
Abstract
This cross-sectional study compared patient satisfaction with headache care in Veterans Health Administration (VHA) Headache Centers of Excellence (HCoE) and HCoE facilities versus traditional headache care. Using the VHA Survey of Healthcare Experiences of Patients specialty care survey, we analyzed responses from 4317 (14% response rate) veterans with a VHA headache visit who received care from (1) a Veterans Affairs (VA) HCoE provider; (2) a non-HCoE provider within a VA medical center containing an HCoE; or (3) a provider in a VA medical center without an HCoE. Compared to patients at non-HCoE facilities, both HCoE patients and HCoE facility patients reported higher overall satisfaction with their VHA care in general (OR = 1.32, 95% CI = 1.05-1.64; OR = 1.46, 95% CI = 1.38-1.54), respectively. Despite a modest response rate, HCoE and HCoE facility patients reported significantly higher satisfaction across other domains including access and communication, in models adjusting for demographics. These findings advance the conversation regarding the value of HCoEs in delivering high-quality, patient-centered care and expanding HCoE resources may improve satisfaction. Future research should formally investigate methods of improving satisfaction.
Plain Language Summary
Little is known about patient satisfaction with Veterans Health Administration (VHA) Headache Centers of Excellence (HCoE) versus VHA traditional headache care. This cross-sectional study evaluated patient satisfaction with headache care using a validated survey across 3 VHA headache care provider types: (1) an HCoE provider; (2) a non-HCoE provider within a VA medical center (VAMC) containing an HCoE; or (3) a provider in a VAMC without an HCoE. Patients cared for in HCoEs and HCoE facilities report greater satisfaction with their headache care than non-HCoE facility patients in most domains.
Introduction
Patient satisfaction is a key indicator of healthcare quality and is associated with higher treatment adherence and better outcomes, including reduced disability in patients.1–5 Headache patients are commonly dissatisfied with their care, partially due to the disabling nature of headache, the difficulty of finding consistent headache relief, and the many bothersome side effects of available treatments. It takes time and patience of both providers and patients to establish effective treatment(s). Despite the fact the number and purported effectiveness of headache treatments have increased in the last few years, 6 the limited expertise of headache nonspecialists has exacerbated patient frustration.4,5,7 One proposed solution to improving headache care has been the implementation of the Headache Centers of Excellence (HCoE).7,8 Headache Centers of Excellences are nested within VA Medical Centers (VAMCs) and offer direct access to providers and care teams with specialty training in headache medicine and an array of state-of-the-art interventions including nonpharmacological modalities and interdisciplinary headache clinics. Additionally, HCoE providers develop policies and protocols within their VAMCs and lead headache educational initiatives for veterans, care partners, and providers.9,10
Persons with migraine disease seen by headache specialists have reported higher satisfaction with care. 5 Two uncontrolled pilot studies investigated the effects of specialized headache management programs and found that patients reported higher satisfaction with headache care after treatment.11,12 However, little is known about the impact of establishing an HCoE on patient satisfaction; furthermore, no studies have compared patients receiving care at an HCoE to patients receiving headache care elsewhere within the same healthcare system.
This study aimed to evaluate patient satisfaction using the validated Specialty Survey of Healthcare Experiences of Patients (SHEP) from the Veterans Health Administration (VHA) Office of Quality and Patient Safety across 3 headache care settings in the VHA: HCoE patients, HCoE facility patients, and non-HCoE facility patients. It was hypothesized that (1) HCoE patients would have higher satisfaction in their care than non-HCoE facility patients, and (2) HCoE facility patients would have higher satisfaction than non-HCoE facility patients, even if their provider was not affiliated with the HCoE, because of the diffusion of headache information and HCoE protocols within a given facility.
Design
This is a cross-sectional study of veteran satisfaction with their headache care at the VHA.
Participants
VHA Office of Quality and Patient Safety procedures were utilized throughout this process from sampling, survey mailing and data management. 13 The SHEP team identified participants from 32 VAMC including the 13 HCoEs and facilities matched with the HCoEs based on facility complexity and Veteran Integrated Service Network (VISN). VISNs are regional care systems within the VHA, which were matched to minimize geographical effects of offered care and patient populations. 14 Facility complexity is a method used in the VHA to define clinical complexity capability based on criteria such as the availability of specialty and support programs. VHA SHEP used a stratified random sampling method to select patients to receive the survey. The sample was stratified by medical center, specialty care provider, sex, and HCoE status, and women were oversampled.
