac surgery, 782 (23.4%) completed the HCAHPS survey. The HCAHPS survey has been shown to be sensitive in identifying male-female differences in patient satisfaction. 3
The HCAHPS and Northwell Hospital survey questions are listed in Supplemental Table 1. 13 The questions focus on communication with nurses, communication with doctors, responsiveness of hospital staff, pain management, communication about medicines and discharge information, hospital environment, and global ratings of the hospital. The majority of answers to the questions are on a Likert scale with a variable number of items. Answers to such questions were linearly converted to a 0 to 100 scale for standardization and analysis. Two questions had dichotomous yes/no answers.
Definitions of postoperative complications were obtained from the New York State Cardiac Surgery Reporting System and the STS Adult Cardiac Surgery Database. It has been shown that females who undergo cardiac surgery experience higher rates of postoperative complications.14,15 As differences in postoperative complications may influence patient satisfaction, we chose to compare differences in postoperative complications before and after propensity score matching.
The study measured sex, which was determined by using the sex assigned at birth listed in the patients’ electronic health records. Sex is defined as a biological attribute, while gender is defined as a social and cultural construct. 16 Following the approach of Mokhles et al, we use the terms “male-female differences” and “sex-based” throughout and avoid using “gender” since the electronic health record did not record gender identity. 17
Propensity-score matching (PSM) based on age, race, and type of operation was performed. Male and female patients were matched on a 1:1 ratio using greedy nearest neighbor matching. The efficiency of the PSM procedure in producing comparability of the 2 groups after matching was evaluated using standardized mean differences (SMDs). An absolute SMD of <0.1 was deemed adequate comparability between groups. 18 Descriptive statistics (frequency distribution for categorical variables and mean, median, SD, interquartile range, minimum, and maximum for continuous variables) were calculated. The association between each categorical baseline variable and sex was examined using the χ2 test. The association between each continuous baseline variable and sex was examined using a 2-sample t test or Mann-Whitney U test, as appropriate. Survey items on a continuous scale were compared between male and female patients using a paired t test or Wilcoxon signed-rank test, as appropriate. McNemar's test for matched pairs was utilized to assess the association between categorical variables and sex. The level of significance was set at 5% unless stated otherwise. All aims were analyzed using SAS software Version 9.4.
Results
Patient Demographics
Patient demographic data on race, age, and type of operation before and after propensity score matching are shown in Table 1. The total sample size before propensity score matching was 782, with a higher number of males (n = 569) than females (n = 213). Race was categorized into 4 groups: Caucasian, African American, Asian, and Other. Although the percentage of Caucasian patients is similar between males and females (67.3% vs 68.4%), there was a greater percentage of African Americans in the female cohort (11.3% vs 6.2%) and a greater percentage of Asians in the male cohort (13.3% vs 9.4%). A significantly greater percentage of males underwent CABG as compared to females (61.5% vs 41.3%). There were 211 patients in each cohort after propensity score matching. There were no statistically significant differences in age, race, and type of operation between males and females after matching.
Pre and Post Match Patient Demographics.

Race data were missing for 5 males.
Hospital Consumer Assessment of Health Care Providers and Systems Standardized Scores
Standardized survey scores of propensity score–matched cohorts are shown in Table 2. Females gave statistically significantly lower overall hospital ratings than males (91.45 vs 95.17, P = .005). Statistically significant differences were revealed for 3 additional questions on the HCAHPS survey: room cleanliness (87.94 vs 92.50, P = .02), staff working together (91.83 vs 95.48, P = .01), and health management education for discharge (83.18 vs 87.78, P = .02).
