
Abstract
Healthcare systems are rapidly transitioning toward patient-centered models, however, there is limited data regarding this from low- and medium-income countries. This cross-sectional study included patients above 18 years, admitted to internal medicine services at 2 tertiary care hospitals in Karachi, Pakistan. The outcome was a patient experience, with independent factors including sociodemographic characteristics (age group, gender, education level, and financial status) and hospital stay-related factors (admission type, length of hospital stay, attending physician's academic designation, functional status, code status, number of consults, and number of surgical and radiological procedures). Among 499 patients, the mean (standard deviation) patient experience score was 44.1 (4.5). Multivariable regression analysis showed higher scores (>45) were associated with factors such as, >16 years of education (OR = 1.6, 95% CI, 0.7-3.9), higher physician academic rank (OR = 4.5, 95% CI, 2.0-9.8 for Associate Professors and OR 12.1, 95% CI, 6.6-22.1) more radiological investigations (OR = 1.3, 95% CI, 0.3-1.8) and undergoing surgical procedures (OR = 2.1, 95% CI, 0.8-5.8). Lower scores (<45) were associated with semiprivate ward admissions, patients with a functional level of II, and a higher number of consults. Overall, the study showed a good patient experience score. However, disparities exist, emphasizing the need for policies to improve patient awareness, physician training, and equitable care for all of those with functional limitations.
Keywords
Introduction
Patient experience encompasses the entirety of interactions individuals have within the healthcare system, including care received from doctors, nurses, and other healthcare facilities. 1 As healthcare systems increasingly prioritize patient-centered care, there has been a growing emphasis on measuring patients’ perceptions of the quality of care. This is because good patient experience is positively associated with clinical effectiveness and influences patient behavior, such as adherence to medication, use of screening services, and resource utilization. 2 This underscores the importance of considering patient experience as a central pillar of healthcare quality, 3 which is a particularly ignored entity in many hospital settings from low- and medium-income countries and is not measured often due to a lack of resources.
In comparison to developed countries, the utilization of patient experience indicators in low-income nations has been minimal, as resource limitations in these settings have directed attention more urgently toward ensuring the provision of fundamental supplies and services rather than emphasizing quality in patient experiences. 4 However, some similar studies have been carried out in other lower-middle-income nations.5,6 For instance, a study by Adhikari et al 7 conducted in a Nepalese outpatient department revealed that 39% of patients reported higher experience scores and were more satisfied with the healthcare in the community. A systematic review by Batbaatar et al 8 examined 109 studies investigating determinants affecting patient experience scores. It revealed that individual characteristics, including age, gender, educational status, religion, race, and marital status, play significant roles in shaping patient experiences. 8 Various methods, including surveys, interviews, and focus groups, measure patient experience. 9 The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a key component of Consumer Assessment of Healthcare Providers and Systems, has become the standard method for assessing adult inpatient experience in the United States 10 and has been adopted and utilized in numerous countries worldwide. 11 The HCAHPS survey collects feedback from discharged patients via 27 questions, assessing various aspects of their hospital experience. 12
It is unclear how patients in an existing healthcare setting from a lower to middle-income country such as Pakistan perceive healthcare quality and what factors most impact their experience. In Pakistan, most of the healthcare system is not insurance-based, and patients are often paying out of their pocket, and have higher demands from healthcare compared to other healthcare systems such as in the United States or Europe. 13
Given these gaps, our research seeks to thoroughly investigate patient experience using the HCAHPS survey. Through applying the HCAHPS survey in this setting, our goal is to acquire insight into any distinct challenges linked to patient experience. The study aims to measure patient experience and factors associated with it using the HCAHPS survey among patients admitted to internal medicine services at 2 tertiary care hospital settings in Karachi, Pakistan. By measuring patient experience and its associated factors, we may be able to take measures to improve patient experience in hospitals.
Methods
This cross-sectional study was carried out from 2022 to 2023, on patients admitted to the medicine unit of 2 tertiary care hospitals at the time of discharge. The study was conducted after acquiring ethical clearance from the Ethical Review Committee (ERC), Aga Khan University (2022-6761-20342), and ERC Ziauddin Hospital (5820822UGMED). This study included all patients aged 18 years or above with a nonpsychiatric principal diagnosis at discharge, who stayed at least 2 days in the hospital and were alive at the time of discharge. Those with a home address outside Pakistan were excluded from the study. Also, those who were discharged from specialized care facilities such as nursing homes were excluded.