Headache Centers of Excellence (HCoE) Status
HCoEs are sites selected for participation in a national program designed to provide excellent interdisciplinary care to veterans with headache disorders. At the time that the HCoE program was Congressionally manadated, the VA had a total of 3 United Council for Neurologic Subspecialties (UCNS) board-certified headache medicine physicians. HCoEs have at least 1.0 FTE UCNS-certified physician and also provide top-of-the-line care for headache, including procedures and devices that not systematically offered in other settings in the VHA. HCoEs are required to provide interdisciplinary management of headache, such as health psychology, pharmacy, and complementary and integrative health approaches, and deliver training and educational initiatives within their VAMCs.
Patients were included if they had an outpatient encounter documented with an International Classification of Diseases (ICD) headache diagnostic code at any of the 32 selected VAMCs within the 30 days prior to the 5 monthly survey distribution dates. Patients were selected based on 3 mutually exclusive locations of care for their index encounter in the VHA: (1) within an HCoE (ie, HCoE), (2) within facilities housing an HCoE though not directly seen by an HCoE provider (ie, HCoE facility), or (3) within facilities without an HCoE (ie, non-HCoE facility). HCoE patients were seen by a provider. HCoE providers were identified based on a list of designated providers from Clinical Leads at each of the 13 HCoEs (Supplemental Table 1). HCoE facility patients included patients whose headache encounter occurred at a facility with an HCoE, but the patient was not seen by a designated HCoE provider. Non-HCoE facility patients were seen at a facility without an HCoE.
Patients were not sampled if they had already completed any SHEP survey for any type of care received within the last 12 months nor did they receive compensated for survey participation.
Procedures
Participants were sent the SHEP Specialty Care survey with an instruction indicating participants should review their recent visit for headache care. Surveys were sent monthly between August 2022 and December 2022 with a one month look back for the patient to select their recent headache visit. Patients received an initial survey via mail and were sent a follow-up reminder postcard. Patients with an email on file also received an electronic version of the survey. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for cross-sectional studies.
Measures
Demographics
Demographic variables included sex (male or female), age, race (White, Black, Asian, American Indian/Alaskan Native, Native Hawaiian/Pacific Islander, Multiracial), and ethnicity (Hispanic/Non-Hispanic). All demographic variables were self-reported, measured categorically, and represent the routine demographic variables collected by the VA SHEP survey.
Survey of Healthcare Experiences of Patients (SHEP) Specialty Care Survey Scores
The SHEP team utilizes a system of surveys to collect information about veterans’ experiences in the VHA under the auspices of the VHA Office of Quality and Patient Safety. These instruments are based on the industry standard Consumer Assessment of Healthcare Providers and Systems (CAHPS) surveys, which are developed by the National Committee for Quality Assurance. These surveys were developed with input from accrediting bodies, healthcare providers and associations, purchasers, and consumers. 15 The CAHPS surveys were developed using modern psychometric methods, including cognitive testing for item-level validity, psychometric validation at the level of the item and indices, and field testing to confirm instrumental validity and utility. 16 These surveys are the gold standard method to assess patient satisfaction in the VHA. Our study utilizes the SHEP Specialty Care survey, which is a 46-item measure designed to assess patient satisfaction with specialty care. Standardly reported SHEP index scores from this survey are outlined below. Additional CAHPS survey questions are included in Supplemental Table 2.
Survey of Healthcare Experiences of Patients (SHEP) Overall Satisfaction Single-Item Score
The SHEP Overall Satisfaction Single-Item score measures the patient's overall satisfaction with their care at the VHA in general,not only with headache care. The only item in this measure asks “Overall, how satisfied are you with the health care you have received at your VA facility during the last 6 months?” Responses are measured on a scale from 1 to 6 with responses ranging from “Very dissatisfied” to “Very satisfied.” The remainder of the composite scores are specifically related to headache care.
