
Abstract
Increased stress, anxiety, and depression hinder recovery of hospitalized patients. Mindfulness therapies, which adopt a holistic approach to patient care, reduce anxiety, and depression. This quality improvement initiative evaluated the implementation of a virtual reality (VR) therapeutic art program at Stanford Health Care from February to June 2024, providing an innovative and scalable adjunct to traditional art and music mindfulness therapies. This mixed methods project piloted 84 cumulative hours with 105 participants. Outcomes investigated satisfaction and the impact on hospitalization experience via survey questions. Data were analyzed using descriptive statistics and thematic analysis. Results (n = 40) indicated substantial improvements in patient experience, with 85% recommending the program and 97.5% reporting positive impacts from VR engagement. Thematic analysis of open-ended survey responses identified 4 key themes: escape and distraction, therapeutic benefits, enjoyment of the interactive activity, and positive facilitator interactions. Participants also expressed interest in additional VR offerings, including virtual mindfulness, and meditation. The results suggest that VR can serve as an effective adjunct to conventional mindfulness therapies and improve the inpatient experience.
Plain Language Summary
Why was the project done?
Anxiety and depression slow the recovery of hospitalized patients. Mindfulness therapies help, but access is often limited. This project evaluated a virtual reality (VR) therapeutic art program to improve the patient experience.
What did the researchers do?
From February to June 2024, 105 patients participated in the program, engaging with art through VR. Researchers collected feedback to assess the impact of VR on patient experiences.
What did the researchers find?
Out of the 105 participants, 40 completed the full VR experience and survey. And 85% recommended the program and nearly all 40 (97.5%) reported that the VR experience positively affected their hospital stay. Key themes from their feedback included:
Participants also showed interest in expanding VR offerings, such as virtual mindfulness and meditation.
What do the findings mean?
The project indicated that VR enhanced patient satisfaction and wellbeing during hospital stays. Future directions include expanding VR training with other therapeutic art facilitators to facilitate patient access to these therapeutic tools.
Introduction
Increased stress, anxiety, and depression hinder recovery of hospitalized patients.1–3 Patients in the top 50% of Hospital Anxiety and Depression scores are 4 times more likely to experience delayed healing. 1 Addressing these psychological conditions through accessible interventions is critical. Holistic therapies, like mindfulness, promote nonjudgmental awareness and openness, reducing anxiety and depression for 3 weeks to 3 years.4,5 Art-based mindfulness interventions also enhance self-expression and learning.6,7 Hospital-based, mindfulness approaches often rely on one-on-one therapist-patient models, limiting accessibility.
Therapeutic virtual reality (VR) art applications immerse patients in self-soothing, computer-generated environments for engagement in creative expression, presenting a feasible and scalable adjunct to traditional therapies. VR can reduce depression and anxiety through immersive meditation, mindfulness training, and virtual nature exposure.8–10 Commercially available VR have modest costs and can be philanthropically sourced.11,12 These devices are designed for consumer use, enhancing their potential to broaden access independent of dedicated specialists.
This project implemented VR-based therapeutic art within the Stanford Office of Patient Experience and evaluated patient satisfaction and participants’ VR experience in an effort to design a reproducible framework.
Methods
Context
This quality improvement project was conducted at Stanford Health Care (SHC), a 600-bed academic, quaternary care hospital in Northern California. The Stanford Creative & Healing Arts (CHA) program serves over 2400 hospitalized patients monthly with the mission of integrating arts with healthcare for patient wellbeing. The CHA VR art program was piloted between February 26 and June 10, 2024.
Intervention
During an Art Program evaluation, the CHA team identified a need for adaptive art tools for patients unable to engage in traditional art forms, for example, those who could not use their extremities due to surgery or burns. VR art was implemented as a scalable alternative to enable meaningful participation. Evaluation and referral processes aligned with existing inpatient art and music programs (Supplemental Appendix A1). To improve efficiency, weekly unit rounds and huddle guides detailing program criteria were created (Supplemental Appendix A2).