HCAHPS Survey
The HCAHPS survey comprises 27 items organized into 22 questions and 5 demographic queries. Among the 22 questions, 18 address critical aspects of the hospital experience while 4 are screening questions. Among the 18 questions, 16 pertain to recent hospital experiences, evaluating eight domains: “communication with nurses,” “communication with doctors,” “staff responsiveness,” “pain management,” “communication about medications,” “discharge information,” and “cleanliness and/or quietness.” Additionally, there are 2 global rating items for overall hospital rating and willingness to recommend the hospital. 14 The questionnaire employs various response scales, including a dichotomous scale (1 = yes, 2 = no), a global rating scale (0 = worst to 10 = best), and a 4-point Likert scale (1 = never, 2 = sometimes, 3 = usually, and 4 = always). The questionnaire demonstrates good factor loading values and internal consistency reliability, as evidenced by Cronbach's alpha of 0.69 during its development process. 15
Variables
The main outcome variable is patient experience as measured by HCAHPS. The independent variables for the study comprised sociodemographic factors (age group, gender, education level, and accommodation type) and hospital stay-related factors (admission type, length of hospital stay, academic designation of attending physician, functional status, code status, number of consults, and number of surgical and radiological procedures).
Demographic variables included age, classified as >65 years and <65 years, and gender, encompassing male and female categories. Educational level was categorized based on years of education: not educated (lacking formal education), <8 years, 8-16 years, and >16 years.
The type of accommodation requested by the patients was taken as a surrogate for financial class categorized as general ward admission as level 1, semiprivate as level 2, and private as level 3 (with 3 being high). These 3 levels of accommodation are such that the cost of the general ward bed is the lowest and the private bed is the highest, hence patients get admitted based on their affordability.
The academic designation of attending physicians was categorized into four levels: Senior Instructor, Assistant Professor, Associate Professor, and Professor. Admission sources indicated whether patients were admitted directly from the emergency room or through scheduled or elective procedures.
The functional status of patients was used to categorize patients into four classes based on physical activity and associated symptoms, ranging from Class I (no limitations to mobilize) to Class IV (severe limitations to mobilize). Code status refers to patient directives during cardiac or respiratory arrest. 16 The full code indicates a desire for all life-saving measures, including cardiopulmonary resuscitation. Do not resuscitate (DNR) pharma declined resuscitation but allowed pharmacological interventions. DNR comfort also declined resuscitation, prioritizing comfort-focused care. 17
Other variables included the number of consultation services, the number of surgical and radiological procedures performed, and the mean length of stay in the hospital. A sample size of 268 patients was required to assess patient experience based on a mean overall hospital score of 85 reported in a previous study, with a standard deviation (SD) of 15 and an alpha error of 0.05.
Statistical Analysis
Mean (SD) was calculated for quantitative variables, while frequency and percentage were calculated for categorical variables. Logistic regression assessed associations between factors and patient experience, reporting odds ratios (ORs) and 95% confidence intervals (CIs). The patient experience score was dichotomized into 2 categories based on a median score of 45, which indicates satisfactory patient experience. To the best of our knowledge, we did not find any cutoff in the score that could be designated as good or optimal patient experience, hence we used the median as cutoff to categorize into acceptable and not acceptable patient experience. Model 1 has age and gender as explanatory variables with patient experience of >45 as an outcome variable. Model 2 is adjusted further for educational level and financial class. Model 3 is additionally adjusted for educational level and financial class, code status, functional class, and length of stay, and Model 4 is adjusted for educational level and financial class, code status, functional class and length of stay, admission source, number of consults, surgical procedures and number of radiological procedures. Multiple linear regression was also conducted as a sensitivity analysis to assess the robustness of the findings and has been shown as Supplementary Table S1. Dummy variables were created for independent variables with more than 2 categories.
