
Abstract
Breast cancer subtypes differ in prevalence, aggressiveness, and availability of targeted therapies. However, research often examines the lived experiences of individuals with breast cancer collectively. One subtype, Triple-Negative Breast Cancer (TNBC) is an aggressive form of cancer that lacks targeted therapy and has higher recurrence and mortality rates. This study aims to explore the lived experiences of individuals diagnosed with TNBC, from diagnosis through active treatment. Audio-recorded interviews were conducted with 11 women who had completed treatment for TNBC. Ages ranged between 26 and 63 years. Data collected were analyzed using interpretative phenomenological analysis. Four group experiential themes were extracted: “Living in shellshock,” “Fighting the aggressive beast,” “Pulling out the beast,” and “Facing the unknown.” Participants described substantial emotional distress stemming from the aggressive progression of TNBC and its earlier onset. The rarity of TNBC further intensified perceptions of reduced survival odds. This study underscores the importance of comprehensive care for TNBC patients, incorporating ongoing engagement with TNBC survivors, access to mental health services, and inclusive screening that includes younger women.
Keywords
Introduction
Breast cancer is one of the most common cancers globally, affecting about one in 12 women. 1 Approximately 15% of breast cancers are Triple-Negative Breast Cancer (TNBC), 2 a subtype lacking estrogen, progesterone, and human epidermal growth factor-2 receptors. 3 Triple-Negative Breast Cancer is more aggressive, has higher recurrence rates,4,5 and is often diagnosed at advanced stages. 6 About 80% of recurrences occur within 5 years following diagnosis, 7 though the risk decreases significantly thereafter. 8 Despite advancements in reducing mortality, long-term survival for TNBC lags behind other breast cancer subtypes. 2
Adding to this concern, TNBC is overrepresented in younger women, African-American women, and those with a family history of breast cancer.5,6 However, early detection in younger women is challenging due to dense breast tissue and a lack of calcium deposits, which limit the effectiveness of mammograms for identifying abnormalities. 9 Moreover, mammograms are typically recommended for women aged 50 to 74, thus impacting the opportunity for early detection in younger women. 10 To address this gap, genetic testing has been introduced, enabling the identification of mutations associated with breast cancer, thereby supporting prevention and early detection. 11 The absence of specific receptors in TNBC further excludes targeted therapies, leaving chemotherapy, surgery, and radiotherapy as primary treatments. 12 However, immunotherapy has recently been introduced as it enhances the immune response to cancer cells. 12
Although psychosocial research on breast cancer is extensive,13–16 only 3 studies5,17,18 target persons diagnosed with TNBC. Bollinger et al 17 examined the challenges of young African American women with TNBC, identifying key issues such as: (1) prolonged and more aggressive treatment protocols; (2) struggles with feminine identity and fertility concerns; and (3) a greater burden of care, compared to those with estrogen receptor-positive breast cancer. Data were collected in 3 phases examining: the impact of diagnosis and the neoadjuvant phase; the adjuvant phase including surgery; and the period approaching or following completion of treatment. The study presented a thematic analysis targeting: female identity, fertility, reproduction and parenting, caregiving burden, psychosocial development, and a sense of alienation. Similarly, Turkman et al's 5 study demonstrated that TNBC's aggressive progression, limited treatment options, and high recurrence rates, significantly increased patients’ stress and uncertainty. Many participants, especially younger women and African Americans, expressed decisional regret, citing a lack of adequate information and support during the treatment process. Post et al 18 combined a parallel mixed design using qualitative interviews and quantitative assessments, to explore patient experiences transitioning from curative therapy to surveillance. The quantitative assessments used were the “Fear of cancer recurrence inventory” and the “Hospital Anxiety and Depression scale.” The findings obtained highlight that fear of recurrence remains a predominant concern affecting quality of life even during the surveillance phase. Patients with TNBC expressed feeling distinct from those with other breast cancer subtypes and emphasized the need for care interventions specifically tailored to their experiences.
Despite growing research on TNBC, this study aims to contribute to the extant literature by exploring, analyzing, and also presenting findings specifically by treatment phase. This enables a more in-depth focus on patient experiences during each phase of the care process.