English-speaking patients were approached for participation. Exclusion criteria for program engagement included history of uncontrolled seizures, severe motion sickness, current nausea, acute visual problems, isolation, facial trauma, facial burns, and those who were not clinically stable. Referrals were managed through the Voalte smartphone application (Sarasota, FL). Upon arrival at a patient unit, the VR facilitator consulted the charge nurse regarding that day's referrals and subsequently provided VR services. The order was determined via urgency of the request, defined as the need for acute anxiety relief, for example, if the patient was in distress and there was a need for nonpharmacological anxiety relief, such as an impending procedure. VR headsets (Quest 3, Meta, Inc., Menlo Park, CA) were cleaned with Sani Cloth AF3 (PDI, Woodcliff Lake, NJ) before and after each use. Applications included Tilt Brush (Google, Mountain View, CA) and Color Space (Lighthaus, Los Angeles, CA), during sessions that were offered from 10 AM to 1 PM, Monday through Friday. Following participation, facilitators invited patients or their family members to complete a brief, confidential survey via a QR code linked to Qualtrics XM (Qualtrics, Seattle, WA). Since this was a quality improvement project, no formal Institutional Review Board consent was required. Surveys were sent to all patients who were offered VR, regardless of whether they completed the VR experience.
Intervention Evaluation
Patient experience (PX) survey questions were standardized in collaboration with the SHC PX Data Analysis and Reporting team (Supplemental Appendix A3). Additional questions identified VR users. Weekly reviews of survey responses facilitated continuous program improvement.
Outcomes and Measures
Patient satisfaction was evaluated via a “Likelihood to Recommend” (LTR) scale with 5 options: very likely, likely, neutral, unlikely, and very unlikely. We also explored impact on hospital experience through a binary yes/no question, and patient experiences of VR therapeutic art, evaluated through thematic analyses of open-ended responses to: “What did you experience?” and “Please let us know if you have any additional comments about the program that will continue to make this program great for other patients.” 13
Analysis
Categorical data for LTR and impact on hospital experience were analyzed using percentages. Qualitative data for the open-ended questions were analyzed using Excel (Microsoft, Inc., Redmond, WA) and Stanford School of Medicine Secure ChatGPT. Caregiver and participant results were analyzed equivalently given the questions were directed to the patient and the patient invited their caregiver answers. For qualitative responses, authors SM, RP, VGP, and ChatGPT reviewed all patient responses, generating themes inductively individually. Themes produced by each author and Secure ChatGPT were discussed and refined following principles of a thematic analysis until consensus was reached. 13 To validate findings, facilitators then reviewed the analyzed contents and unanimously agreed that it accurately represented participants’ sentiments.
Results
Participants
The project piloted for 84 h, involving 105 individuals, with 56 completing surveys (53.33%). Among survey respondents, 40 of 56 (71.42%) used VR for the entire duration. Reasons for incomplete use (n = 16) included feeling overwhelmed or unspecified. Four respondents were family members who reported positive experiences, noting that their relative using VR appeared relaxed. Most 51 of 56 (91.1%) were first time participants, with 3 having participated 1 to 2 times and 2 participated 3 to 4 times (Figure 1).