Results
A total of 600 patients were approached out of which 499 (80%) agreed to participate in this study, all of whom were admitted to the medicine unit of Aga Khan University Hospital (N = 350) and Ziauddin Hospital (N = 149). Among the participants, 261 (52.3%) were male, 334 (67%) were aged 65 or older, with 279 (55.9%) having 8-16 years of education. Precisely, 246 (49.3%) were admitted to private wards, and the emergency room was the main admission source for 470 (94.2%) of patients. Furthermore, 238 (47.7%) of attending physicians were Professors or Associate Professors. Almost 480 (96.2%) patients were designated as full code. The mean (SD) hospital stay was 4.8 days (2.6). This has been presented in Table 1.
Baseline Characteristics of Patients Admitted to Internal Medicine Service at the 2 Hospitals.

Patient Experience Score
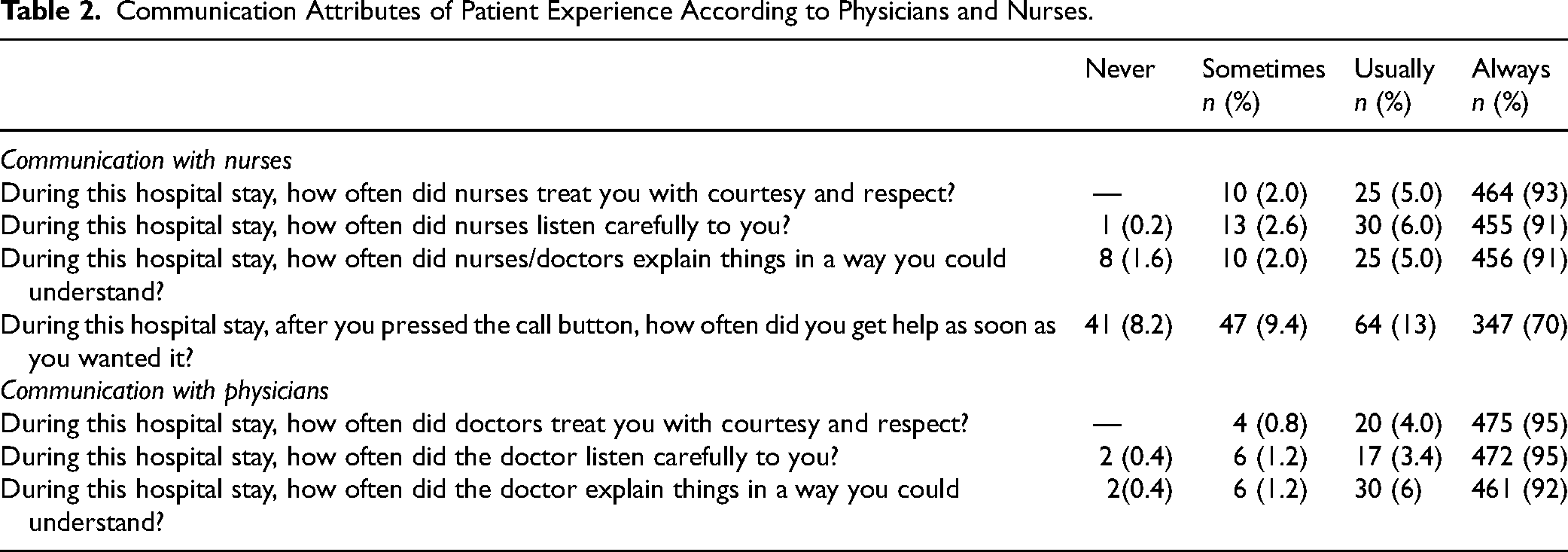
The mean (SD) patient experience score was 44.1 (4.5), and Supplemental Figure S1 shows the patient experience scores in percentiles of patients. The patient experience score was categorized into 2 categories based on a median score of 45, considered acceptable for patient experience. The patient experience score ranged from 28 to 50, with 232 (53.5%) scoring more than 45 on the scale. The assessment of communication attributes of patient experiences with nurses and physicians revealed high levels of satisfaction in several key areas. Patients overwhelmingly reported always being treated with courtesy and respect by both nurses (464 (93.0%) and physicians (475 (95.2%)). Additionally, a large majority of patients indicated that nurses 455 (91.2%) and physicians 472 (94.6%) always listened carefully to them. Patients also reported high levels of understanding from both nurses 456 (91.4%) and physicians 461 (92.4%) when explanations were provided. However, responses varied regarding response times to call button presses with nurses, with 347 (69.5%) of patients reporting always receiving help as soon as desired while 41 (8.2%) reported a delay in responding to call bells. The results have been presented in Table 2.