Standardized Survey Scores in Propensity Matched Cohort.a
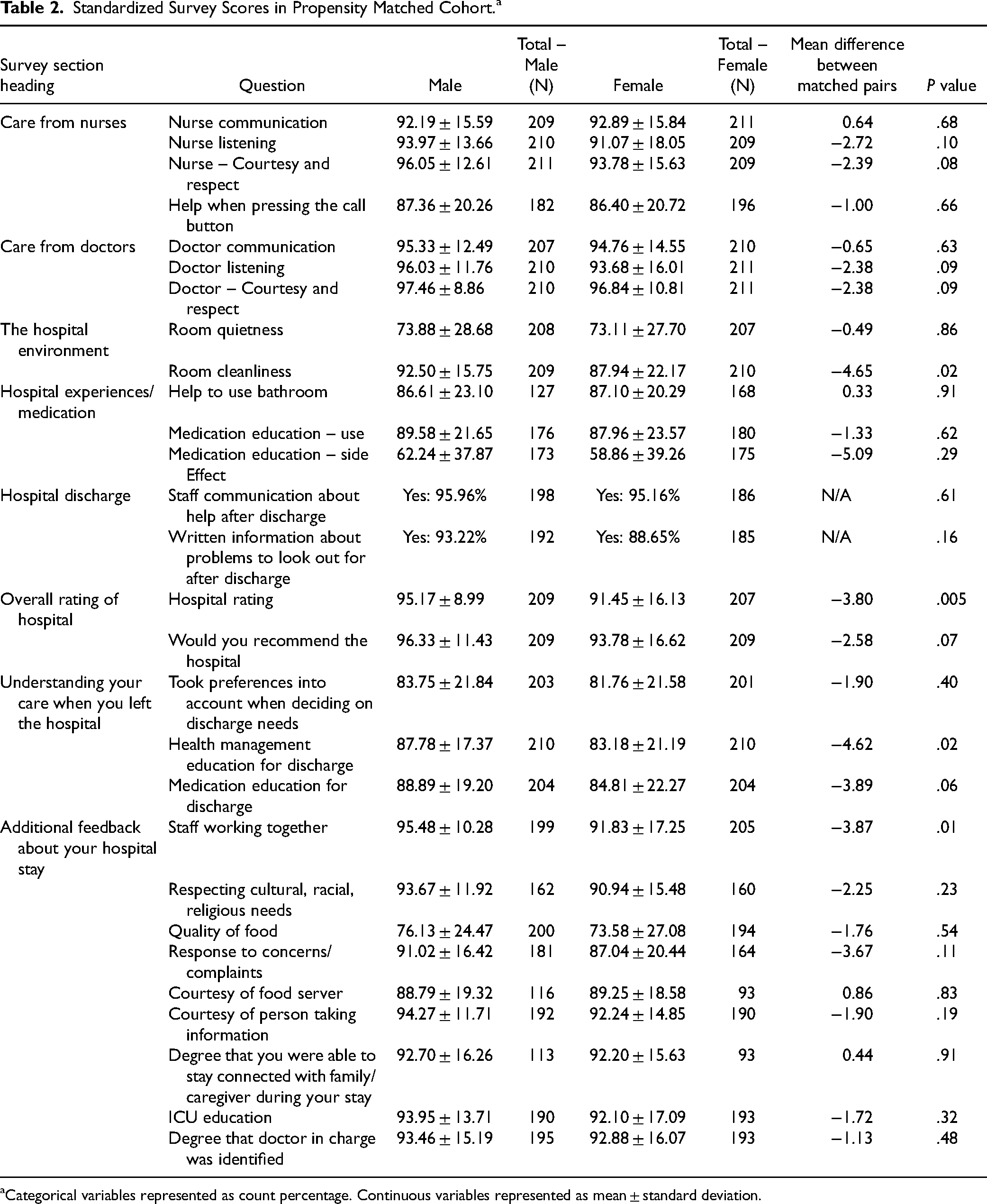
Categorical variables represented as count percentage. Continuous variables represented as mean ± standard deviation.
There were 3 survey questions that showed near-significant findings, with females reporting lower scores than males: nurse courtesy and respect (96.05 vs 93.78, P < .08), medical education for discharge (88.89 vs 84.87, P < .06), and would you recommend the hospital (96.33 vs 93.78, P < .07). For the majority of the remaining questions, females reported lower average scores than males, although the differences were not statistically significant.
Postoperative Complications
There were no statistically significant differences in major postoperative complications before propensity score matching (Table 3). After propensity score matching, the male cohort did have a higher rate of postoperative atrial fibrillation (42.2% vs 28.4%, P = .003). Although females had a longer length of hospital stay before propensity score matching (7 days [IQR 5-10] vs 6 days [IQR 5-8], P < .001) that difference was no longer observed after matching.
Postoperative Complications in Prematch and Postmatch Samples.

Discussion
Patient satisfaction is an important measure of hospital, physician, and staff performance. It is a quality measure and a main provision in the Patient Protection and Affordable Care Act and is associated with clinical outcomes, patient compliance, and patient retention. Studies on patient satisfaction have identified racial and ethnic background, and patient age is independent predictors of patient satisfaction.19,20 After adjusting for patient and provider characteristics, higher overall provider ratings were associated with older patient age, and lower overall provider ratings were associated with Asian race. 21 The type of surgery has also been shown to be predictors of overall patient satisfaction. 22 Given the previously described association between race, age, and type of operation with patient satisfaction, we chose to propensity match for these factors in our analysis to remove these potential confounders. After adjusting for patient and provider characteristics, satisfaction scores did not vary based on sex of the surgeon, suggesting that patient satisfaction scores are more influenced by patient variables than surgeon factors. 21 Our study found that there are sex disparities in patient satisfaction among cardiac surgery patients with females reporting lower satisfaction than males.