Survey of Healthcare Experiences of Patients (SHEP) Access Composite Score
The SHEP Access Composite Score measures patient satisfaction with getting timely appointments, care, and information. 13 Three questions comprise this measure, including: “In the last 6 months, when you contacted this provider's office to get an appointment for care you needed right away, how often did you get an appointment as soon as you needed?,” “In the last 6 months, when you made an appointment for a check-up or routine care with this provider, how often did you get an appointment as soon as you needed?,” and “In the last 6 months, when you contacted this provider's office during regular office hours, how often did you get an answer to your medical question that same day?” Responses were scored on a 4-point scale from “Never” to “Always.” This measure demonstrated good internal consistency in this sample (Cronbach's Alpha: .87).
Survey of Healthcare Experiences of Patients (SHEP) Communication Composite Score
The SHEP Communication Composite Score measures satisfaction with how well providers communicate with patients. 13 Two questions comprise this measure, including: “In the last 6 months, how often did this provider show respect for what you had to say?” and “In the last 6 months, how often did this provider spend enough time with you?” Responses were scored on a 4-point scale from “Never” to “Always.” This measure demonstrated excellent internal consistency in this sample (Cronbach's Alpha: .93).
Survey of Healthcare Experiences of Patients (SHEP) Care Coordination Composite Score
The SHEP Care Coordination Composite Score measures satisfaction with how providers use information to coordinate patient care. 13 Three questions comprise this measure including: “In the last 6 months, how often did this provider seem to know the important information about your medical history?,” “In the last 6 months, when this provider ordered a blood test, x-ray, or other test for you, how often did someone from this provider's office follow up to give you those results?,” and “In the last 6 months, how often did you and someone from this provider's office talk about all the prescription medicines you were taking?” Responses were scored on a 4-point scale from “Never” to “Always.” This measure demonstrated adequate internal consistency in this sample (Cronbach's Alpha: .70).
Survey of Healthcare Experiences of Patients (SHEP) Office Staff Composite Score
The SHEP Office Staff Composite Score measures patient satisfaction with the helpfulness, courteousness, and respectfulness of office staff at a facility. 13 Two questions comprise this measure, including “In the last 6 months, how often were clerks and receptionists at this provider's office as helpful as you thought they should be?” and “In the last 6 months, how often did clerks and receptionists at this provider's office treat you with courtesy and respect?” Responses were scored on a 4-point scale from “Never” to “Always.” This measure demonstrated good internal consistency in this sample (Cronbach's Alpha: .87).
Survey of Healthcare Experiences of Patients (SHEP) Provider Rating Single-Item Score
In this study, the SHEP Provider Rating Single-Item score measures a patient's satisfaction with the individual provider giving care at their headache visit. This measure is derived from a single question: “Using any number from 0 to 10, where 0 is the worst provider possible and 10 is the best provider possible, what number would you use to rate this provider?” Responses are scored from 0 to 10, with a score of 9 to 10 considered excellent care.
Analysis
The analytic sample was limited to patients with a “completed” specialty care survey of 10 or more answered questions including a positive response to having a headache visit. Data were cleaned, variables were visually inspected, and their distributions were described. Only observed variables are reported.