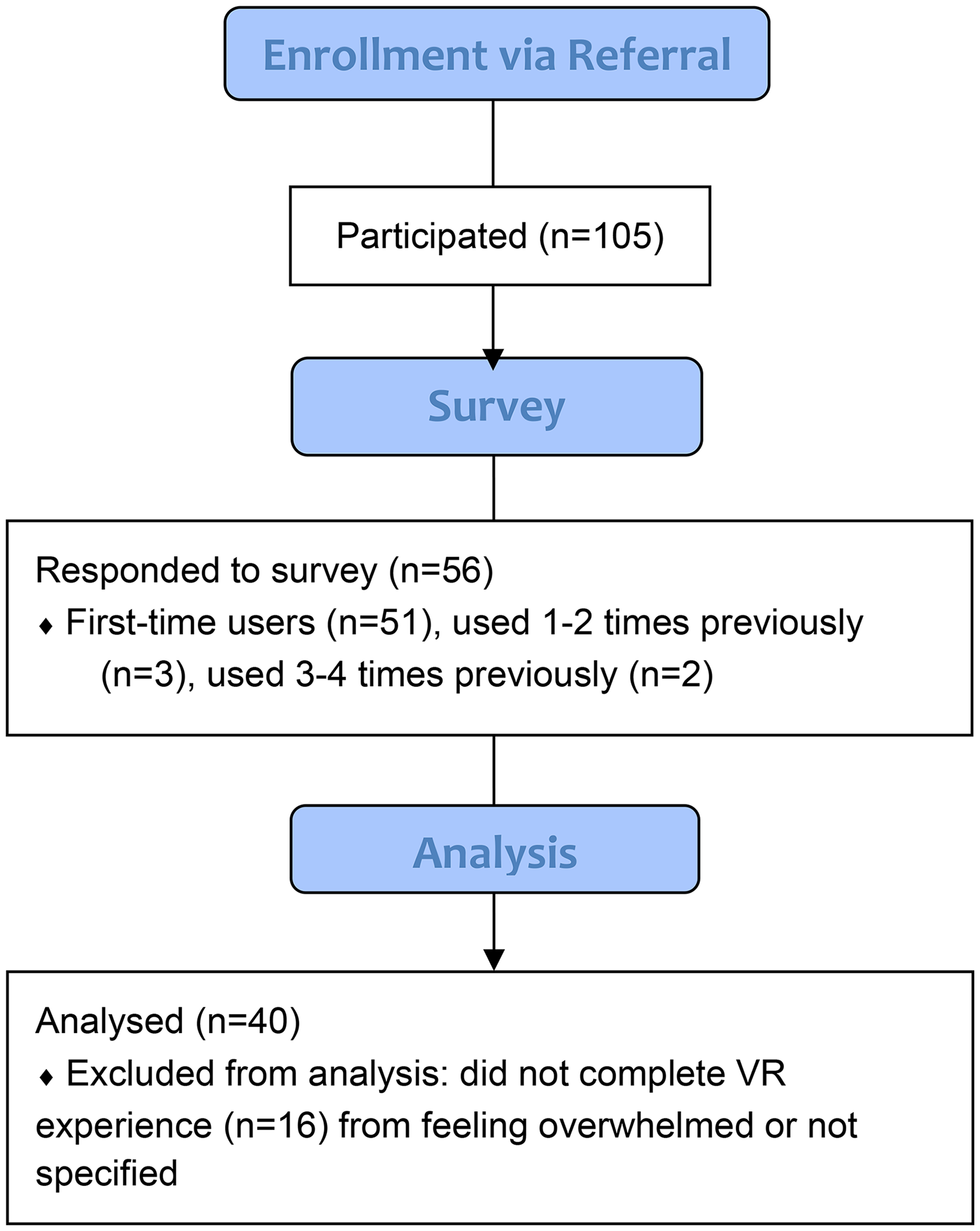
CONSORT flow diagram of participant enrollment, survey response, and analysis.
Patient Satisfaction and Experience
Of the 40 participants who completed the VR experience and the LTR survey, “How likely are you to recommend this program to another patient?”, 34 (85%) reported “very likely.” When asked “Did participating in this service have an impact on your time at the hospital?”, 39 of 40 (97.5%) said “yes.” Participants also displayed interest in other VR offerings: 6 for “Virtual mindfulness and meditation,” 11 for “Virtual traveling and exploring,” and 2 interested in “other” unspecified.
Open-ended responses indicated gratitude for the program, with 4 main themes: escape and distraction, therapeutic benefit, enjoyment of the interactive activity, and positive interaction with the facilitator.
For Escape and Distraction, participants described the activity as an escape from the hospital environment, providing distraction from their medical concerns. “I felt I was in a different place than the hospital. I can paint in an endless world; I like the crazy things you can draw.” “Definitely took our minds off of the waiting that we were doing for the heart transplant.”
For Therapeutic Benefit, participants found the VR calming, therapeutic, and beneficial to their wellbeing. “My stomach pain went away for a little bit. The scenery was beautiful. Thanks!” “The value of this program is the power that it has to alleviate stress.”
For Enjoyment of the Interactive Activity, participants enjoyed the interactive VR art, finding it fascinating and engaging, noting the variety of colors and sound and the ability to manipulate them. “I had a great time, I love painting.” “So many colors! It was beautiful. I enjoyed the beauty of the bright colors.”
For Positive Interaction with Facilitator, several comments reflected appreciation for the facilitator's guidance, helpfulness, and kindness throughout the activity. “[Facilitator name] was amazing” “Wow, she was amazing and her teaching me how to use it. She took the time to explain everything. She was very kind and I really enjoyed the class.”
For program improvement or expansion, 2 themes were synthesized: desire for more access and time with the activity, and suggestions for additional features. For Desire for More Access and Time with the Activity, some participants expressed a desire for increased time with VR, suggesting the ability to check it out for longer periods. “It would be interesting to be able to check them out from the nurses’ station for a few hours at a time. Thank you so much! It's the most fun I’ve had in a while.” “Just keep expanding it…It's power to be a blessing to others are all reasons to give this more attention and backing.” For Suggestions for Additional Features, comments expressed interest in additional features like meditation videos and music studio applications. “More meditation videos.”
Discussion
This VR program highlighted VR as a meaningful escape that provided distraction from medical concerns for the majority of participants. Therapeutic benefits included increased happiness and relief from discomfort, with participants appreciating the interactive nature of VR art and facilitators’ support. Suggestions for improvement included extending access to the VR experience and adding features such as meditation and music studio applications, reflecting a desire for enhanced engagement during hospital stays.