Methods
Study Design
An Interpretative Phenomenological Approach (IPA) was chosen, as it facilitates an in-depth exploration of the participants’ lived experiences, while acknowledging the researchers’ interpretative role.19,20 Interpretative Phenomenological Analysis is based on 3 key theoretical foundations: phenomenology, hermeneutics, and ideography. Phenomenology seeks to explore participants’ lived experiences through their subjective first-person accounts, while hermeneutics emphasizes the analyst's role in interpreting how individuals make sense of these experiences. The study's ideographic approach incorporates the in-depth examination of each individual case before drawing comparisons across multiple cases.
Participants
Inclusion criteria to participate in this study included being aged 18 years and over; having been diagnosed with stage I to III TNBC; and having completed their curative cancer treatment within the past year and being non-metastatic. Eleven females were recruited via purposive sampling between March 2023 and January 2024. Their ages ranged between 26 and 63 years, with a mean age of 48.3 years. The participants had all received treatment at single public-funded oncology center in Malta. Eight participants commenced their treatment with chemotherapy and 3 with surgery. Three participants underwent a mastectomy, while 8 participants underwent a lumpectomy. Most participants (72.7%) were employed, and all were in a relationship and had children.
Table 1 provides an overview of the participants’ demographic information. The participants’ confidentiality was safeguarded by replacing their names with pseudonyms.
Demographic Details of Participants.

Data Collection
Audio-recorded interviews were conducted by the first author. A single interview was held in the location chosen by the participant. Eight participants had their interviews conducted in their individual home; one participant was interviewed at her workplace and 2 participants were interviewed in a university office. The interviews lasted between 22 and 85 min, with an average duration of 51.7 min.
An open-ended question namely: “Can you describe your experience following a diagnosis of TNBC?” was asked. Probing questions, such as “how did such a situation affect you?” were asked whenever further information was required.
Data Analysis
Data were analyzed according to the principles of IPA as described Smith et al. 19 Each transcript was individually read by the following 2 authors [JS;JA] and exploratory statements targeting descriptive, linguistic, and conceptual insights were generated. The data extracts were then coded, and experiential statements were identified and grouped into personal experiential themes for each case. Similarities and discrepancies across cases were analyzed to create group experiential themes (GETs). These authors then collaboratively agreed upon the final set of GETs.
Ethical Considerations
The study adhered to the Declaration of Helsinki and all procedures in this study were conducted in accordance with the Faculty of Health Sciences Research Ethics Committee, University of Malta (Approval number: FHS2022-00338) approved protocols. Two healthcare professionals provided potential participants with an information sheet explaining the nature of the study. Written informed consent was obtained from the patients for their anonymized information to be published in this article. Psychological support was available, should any participant experience distress; however, this service was not availed of.
Rigor
Trustworthiness was evaluated using Yardley's model. 21 This incorporated: (i) inclusion of verbatim extracts in this account; (ii) provision of detailed descriptions of the research design, participant recruitment, and data analysis; (iii) use of a reflexive diary, to identify biases and observations; and (iv) exploring an understudied topic, namely the lived experiences of females with TNBC.
To maintain credibility, a thorough audit trail was maintained by the researchers to document analytical decisions and reflexive processes throughout the study. Furthermore, research triangulation enhanced the validity of the findings by involving researchers from diverse academic backgrounds at every stage, from data collection to analysis. This multidisciplinary approach allowed for a more comprehensive and nuanced interpretation of the results.