Communication Attributes of Patient Experience According to Physicians and Nurses.
Factors Associated with Acceptable Patient Experience Score (>45) Admitted to Internal Medicine Service
On univariate analysis of factors associated with patient experience of >45 were: education level ranging 8-16 years (OR = 2.4, 95% CI, 1.2-4.7), undergoing more than 16 years of education (OR = 4.0, 95% CI, 1.9–8.3), senior academic designation (Associate Professor and above) (OR = 5.1, 95% CI, 2.5-10.5), and undergoing a higher number of radiological investigations (OR = 2.11, 95% CI, 1.65-2.7) were associated with a patient experience score of (OR = 2.11, 95% CI, 1.65-2.7) > 45. The findings are presented in Table 3.
Factors Associated With Patient Experience Score >45 in Patients Admitted to a Hospital Setting.

Table 4 presents the results of the multivariable analysis, where several factors were examined for their association with patient experience exceeding 45 among those admitted to the Internal Medicine service. Among these various factors, more than 16 years of education (OR = 1.6, 95% CI, 0.7-3.9), higher academic designation of physician (OR = 4.5, 95% CI, 2.0-9.8 for Associate Professors and OR 12.1 95% CI, 6.6-22.1) patients undergoing a higher number of radiological investigations (OR = 1.3, 95% CI, 0.3–1.8) and undergoing surgical procedures (OR = 2.1, 95% CI, 0.8-5.8) were associated with a patient experience score of >45 in the final model.
Factors Associated With Patient Experience Score of ≥45 in Patients Admitted to Internal Medicine Service.

*Model 1 adjusted for age and gender.
**Model 2 adjusted for age, gender, educational level, and financial class.
***Model 3 adjusted for age, gender, educational level, financial class, code status, functional class, and length of stay.
****Model 4 adjusted for age, gender, educational level, financial class, code status, functional class, length of stay, and admission source, Academic designation of attending physician, number of consults, number of surgical procedures, and number of radiological procedures.
Conversely, patients admitted to semiprivate wards (OR = 0.4, 95% CI, 0.2-0.7), patients with a functional level of II (OR = 0.6, 95% CI, 0.2-1.4), and an increased number of consults involved (OR = 0.9, 95% CI, 0.7-1.2) were associated with a patient experience score <45 in the final model. Similar models were created using multiple linear regression using patient experience as a continuous outcome (Supplemental Appendix). The final models showed that a higher academic rank of admitting physician was associated with a higher patient experience score; β = 0.2 (95% CI, 1.7-4.4) for Associate Professor and β = 0.5 (95% CI, 3.4-5.3) for Professor (R = 0.57)
Discussion
Our study, conducted in 2 tertiary care hospitals in Karachi, Pakistan, found that 53.5% of patients had acceptable patient experience scores above 45. Higher education levels (8-16 years and more than 16 years), senior academic physician designation, and greater radiological investigations were associated with higher patient experience scores. Conversely, patients admitted to semiprivate wards, those with a functional level of II, and those involved in increased consultations had lower patient experience scores.
Numerous studies have explored how sociodemographic factors influence patient experience scores. A systematic review of 24 articles explored factors influencing patient experience and found that individual factors such as health status and education were found to positively impact patient experience, while characteristics such as younger age, lower education levels, lower socioeconomic status, marital status, poorer health, and higher service utilization were associated with lower satisfaction. 18 However, specific population studies, such as one in Nepal, identified a significant association between factors such as age, gender, and education level with patient experience scores. 7 In contrast to our study's findings, which showed no significant relationship between age and gender and patient experience scores, we observed a positive association between higher education levels and enhanced patient experience scores. One possible explanation for individuals with higher education levels having higher patient experience scores could be that they were able to understand the questions more in the survey and felt the responsibility to express their opinions while being aware of the constraints within the health system doctor–patient/attendant communication was more meaningful with patient/attendants who were more educated and they were able to understand some if not all medical terminologies while those who were less educated had trouble understanding and hence scored lower. This could improve communication among physicians.