It's important to consider the ability of the HCAHPS survey to capture sex-specific nuances in care perception. The HCAHPS survey has been shown to capture male-female differences in patient experience at a population level. 3 However, it may overlook other important aspects of patient care that contribute to patient differences, such as medical care costs and perceptions of safety. 23 While these are limitations, multiple prior studies have used HCAHPS to identify sex differences in patient satisfaction. Elliott et al analyzed HCAHPS survey responses from medical and surgical patients discharged from hospitals and found that females reported less positive experiences than males. 3 Hausman et al analyzed HCAHPS survey responses from VA Medical Centers and found that male, black, and Hispanic patients reported more positive experiences than female and white patients treated at the same facilities. 24 Scholle et al established the Primary Care Satisfaction Survey for Women (PCSSW) as a new survey tool for assessing women's satisfaction with primary care services. 25 Aside from the PCSSW, there is a paucity of survey tools that assess sex differences in patient satisfaction. Future research directions should focus on creating survey tools that specifically assess sex-specific differences in patient satisfaction.
Sex differences in cardiac surgery outcomes have been well described, with females having worse outcomes than males across all types of cardiac surgery, including coronary artery bypass and valve replacement surgery.17,26 Thus, female sex is a risk factor for both major cardiac surgery risk prediction models: EuroSCORE and Society for Thoracic Surgery Risk Score. Multiple studies show that patient outcomes may impact patient satisfaction.27–29 Berkowitz et al showed that for patients who underwent general surgery, vascular surgery, or gynecological surgery procedures, those who experienced complications were less likely to be highly satisfied with their surgery and more likely to regret their surgery. 27 A similar trend was found in thoracic surgery and cardiac surgery patients: Woodfield et al found that thoracic surgery patients who experienced complications reported lower general satisfaction with care than those without. 28 Catalano et al found that major postoperative complications were associated with lower satisfaction with physician care and overall hospital rating. 29
We, therefore, examined the complications of our study cohort to determine if the observed sex differences in HCAHPS scores were reflective of differences in outcomes. Despite poorer outcomes for females undergoing cardiac surgery, we did not find increased postoperative complications in females. Thus, the disparity in HCAHPS scores observed in our study does not appear to be driven by differences in clinical outcomes. This finding may be because we are limited to responses from patients who voluntarily completed the survey, resulting in a different sample population from other studies. Additionally, this is a single-institution study, which may result in limited diversity in patient demographics compared to studies with access to data from multiple institutions. Many studies that examine complications after cardiac surgery only examine short-term mortality, defined as in-hospital/within 30 days, and long-term mortality, defined as after 30 days.14,15 We were unable to use mortality as a complication as deceased patients cannot submit the HCAHPS survey. Although we did examine postoperative complications within 30 days, a meta-analysis by Dixon et al showed that females who underwent cardiac surgery were at a higher risk of postoperative stroke but not at a higher risk of postoperative MI or sternal wound infection. 14 A separate meta-analysis by Dumitriu et al showed the same findings, but also showed that females had lower odds of postoperative atrial fibrillation. 15 Overall, these variable findings show that the mechanisms behind sex disparities in outcomes after cardiac surgery are not well understood and are likely multifactorial.