Results
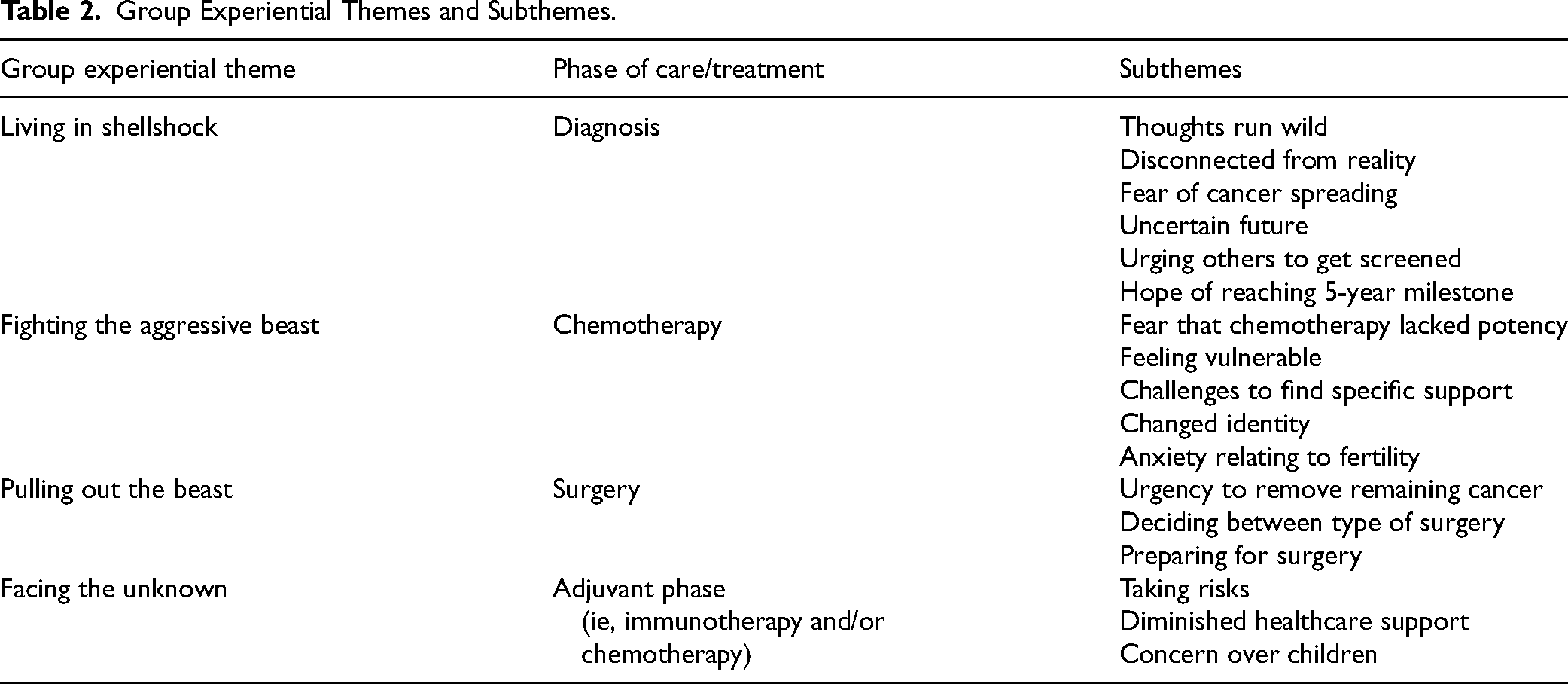
Four GETs “Living in shellshock,” “Fighting the aggressive beast,” “Pulling out the beast,” and “Facing the unknown” were derived from the data. Table 2 delineates the resultant GETs and the corresponding phase of treatment and subthemes.
Group Experiential Themes and Subthemes.
Living in Shellshock
Receiving a diagnosis of an aggressive cancer profoundly affected the participants’ well-being, triggering severe psychological distress. Many described losing control over their thoughts. Carla likened her mental turmoil to the chaotic energy of a wild, untamed stallion. “It [my mind] seemed extraneous to my body… like a wild stallion, bolting and turning around in an uncontrolled and unruly manner…. thoughts raced through my mind, and I could not control or rein them” (Carla).