In the study by Nabbuye-Sekandi et al, 19 there was a positive relationship between having primary or secondary education and higher levels of satisfaction (mean = 2.8) compared with no education (mean = 2.3) and postsecondary education (mean = 2.3). However, several different studies reported different influences of education on patient experience scores, a study by Asamrew et al 20 found no significant correlation between education levels and patient experience scores. Several other studies have similarly found that individuals with education up to secondary school or possessing diplomas or higher qualifications tended to report lower patient experience scores compared to those with no formal education.21,22 In contrast to previous findings, our study revealed an association between education levels and increased patient experience scores. The study noted that individuals with higher education were inclined to report higher scores, this could be because these patients are more aware of the constraints within the health system. As a result, receiving care that meets or exceeds their expectations could lead to higher levels of satisfaction.
We found a positive association between the number of radiological investigations undergone by patients and their likelihood of reporting a satisfactory patient experience score (>45) (OR = 2.11) on univariate analysis, but the association weakened in the final model. However, this suggests that patients who received more extensive radiological evaluations tended to perceive their overall hospital experience more positively. Possible explanations for this association could include patients feeling that thorough radiological assessments contribute to a more objective assessment and diagnosis of disease, and they interpret multiple investigations as indicative of thorough diagnostic evaluation, leading to increased confidence in their healthcare providers and increased satisfaction with the healthcare provided. No specific study has explored this association in detail. However, one study assessed patient experience scores among 43 patients, finding a median score of 4 out of 5 (with 5 indicating the highest level of satisfaction) regarding their experiences with magnetic resonance imaging and ultrasound procedures. 23 Thus, further research may be needed to confirm these findings. We also found that those medicine patients who undergo surgery were more satisfied, although this did not reach significance as in most patients of medicine surgeries are not indicated. Hence this is of less relevance, although this does highlight that when patients undergo curative treatment it gives a sense of satisfaction to patients and their families.
While patients generally provided positive feedback regarding their interactions with physicians and nurses, there was a notable divergence in opinions regarding the promptness of nurse responses to call button activations, with 8.2% of respondents citing delays. This issue is directly linked to the timeliness with which nurses address patient inquiries and emerges as the sole aspect where satisfaction levels were comparatively lower. Interestingly, past research has yielded varying findings on this matter. For instance, Koc et al's 24 study, encompassing 4266 patients found that the highest satisfaction was recorded in the category “How quickly nurses came when you called for them". Similarly, Buchanan et al's 25 investigation, which focused on 142 patients in an urban teaching hospital in Jamaica, identified one of the top three satisfaction items as the promptness with which nurses responded to patients’ calls. These disparities in findings suggest that factors influencing patient satisfaction with nurse responsiveness may vary across different healthcare settings and populations. Particularly focusing on Pakistan's healthcare system, this finding may be influenced by factors such as workload, staffing ratios, organizational efficiency, and cultural expectations unique to the region. Specifically, the nurse-to-patient ratio plays a critical role in determining the promptness of nurse responses as we also report that patients with functional limitations were more likely to score <45 for patient experience. In settings with lower nurse-to-patient ratios, nurses may face challenges in prioritizing tasks, leading to delays in responding to patient calls, which can increase patient dissatisfaction. 26 Another potential reason could be that most patients admitted to these tertiary care hospitals are multimorbid, which increases their dependency on nurses.
In a systematic review, it was found that among the 5 studies analyzed, 2 (40%) showed a positive or partially positive correlation between physicians’ clinical experience and outcome measures associated with patient-centeredness. Conversely, 3 studies (60%) did not find any significant association between these variables. 27 In our study, we observed a comparable outcome, wherein we noted an improvement in patient experience scores as the physician's seniority designation increased. This result suggests that experienced physicians may have better communication and diagnostic skills, which helps them provide better experiences for their patients. This probably suggests that junior faculty should shadow senior faculty for some time before being independent consultants, and in their junior years should consider consulting seniors in complex patient management.