Survey of Healthcare Experiences of Patients scores (both composite and single-item) were dichotomized for analysis due to the non-normal distribution of the variables, as is common in the patient satisfaction literature.17,18 Survey of Healthcare Experiences of Patients composite scores were coded into “always satisfied” versus “not always satisfied” (all other response choices); this scoring is commonly used in the literature.17,18 Overall satisfaction Single-Item scores were dichotomized into “satisfied” or “very satisfied” versus all lower satisfaction scores . Provider Rating Single-Item scores was dichotomized into a score of 9 or 10 (eg, “excellent care”) versus all lower satisfaction scores. These methods for composite and single-item scoring are consistent with the standardized reporting of the SHEP Specialty Care survey. 13
Chi-square tests examined categorical demographic variables by headache care location type. Logistic regressions evaluated the associations between variables of interest [HCoE Status (HCoE, HCoE Facility, Non-HCoE), sex (male compared to female), age category (reference 18-24), race (reference: White), and ethnicity (Hispanic vs non-Hispanic)] and SHEP Specialty Care Survey scores, adjusted for HCoE Status, sex, age, race, and ethnicity. Individual unadjusted logistic regression models were conducted and are included as a supplemental table (Supplemental Table 1). All analyses included survey design weights factoring in facility and specialty provider and were clustered by headache care location type. A P-value under .05 was considered statistically significant in a 2-tailed test. Cases missing data from response categories or demographic variables were not included in the analysis of those variables. Missing values were not imputed (missing <7%). All models included participants who responded to the domains of patient satisfaction, which ranged from a total of 3,204-4,033. All analyses were performed using SAS 9.4. 19
Results
Response Rates
A total of 104,661 patients were eligible for this study, of which a sample of 30,795 patients were selected and sent surveys. A total of 4,569 eligible veterans returned their surveys. A total of 252 respondents did not confirm a headache visit in the last 30 days and were removed due to ineligibility. The analytic sample contained 4,317 participants (14.1% response rate) who completed at least 10 of the SHEP Specialty Care Survey items (Figure 1). Response rates ranged from 13.9% to 15.3% over the study period. The survey completion rate was similar across specialty clinic types, ranging from 10.8% completion from Women's Health clinic to 17.4% completion in Neurology clinic.

Flow Diagram for Study Participants.
Respondent Characteristics
Our patient respondent population was mostly male (62.8%, 2,709/4,317), White (68.6%, 2,750/4,009), and non-Hispanic (90.0%, 3,662/4,068). Respondents were well-distributed across age bands (Table 1). HCoE patients were less likely to be women (P = .002) and less likely to be Black (P < .001) than HCoE facility patients and non-HCoE facility patients (Table 1). Therefore, odds ratios presented below are adjusted for sex and race.