Participants also conveyed a sense of detachment from reality, describing shock and disorientation, as they underwent medical investigations in quick succession. This left them with little time to process their diagnosis and reinforced a feeling that life was irrevocably altered. “My head was in the clouds; I was overwhelmed with all the investigations …from that point onwards my life was never going to be the same” (Carla)
The aggressive nature of TNBC triggered fears and heightened participant anxiety that their cancer could be spreading, prior to treatment commencement. Anne worried that her young age could accelerate the disease's progression. “… the doctor explained that this cancer is more often diagnosed in younger people, and is very aggressive, and spreads fast …that's what happened…from diagnosis to treatment I felt the lump grow” (Anne)
Mothers voiced their apprehension that they would not witness their children's milestones. This prompted them to proceed with plans, despite uncertainty on whether they would survive. The emotional burden of the diagnosis was so overwhelming that Chanelle avoided using the word “cancer,” instead referring to it as the “thing. “Before I received that ‘thing’ [cancer diagnosis], we planned my daughter's birthday party, and then when I was diagnosed with the ‘thing’, my daughter told me, shall we cancel the party? I said no, because I don’t know if this is the last birthday where I will be present.” (Chanelle)
Although a cancer diagnosis brought a profound shift in priorities, it also served as a wake-up call to protect loved ones. Participants emphasized the importance of encouraging relatives to undergo breast cancer screenings, despite state programs often excluding younger individuals. “I tell my daughters to go for screening, but the state services are for those over 50, and my daughters are younger” (Helen)
Alongside their advocacy, participants expressed hope of reaching the 5-year survivorship milestone as the likelihood of recurrence would be then drastically reduced. “He [oncologist] told me that…if I make the 5-year mark, I can consider myself healed.” (Francesca)
Fighting the Aggressive Beast
This GET explores participant experiences of undergoing chemotherapy. Participants viewed chemotherapy as pivotal in confronting TNBC, but some questioned its potency against such an aggressive disease. The rarity of TNBC compounded a sense of vulnerability, as participants rarely encountered others receiving treatment for TNBC in the hospital ward. “Nurses would call out the types of chemo received in the ward…it seemed that I was the only one being treated for TNBC…I was a rare breed in the ward, and this did not augur well in my mind for survival” (Carla).
The rarity of TNBC also hindered participants from identifying TNBC survivors. They expressed that interacting with someone who had successfully overcome TNBC, would inspire hope for recovery and boost their morale during a challenging time. “I wanted to meet a TNBC survivor who had a good quality- of -life. They would inspire me and be a point of reference. But I couldn’t find such a person” (Carla)
Participants also grappled with significant identity shifts, primarily linked to hair loss and breast surgery, which challenged their sense of femininity. Despite wearing wigs, many participants expressed feeling that they had become another person. “I had become a somewhat different person…a different me.” (Carla)
Younger participants voiced concerns about their fertility. “…I don’t know whether I will have another menstrual cycle, since my monthly cycles stopped” (Pauline)
Pulling out the Beast
This GET targets the experiences of participants relating to the surgical procedure. The surgical removal of the tumor was welcomed by all participants, to prevent cancer cells from spreading. Some participants such as Francesca advocated for expedited surgery following chemotherapy, citing the aggressive nature of TNBC. “They scheduled my surgery for a month later, however I wanted it sooner. I told them … I have TNBC and the effects of chemo last for 3 weeks. If we wait longer than that, any remaining cancer cells can spread uncontrollably” (Francesca)
Oftentimes participants were given the choice between a lumpectomy or mastectomy. While some opted for a lumpectomy to preserve breast tissue, others preferred a mastectomy to reduce the risk of recurrence. However, Jean underestimated the full implications of a mastectomy, questioning the impact on her femininity: “It never crossed my mind that they would remove the entire breast. I didn’t expect to see myself looking like this” (Jean)
Others like Pauline, prepared themselves mentally before surgery, comparing the loss of her breast to the experience of losing their hair. “It will take me time, but as humans, we adapt. Same as looking at myself in the mirror. when my hair started to fall out, I got used to it gradually” (Pauline)
Facing the Unknown
This section explores the experiences of participants after undergoing chemotherapy and surgery. Most participants underwent radiotherapy, while 4 participants additionally received immunotherapy. At this stage, preventing a recurrence became the primary focus for participants, who were willing to undergo further treatment with potential side-effects, to increase their chances of survival. “You clutch at any straw to survive. Even though immunotherapy had many side-effects, some serious…I just took the plunge. I didn’t focus on the risks…when those thoughts came to mind, I distracted myself” (Carla)
The participants also expressed that undergoing further treatment improved their chances of remaining present for their families. “The treatment provides me with hope to beat cancer and spend more time with my husband and kids” (Carla)
Participants grew increasingly anxious as their treatment neared completion, as that would imply ever-decreasing contact with healthcare providers. Carla described this transition as akin to a puppet losing its strings, with the strings representing the support provided by professionals. “It is like being a puppet held up by strings. Once treatment ends, the strings are gone and the puppet collapses” (Carla)
Several participants emphasized the importance of connecting with TNBC survivors even in the immediate post-treatment phase, highlighting the value of shared experiences. “There should be a service where survivors can be there for others, so we can talk to someone who truly understands.” (Francesca)
Discussion
This study offers an in-depth exploration of the lived experiences of women diagnosed with TNBC, spanning from initial diagnosis to active treatment. Participants commonly reported high levels of distress, largely attributed to the aggressive progression of TNBC and its tendency to appear at a younger age. Additionally, the study adds to existing literature by highlighting that the rarity of TNBC influences perceptions of reduced survival chances when compared to other breast cancer subtypes.