While our study provided valuable insights into patient experience within Pakistan, certain limitations must be acknowledged. The study has a sample size of 600, however, it is not representative of the entire population's patient experience score, which limits the generalizability of this study's findings. Even though the study was conducted in 2 tertiary care hospitals in Karachi, this does not reflect the experiences of patients in smaller healthcare facilities, rural areas, or public sector hospitals, either within Pakistan or internationally. However, the findings can be generalized to private tertiary care setups across Pakistan. Additionally, the cross-sectional design limits our ability to establish causal relationships between patient characteristics and experience. Finally, the study utilized a self-reported survey to calculate the patient's experience score, which can introduce a potential response bias due to several reasons such as recall errors, personal expectations, and social desirability bias, which limits the validity of the results. Also, patient experience is dependent on various factors such as timely appointments, good communication with healthcare providers, care coordination, shared decision-making, self-management support, culturally appropriate care, etc., which was not considered in our study. However, despite the limitations, it utilizes the standardized HCAHPS survey, ensuring consistency, and by including 2 tertiary care hospitals in Karachi, Pakistan, the study's findings can be generalized to similar healthcare settings in the region. It also provides a foundation for future research and policymakers and healthcare providers to enhance patient-centered care, improve hospital practices, and address the factors leading to disparities in patient experience. Future research that employs interventions to improve patient experience is needed to yield more definitive causal conclusions.
Conclusion
Our study in 2 tertiary care hospitals in Karachi, Pakistan shows acceptable patient experience with physicians and nurses. Higher patient education levels and care by senior academic physicians positively influenced experience scores while those patients admitted to semiprivate wards or with a functional level of II reported suboptimal experiences. The findings from this study suggest that patient experience should be measured using simple questions or alternative methods for assessment of patient experience in our setting as nurses are an integral part of healthcare, and enough experienced nurses need to be maintained to improve patient experience. Junior faculty should shadow senior faculty for some time before becoming independent consultants and consider consulting seniors in complex patient management. These findings also highlight how there is a need for policies to enhance doctor–patient communication, patient engagement, and nursing in both public and private healthcare sectors. On an international scale, there should be development for patient-centered models, especially in lower-middle income countries, that are aimed at ensuring better healthcare quality and even distribution of healthcare among the population. While our research particularly highlighted factors that affect patient experience, however, it is limited to private healthcare sectors thus it is important to have studies being conducted in the public healthcare settings, which can help in devising policies for everybody's benefit.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251342118 - Supplemental material for Factors Associated With Patient Experience From 2 Tertiary Care Hospitals—A Cross-Sectional Study From Karachi, Pakistan
Supplemental material, sj-docx-1-jpx-10.1177_23743735251342118 for Factors Associated With Patient Experience From 2 Tertiary Care Hospitals—A Cross-Sectional Study From Karachi, Pakistan by Aqsa Amjad, Zaibun Nisa, Sana Javed Khan, Sania Sabir Sethi, Asmara Ghafoor, Anoosha Iqbal, Farheen Shahzad, Mehmood Riaz, Uzma Ghori and Aysha Almas in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251342118 - Supplemental material for Factors Associated With Patient Experience From 2 Tertiary Care Hospitals—A Cross-Sectional Study From Karachi, Pakistan
Supplemental material, sj-docx-2-jpx-10.1177_23743735251342118 for Factors Associated With Patient Experience From 2 Tertiary Care Hospitals—A Cross-Sectional Study From Karachi, Pakistan by Aqsa Amjad, Zaibun Nisa, Sana Javed Khan, Sania Sabir Sethi, Asmara Ghafoor, Anoosha Iqbal, Farheen Shahzad, Mehmood Riaz, Uzma Ghori and Aysha Almas in Journal of Patient Experience
Footnotes
Authors Note
All authors approved the final version of the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. The lead author Aysha Almas affirms that the manuscript is an honest, accurate, and transparent account of the study being reported and that no vital aspects have been excluded.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
ERC approval was obtained from the ERC, Aga Khan University (2022-6761-20342), and the ERC Ziauddin Hospital (5820822UGMED). Respondents gave written consent before starting to fill out the survey.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.