The connection between VR use and patient satisfaction supports previously reported therapeutic outcomes related to reduced stress and improved mood.14–16 VR's ability to provide escape and distraction is linked to its real-time reorientation capabilities and cognitive load modulation. 17
This project's strengths lie in its effective hospital implementation strategy. By detailing weekly unit rounds, huddle guides, and handouts of program criteria, other healthcare institutions can utilize this framework to plan and execute (Supplemental Appendices A1 and A2). To replicate this work, other institutions need technical and sanitary equipment (for example, VR headsets and sanitizing cloths), facilitators who understand patients’ indications for anxiolytic VR, and abidance with safety protocols. To scale this intervention in limited resource settings, headsets and resources can be sourced through nonprofits such as Invincikids (Invincikids, Inc., San Bruno, CA). Items that can be readapted by other hospitals include involvement of the Charge Nurse, manager, or other health professionals depending on availability and roles of each staff, amount of time patients engage in VR, presence of a screencasting device based on availability of technology, and location and room details. Hospital teams should establish a communication method and framework that enables best patient care and safety at their institution.
Limitations
Similar to other improvement projects, this initiative lacked a control group, preventing conclusions about noninferiority to traditional art mindfulness therapies. Although anonymous surveys encouraged candid feedback, absence of demographic data limited the ability to assess participation bias and trends in accessibility. Additionally, despite a facilitator assisting with use, the technological learning curve inherent to adoption of new technologies may have hindered some participants from fully engaging with VR. Survey compliance was similar in this project compared to the response rate from other Arts and Wellness surveys, but future studies would benefit from increased compliance. All patients also received a standard set of survey questions regardless of how they heard about the program, so this may have biased results in an unknown direction. Furthermore, the study was conducted at a single, well-resourced hospital, limiting generalizability to low-resourced settings.
Conclusion
VR therapeutic art enhanced patient experiences during hospital stays, providing therapeutic benefits and positive emotional impacts. Incorporating VR therapeutic art into standard patient care facilitates a holistic approach that addresses physical, emotional, and psychological needs to improve outcomes and patient satisfaction. Future directions involve training more staff to provide VR upon request, enabling patients to access VR experiences directly in their rooms outside of typical art therapist service hours, and incorporating control groups in future studies to strengthen validity. Future studies will also investigate program impact on patient recovery parameters, such as recovery time and duration of benefits.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251330467 - Supplemental material for Virtual Reality Therapeutic Art for Adult Hospitalized Patients and Caregivers: A Mixed-Methods Project
Supplemental material, sj-docx-1-jpx-10.1177_23743735251330467 for Virtual Reality Therapeutic Art for Adult Hospitalized Patients and Caregivers: A Mixed-Methods Project by Sophina McDaniel, Rachyl Pines, Emily M. He, Faith Collins, Faaizah Arshad, Maria Menendez, Vishnunarayan Girishan Prabhu and Thomas J. Caruso in Journal of Patient Experience
Footnotes
Acknowledgments
Our team would like to acknowledge the leadership and staff at Stanford Health Care and Stanford Medicine, our generous art program donors, and our virtual reality facilitator, Michelle Doan. We would also like to acknowledge the support of the Stanford Chariot Program, Amanda Casillas, Director Service Excellence, Mysti Smith-Bentley, Executive Director Service Excellence, and Alpa Vyas, Senior Vice President, Chief Patient Experience & Operational Performance Officer.
Authors’ Contributions
SM was involved in conceptualization, methodology, investigation, data curation, writing—review & editing, and visualization; RP in conceptualization, methodology, investigation, and writing—review & editing; EMH in writing—original draft, writing—review & editing, and visualization; and TJC in conceptualization, methodology, software, resources, writing—review & editing, supervision, project administration, and funding acquisition.
Declaration of Conflicting Interests
TC is on the board of a nonprofit (Invincikids, Inc), that seeks to distribute immersive technology to hospitalized children at no cost. The Stanford Chariot Program has received philanthropic donations from Meta Inc., and Magic Leap, Inc. All other authors declare no competing interests or conflicts of interest.
Funding
This research was supported by the Stanford Chariot Program and SHC Creative and Healing Arts Program.
Ethical Approval
Our institution does not require ethical approval for reporting quality improvement projects.
Statement of Human and Animal Rights
This article does not contain any investigations with human subjects, rather, it is a quality improvement project.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because this was a quality improvement project.
Data Availability
Data is not available to protect protected health information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.