Living in Shell Shock
Participants described the profound emotional and psychological impact of their diagnosis, often marked by feelings of hopelessness, isolation, and dissociation from reality. To articulate the profound depth of these experiences, participants frequently used metaphors as it enables them to express intricate emotions that might otherwise be difficult to convey directly. 22 For instance, the metaphor voiced by Cala comparing her mind to a “wild stallion” captures the loss of control and cognitive disconnection experienced. In fact, she describes a mind that is “extraneous” to the body, symbolizing a loss of control over thoughts and emotions, that is linked to heightened psychological distress and diminished social functioning and vitality. 23 While the metaphor being “in the clouds” evoked a sense of dissociation and surrealism, that may buffer the initial shock of diagnosis. However, it could also indicate psychological distancing from reality, which may impact commitment to screening and treatment. 24
Existential uncertainty was a common theme, as illustrated by Anne's account of her tumor's rapid growth between diagnosis and commencement of treatment. This highlighted a sense of urgency and anticipatory grief, with participants grappling with the prospect of a shortened life expectancy and diminished quality of life. This awareness of mortality is especially poignant for women with young children, who experience heightened distress from increased health risks and disrupted life goals.5,17 For instance, Chanelle's reference to her diagnosis as the “thing” revealed an implicit avoidance of the term “cancer,” underscoring the burden of her prognosis. Despite this, her decision to celebrate her daughter's birthday emphasized a struggle to maintain normalcy, while acknowledging an uncertain future. This striving to maintain normalcy has also been identified in the study by Post et al 18 and is linked to an improved cancer-related quality of life, alongside enhanced social, functional, psychological, and emotional well-being. 25
The present research contributes to literature, by highlighting that participants also expressed concerns about the genetic implications of TNBC. This motivated them to encourage proactive screening among family members, reflecting a focus on intergenerational health rather than solely individual concerns. One participant, Helen also emphasized the inadequate screening options for younger women and advocated for early, targeted public health policies for families with aggressive cancer histories.
Another significant contribution to the existing literature is the profound sense of isolation reported by participants, primarily stemming from the rarity of TNBC and the limited opportunities to connect with other survivors. This absence of shared experience often left participants feeling vulnerable and unsupported. Supporting this, a study by Post et al¹⁸ found that TNBC patients often felt different from those with other breast cancer subtypes, underscoring the importance of peer support among individuals with TNBC. Such connections not only foster a sense of understanding and solidarity but also facilitate the exchange of personal experiences and practical coping strategies, helping to reduce isolation²⁶ and address the unique challenges posed by this rare and aggressive form of cancer.