Demographics of Survey Respondents by HCoE Status.

Abbreviations: AI/AN, American Indian/Alaska Native; HCoE, Headache Centers of Excellence; NH/PI, Native Hawaiian/Pacific Islander.
P values presented only for group differences with cell sizes ≥20.
Satisfaction Description
Rates of endorsing “always satisfied” in each SHEP domain (or “excellent care” for the Provider SHEP item) are described in Table 2. Over three-quarters of respondents endorsed being satisfied overall with their care at the VHA (3,029/3,895, 77.8%). Regarding headache-specific care, over half of patients reported being satisfied with their provider (2,643/3,945, 67.0%), communication (2,463/4,033, 61.1%), and office staff (2,336/3,937, 59.3%). Over one-third of patients reported being satisfied with their access (1,164/3,204, 36.3%) and care coordination (1,516/4,001, 37.9%).
Unadjusted Rates of Endorsing “Always Satisfied” Across SHEP* Composite Score Domains by HCoE Status.
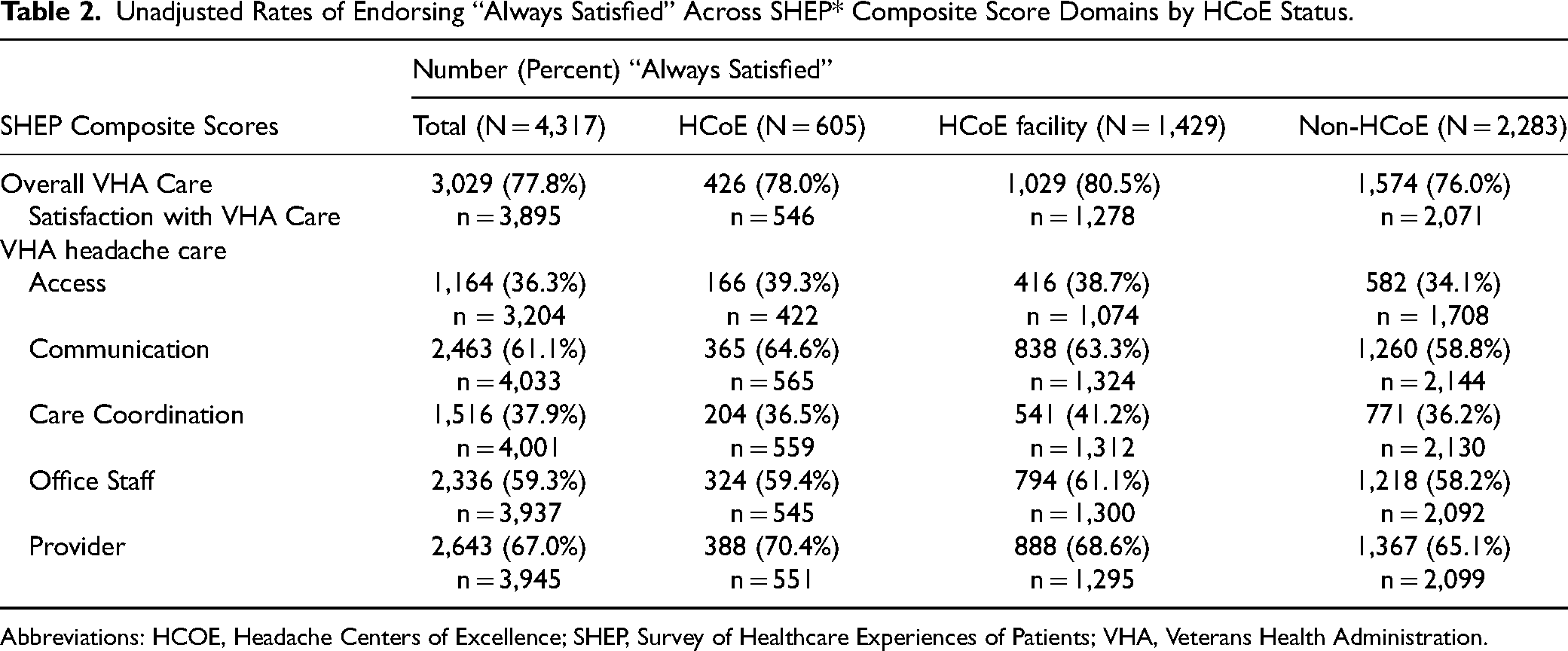
Abbreviations: HCOE, Headache Centers of Excellence; SHEP, Survey of Healthcare Experiences of Patients; VHA, Veterans Health Administration.
Satisfaction by HCoE Status
Adjusting for demographics, patients from HCoE clinics (aOR = 1.32, 95% CI = 1.05-1.64) and HCoE facilities (aOR = 1.46, 95% CI = 1.38-1.54) had significantly higher odds of reporting satisfaction with their overall VHA care than patients seen in a non-HCoE facility (Table 3). This pattern also held true across all SHEP domains assessing satisfaction with headache care, although the aORs did not reach statistical significance for Care Coordination and Office Staff for the HCoE versus non-HCoE comparisons. We observed no significant differences in SHEP-assessed satisfaction across patients seen within HCoEs compared to those seen in HCoE facility locations (Table 3).
Adjusted Odds of Patients Endorsing “Always Satisfied” on SHEP Composite Patient Satisfaction Scores.a

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; HCoE, Headache Centers of Excellence; SHEP, Survey of Healthcare Experiences of Patients; VHA, Veterans Health Administration.
SHEP composite scores were coded as 1 = always satisfied, and 0 = not always satisfied. For race, odds were reported only groups with individual cell sizes greater than n = 20 (White, Black, and Multiracial). Odds were adjusted for sex, age, race, and ethnicity.
Satisfaction by Age
Adjusting for other demographics and HCoE Status, older age groups reported increasingly higher odds of satisfaction with their overall VHA care compared to 18–34 year-olds, peaking at the 65–74 age band (Table 3). This result was similar for satisfaction with headache care Access, Care Coordination, Office Staff, and Provider (Table 3). With respect to Communication, all age groups between 45 and 74 had significantly higher odds of satisfaction with headache care Communication compared to ages 18–34.