While the literature has identified differences in patient satisfaction between males and females, few studies have explored the factors that contribute to these disparities. These differences can result from sex differences in expectations and prioritization of certain aspects of patient care, as well as differences in the behavior of staff secondary to sex-based biases. Our study identified specific areas of care where females reported significantly lower satisfaction scores than males, including hospital environment, patient education during transition of care, and cohesiveness of the care team. This may be because females prioritize certain aspects of care more than males. 12 Wessels et al found that female cancer patients reported higher levels of unmet support needs and attached higher value to psychosocial support. 30 This may be because male patients seek support from different sources than females, often their spouses, while females expect social support from hospital staff. 30 This may influence female patients’ expectations of the nurse's role in providing psychosocial support, impacting their satisfaction with nursing care. 30 Teunissen et al found for hospitalized patients, female patients reported less privacy during personal care and visiting hours compared to males, indicating that female patients value privacy. 31
Teunissen et al also showed that female patients were more dissatisfied with nursing care when compared to male patients. 31 Foss et al suggest that the sex difference in satisfaction with nursing care may be due to males and females prioritizing different aspects of care: males focused more on friendly and helpful nurses, while females valued respect from people in positions of power and cooperative physicians. 32 Nursing bias may also play a role in the sex difference in satisfaction with nursing care: when nurses were asked to develop a nursing plan for an imaginary patient, nurses spent less time motivating female patients to be active, providing emotional support, and gave fewer painkillers to females than males. 33
Since cardiac surgery is more common in males, female patients’ expectations before surgery may also influence patient satisfaction. Currently, there are no studies that directly examine the effect of female patients’ expectations on patient satisfaction in cardiac surgery patients. However, Holmes et al assessed for an association between patients’ expectations before cardiac surgery and their recovery after surgery. 34 Using the adapted Cardiac Surgery Patient Expectations Questionnaire (C-SPEQ) as a measure of patients’ expectations, with a higher score indicating more negative expectations, they found that higher C-SPEQ scores were associated with more depressive symptoms, perceived stress, and lower physical composite health-related quality of life (HRQoL) score. 34 While this study did not directly examine patient satisfaction, factors such as depression, stress, and physical composite HRQoL may influence patient satisfaction, suggesting that patients’ expectations may influence patient satisfaction in cardiac surgery patients. Future studies should explore whether patients’ expectations influence patient satisfaction in cardiac surgery patients and whether female patients have different expectations regarding cardiac surgery than male patients.
Implications for Practice
The findings of this study serve as a guide for identifying potential high-impact areas, such as patient support, patient privacy, nursing care, and patient sex-based biases in nursing care, to prioritize and modify in order to narrow the sex gap in patient satisfaction for patients undergoing cardiac surgery.
Limitations
First, our study only examined patients who underwent cardiac surgery. Thus, our results may not be applicable to other surgical specialties. Second, the number of factors included in our propensity matching was limited by our small sample size. There can be additional known or unknown confounders that we did not account for in our match. We also did not match for comorbidities, socioeconomic status, cultural and language background, education level, and pain control, which may be potential confounders for patient experience. Poor pain control is associated with worse patient satisfaction. 35 Patients with comorbidities report worse pain outcomes, while adults with lower socioeconomic status have higher odds of suffering from chronic pain, which results in negative overall patient experience.36,37 Patients from different cultural backgrounds may communicate their pain in ways unfamiliar to Western heathcare workers, resulting in poor pain management. 38 In US adults, a higher education level is associated with fewer reports of bodily pain, which would create more positive patient experiences. 39 Thus, all these factors can serve as potential confounders for patient experience, which may influence patient satisfaction.
Our study only included results from patients who filled out the HCAHPS survey, leaving the views of patients who did not complete the survey unaccounted for. The HCAHPS survey does not report the sex of physicians, nurses, and hospital staff, which makes it unable to assess the effect of sex concordance on patient satisfaction. 3 Lastly, as this is a single-institution study, the institutional culture or staff demographics may influence the results, which may not be generalizable to other institutions.
Conclusion
Our results indicate a disparity in patient satisfaction between males and females among cardiac surgery patients, with females reporting lower overall hospital scores on HCAHPS surveys compared to their male counterparts. We also identified specific areas of patient experience with the most significant disparity in satisfaction scores. Further studies are needed to elucidate the source of this disparity so that steps can be taken to improve the experiences of female cardiac surgery patients.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251379951 - Supplemental material for Sex Disparities in Patient Satisfaction in Cardiac Surgery Patients
Supplemental material, sj-docx-1-jpx-10.1177_23743735251379951 for Sex Disparities in Patient Satisfaction in Cardiac Surgery Patients by Stefanie Ma, BS, Kavi O’Connor, BS, Sashane John, MHS, Xueqi Huang, MS, Nicole Sherman, BS, and Pey-Jen Yu, MD in Journal of Patient Experience
Footnotes
Authors’ Note
Consent to Participate: This study received approval from the Northwell Health Institutional Review Board (IRB#:23-0755), and patient consent requirements were waived. Ethical Considerations: This study received approval from the Northwell Health Institutional Review Board (IRB#:23-0755), and patient consent requirements were waived.
Author Contributions
Stefanie Ma submitted IRB approval, drafted manuscript and tables, wrote revised manuscript; Kavi O’connor assisted with revision of manuscript; Sashane John assisted with drafting of manuscript; Xueqi Huang performed statistical analysis; Nicole Sherman assisted with drafting of manuscript ; Pey-Jen Yu assisted with drafting of manuscript, tables, statistical analysis, and final review of the original and revised manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.