Fighting the Aggressive Beast
The aggressive nature of TNBC created an urgency among participants to commence treatment. Many emphasized the need to confront the “aggressive beast” while others questioned the chemotherapy's potency to combat such an aggressive cancer. This internal conflict embodied a blend of hope for a cure, anxiety about the effects of chemotherapy, and fear that the treatment might not control their aggressive cancer. Physical changes posed significant challenges, aligning with the studies of Bollinger 17 and Post et al 18 which found that women with TNBC faced unique challenges due to aggressive treatments, fertility concerns, and the impact on their feminine identity. Since TNBC disproportionately affects younger women, the added burden of fertility issues and the responsibilities of caring for young children further exacerbates their distress, 17 underscoring the need for tailored psychoemotional support. The study by Bollinger 17 also demonstrated that a TNBC diagnosis can also disrupt college, as patients may be unable to attend classes and face financial barriers, such as the inability to pay tuition due to the primacy of medical bills. This aspect was not cited by participants in the present study, and this may be attributed to the availability of state-funded healthcare and education in Malta.
Despite harsh side effects, participants showed resilience, punctuated by moments of despair. In some cases, thoughts of discontinuing treatment surfaced, underscoring the physical and emotional toll of their journey.
Pulling out the Beast
Surgery, often considered a crucial step, brought both relief and emotional conflict. This study demonstrates that the aggressive nature of TNBC increased pressure to expedite surgical decisions. In such scenarios, it is crucial for healthcare professionals to actively listen to patients’ narratives and collaborate with them as equal partners in planning their care. This ensures that patients’ information needs are addressed, fostering a sense of respect and mutual understanding. 27 In those cases where a choice between a mastectomy or lumpectomy was given, participants experienced a sense of control, that enabled them to reshape their identities and find meaning amid a chaotic situation. 28
While concerns about body image were prevalent, various participants viewed a mastectomy as essential to reduce recurrence risk. This finding concurs with the work of Turkman et al⁵ and aligns with the Necessity-Concerns Framework, which suggests that individuals are more likely to adhere to treatment when they believe its benefits outweigh their concerns.²⁹ Despite this, the physical consequences of surgery profoundly impacted participants’ identities, particularly for younger women, as it conflicted with societal images of femininity, 17 and the perception of being too young for such a diagnosis.
Facing the Unknown
The post-surgery phase brought heightened fear of vulnerability and recurrence. Participants dreaded the thought of reduced contact with health professionals. This emphasizes the need for extended follow-up care and psychological support to help TNBC patients’ transition from intensive treatment to long-term surveillance.
Strengths and Limitations
Typical of an IPA study, the study was conducted with a small sample of participants. Consequently, findings cannot be generalized to a wider population. The aim of this study, however, was not to generalize findings but to explore the experiences of females living with TNBC. Additionally, to the authors’ knowledge, this is the first study targeting the lived experiences of women with TNBC, from diagnosis through active treatment.
Conclusion
The experiences of TNBC patients highlight the profound impact of living with a particularly aggressive and rare form of cancer. Participants grappled with anticipatory grief, existential uncertainty, isolation, and the urgent need for treatment, compounded by the difficulty to find support from TNBC survivors. These experiences underscore the importance of ongoing comprehensive psychoemotional care that extends beyond medical treatment. Effective support systems are essential for TNBC patients to navigate their complex journeys, such as specialized mental health services, genetic counseling for patients and their relatives, and accessible peer networks with TNBC survivors. This study further underscores the importance of ongoing post-treatment support for women with TNBC and the need for more inclusive screening policies, particularly for younger populations as Malta's National Breast Screening program currently offers free screenings for persons aged 50 to 69.
Footnotes
Authors’ Note
Informed Consent: Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Acknowledgments
The authors would like to thank Ms Alexis Borg Sapiano and Dr Kristel von Brockdorff, Action for Breast cancer and Europa Donna for their assistance in the recruitment process and the study participants who shared their experiences. The authors would also like to thank Prof Carmel Cefai for assistance in funding acquisition.
Author Contributions
JS, JA, and MG: study concept and methodology; JS and JA: formal analysis; JS: data collection; JS and JA: writing—original draft; JS, JA, and MG: writing—review and editing; JS and MG—funding acquisition. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
All procedures in this study were conducted in accordance with the Faculty of Health Sciences Research Ethics Committee, University of Malta (Approval number: FHS2022-00338) approved protocols.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a peer-reviewed grant from the Alive Charity Foundation through the Research, Innovation, Development and Trust fund University of Malta. The funders did not play any role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.