Satisfaction by Race and Ethnicity
Adjusting for other demographics and HCoE Status, Black patients had lower odds of satisfaction with headache care Communication (aOR = 0.87, 95% CI = 0.82-0.91) compared to White patients. However, Black patients had higher odds of satisfaction with headache care Access and Office Staff. Multiracial patients reported significantly lower odds of satisfaction with VHA care overall (OR = 0.66, 95% CI = 0.61-0.73) and all components of headache care except Care Coordination compared to White patients (Table 3). Adjusting for demographics and HCoE Status, Hispanic patients had higher odds of satisfaction with overall VHA care (aOR = 1.25, 95% CI = 1.15-1.36), as well as most SHEP-assessed domains of headache care (Table 3). Hispanic patients had lower odds of satisfaction with headache Office Staff (aOR = 0.80, 95% CI = 0.75-0.85). The odds that a Hispanic patient deemed their headache provider gave “excellent care” was 1.36 times higher than that of a White patient (95% CI = 1.27-1.45).
Satisfaction by Sex
Adjusting for other demographics and HCoE status, men and women had similar odds of satisfaction with overall VHA care and Office Staff (Table 3). Regarding headache care, women had significantly higher odds of satisfaction with Communication (aOR = 1.49, 95% CI = 1.42-1.56), Care Coordination (aOR = 1.18, 95% CI = 1.14-1.22), and their headache Provider (aOR = 1.16, 95% CI = 1.12-1.20) compared to men. Women had significantly lower odds of satisfaction with headache care Access compared to men (aOR = 0.89, 95% CI = 0.86-0.93).
Discussion
Patients receiving headache care in HCoE facilities and directly by HCoE providers reported higher satisfaction than non-HCoE facility patients in most domains. These findings were expected given the high level of headache care offered at HCoEs and HCoE facilities, as described in our qualitative study of veterans with headache. 20 These veterans reported that HCoE headache providers were knowledgeable about headache and integrated a variety of different headache management approaches (eg, preventive medications and nonpharmacological options). Patients felt “heard” with providers who were attentive and caring, after feeling their previous providers were dismissive or uninterested in their headache disease. These findings underscore the value of having a HCoE within a VAMC and highlight the impact of specialized care provided by HCoE providers, reinforcing the need to invest in programs intended to improve headache care quality and delivery and implement educational and training initiatives that promote standardized, high-quality headache care across all VAMCs.
There were 2 domains (Care Coordination and Office Staff scores) where satisfaction was not significantly higher in HCoE patients versus non-HCoE facility patients. Administrative domains are a barrier for many clinical programs in the VHA, particularly regarding hiring new staff and securing physical space for clinics. 21 HCoEs included in this study were established at different times periods prior to the time of the study, which may contribute to lower scores in new sites. Administrative resources should be established in advance of establishing an HCoE program to ensure successful implementation. Future research should interview headache site leads to understand how programs have overcome those barriers in the past and provide guidance for future HCoEs.
Compared to non-HCoE facility patients, HCoE facility patients reported higher satisfaction in all domains. However, there were no significant differences between HCoE patients and HCoE facility patients in any domain. These results suggest that HCoEs elevate care quality and awareness of headache throughout their facilities and/or selected HCoE sites already delivered high-quality headache care across the facility prior to their establishment as CoEs. HCoEs bring additional benefits, including advanced headache treatments and interdisciplinary care models, which may diffuse headache care improvements throughout the facility. Expanding provider education on advanced headache treatments and interdisciplinary approaches can help reduce delays in diagnosis and referrals. 20
Findings suggest that there is variation in satisfaction in different domains by demographic variables. Satisfaction rates increased with age across categories, which is consistent with the broader literature on patient satisfaction particularly in ambulatory care settings. 22 Interventions to target patient satisfaction should be sure to include the perspectives of younger patients, as they tend to be the least satisfied with headache care in the VHA.17,19–21 Future work should engage a broad array of headache patients in structured interviews to inform initiatives aimed at improving satisfaction and addressing health literacy needs satisfaction.
Limitations and Future Directions
This study focuses on HCoEs within the VHA integrated care network and may not generalize to other healthcare settings. The study is also limited by our modest response rate, as nonresponse could be linked to satisfaction with services provided. Although a modest overall response rate was observed compared to other studies who analyzed data from the SHEP-Patient Centered Medical Home version,23,24 the response rate across specialty clinic types (14.0%) corresponded to the overall response rate published from the VHA Coordination of Specialty Care-Patient survey (15.6%). 25 The current study can only comment on contemporaneous findings as a cross-sectional study. However, future longitudinal research on patient satisfaction before and after care at the HCoE could elucidate differences between HCoE and HCoE facility-level care. This study also does not include information on headache burden. Patients with severe or frequent headaches may rate their care quality more poorly than patients with well-managed headache. HCoE patients typically have high headache burden which may influence these results. As such, future studies could also measure headache severity, frequency, and treatment in HCoE and non-HCoE facility patients to further explore the meaning of our results.
Examining satisfaction by provider type and comparing interdisciplinary versus single-discipline care models could clarify these results. Finally, future studies should include quality improvement projects to increase patient satisfaction with headache care across care settings in the VHA. Implementing the stepped care model in VHAs with HCoEs has potential to improve patient satisfaction. 26 Similarly, implementing a national telehealth HCoE program could increase access to tertiary care headache resources for VHAs that do not yet have a local HCoE.
Conclusions
Patients who received headache care at facilities that included an HCoE, and directly from HCoE providers, reported generally had higher satisfaction than patients who received headache care at non-HCoE facilities. Headache Centers of Excellence hold promise as a tool to improve satisfaction in headache care. Future studies should interview headache patients to better understand their satisfaction and experimentally evaluate components of HCoEs to determine active components.
Abbreviations
aOR, adjusted odds ratio; CI, confidence interval; HCoE, Headache Centers of Excellence; ICD: International Classification of Diseases, OR, odds ratio; SHEP, Survey of Healthcare Experiences of Patients; UCNS, United Council of Neurological Subspecialties; CAHPS, Consumer Assessment of Healthcare Providers and Systems; VAMC, Veterans Affairs Medical Centers; VHA, Veterans Health Administration; VISN, Veteran Integrated Service Network.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251346615 - Supplemental material for Patient Satisfaction in the Headache Care at the Veterans Health Administration Headache Centers of Excellence: A Cross-Sectional Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735251346615 for Patient Satisfaction in the Headache Care at the Veterans Health Administration Headache Centers of Excellence: A Cross-Sectional Study by Addison L. Kimber, Brenda T. Fenton, Bin Zhou, Sarah E. Anthony, Jason J. Sico and Elizabeth K. Seng in Journal of Patient Experience
Footnotes
Acknowledgments
The views expressed in this study are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. The authors thank the Survey of Healthcare Experiences of Patients (SHEP) team for sharing their data regarding veteran satisfaction with their headache care.
Authors’ Note
All listed authors should have contributed to the manuscript substantially and have agreed to the final submitted version. Substantial contributions provided by each author include the following: Concept and design: ALK, BTF, EKS, and JJS. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: ALK, BTF, EKS, and JJS. Critical review of the manuscript for important intellectual content: All authors. Statistical analysis: ALK and Zhou. Obtained funding: JJS. Administrative, technical, or material support: BTF, SEA, EKS, and JJS. Supervision: BTF, JJS, and EKS.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ALK reports no conflicts relevant to the manuscript; BTF reports no conflicts relevant to the manuscript; BZ reports no conflicts relevant to the manuscript; SEA reports no conflicts relevant to the manuscript; JJS reports no conflicts relevant to the manuscript; EKS has consulted for GlaxoSmithKline, Theranica, and Click Therapeutic and served as an advisory board member for Abbvie.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the special purpose medical service funding provided by the Department of Veterans Affairs, award number SP80DPE.1-0160.
Authors’ Note
Ethical Considerations: The EXEMPT VHA HCoE Administrative Data Headache Cohort protocol (1582990) has been approved under Institutional Review Board of the VHA Connecticut Healthcare System in March 2020, which approved a waiver of informed consent. Data Availability: Anonymized data not published within this article will be made available by request from any qualified investigator. As per VA policy, analytic datasets used for this study are not permitted to leave the VA firewall without a Data Use Agreement. ALK, BTF, BZ, SEA, JJS, and EKS affirm that the manuscript is an honest, accurate, and transparent account of the resource and analyses being described; no important aspects have been omitted. ALK had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Methods: Study procedures were approved under IRB protocol 1582990.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.