
Abstract
Patient communication with healthcare professionals regarding their health is essential for patient engagement in healthcare; however, some medical professionals do not facilitate this process. This study aimed to analyze the concept of patient–healthcare professional dialog from the patient perspective, using Walker and Avant's eight stage methodology. The findings show that patient–healthcare professional dialog can be defined as the process in which patients exchange and share opinions with healthcare professionals who stay close to them, fostering a trusting partnership, while participating in the decision-making process regarding their medical care. The identified antecedents for dialog were the need for communication, time and space for dialog, and being acquainted with each other. Dialog determined the emergence of a desire for recovery and feelings of reassurance. This concept analysis has proven useful to understand patients in their entirety as individuals. It introduces a new framework for communication training programs, promoting patients’ active involvement in their healthcare.
Plain Language Summary
Dialog between healthcare professionals and patients is crucial for patients' healing. It helps create a sense of security, trust, and reassurance for patients, that they have been heard and are in safe hands. It also encourages the patient to proactively participate in their own healing. Contrastingly, if the patient feels that the healthcare professional does not have time or the inclination to listen to their concerns or perspectives, their desire for healing can literature on the topic to consolidate the insights from patients. The study findings are useful for developing training programs for health professionals on respecting the dignity of patients and encouraging their participation in healing.
Key Points
If patients and healthcare professionals cannot engage in effective dialog, patients remain mere recipients of information from healthcare professionals. The author has defined patient–healthcare professional dialog from the patients’ perspective as the process in which patients can exchange and share opinions with healthcare professionals who stay close to them, fostering a trusting partnership and making joint decisions on patients’ medical care. The patient–healthcare professional dialog allows the latter to respect the former's opinions, and actively involves patients in their own medical care. To facilitate dialog between patients and healthcare professionals, it is essential that the latter respect the former's opinions and stay close to them.
Dialog between healthcare professionals and patients is crucial for patients’ healing. It helps create a sense of security, trust, and reassurance for patients, that they have been heard and are in safe hands. It also encourages the patient to proactively participate in their own healing. Contrastingly, if the patient feels that the healthcare professional does not have time or the inclination to listen to their concerns or perspectives, their desire for healing can be compromised. This lack of dialog may cause unnecessary health complications. This study examined the existing literature on the topic to consolidate the insights from patients. The study findings are useful for developing training programs for health professionals on respecting the dignity of patients and encouraging their participation in healing.
Introduction
The importance of effective patient–healthcare professional communication cannot be overstated. Patient communication with healthcare professionals regarding their health is essential for patient engagement in healthcare. 1
However, Gruffydd-Jones and Hansen 2 reported that many patients with asthma struggle to explain specific observations or problems to their doctors in a way that is accurately understood. Other researchers have found that physicians often disagreed with parents’ perceptions of their children's symptoms, leading to strained relationships between families and healthcare professionals.3,4 The lack of effective communication between healthcare professionals and patients has been shown to lead to poor patient participation in healthcare. 5
The Merriam-Webster Dictionary defines “communication” as “a process by which information is exchanged between individuals”, 6 (communication). Various studies have been conducted and frameworks developed on patient-healthcare professional communication. For example, the Hospital Consumer Assessment of Healthcare Providers & Systems (HCAHPS) Survey is a national, standardized survey of patients’ perspectives on hospital care that measures communication with doctors and nurses, hospital staff responsiveness, medication communication, the hospital setting, discharge information, posthospital care transition, and overall hospital ratings, 7 (Hospital CAHPS).
In addition, Islam and Muhamad 8 extended the HCAHPS survey to assess patient-centered communication, adding items measuring clinicians’ affective and instrumental communication, and provided a new metric for assessing doctor–patient communication.
The 9-item Shared Decision-Making Questionnaire, developed using a theory-driven approach, measures the extent of patient involvement in decision-making from both the patients’ and physicians’ perspectives, 9 (SDM-Q-9/SDM-Q-Doc).
These scales assess factors such as courteous attitude and language, adequate explanations, and active listening to symptoms by the provider.
Healthcare professionals and patients differ in their perspectives: Healthcare professionals tend to view disease as a malfunctioning biological process, while patients often perceive illness as a psychosocial experience. 10 There is also a difference in treating and being treated.
While “communication” refers simply to the exchange of information between individuals, the Merriam-Webster Dictionary defines “dialogue” as “an exchange of ideas and opinions” or “a discussion between representatives of parties to a conflict that is aimed at resolution,” 11 (dialog). Dialog involves the exchange of ideas and values in problem-solving between representatives. It requires mutual understanding of each other's role and the context to facilitate meaningful exchange. If healthcare professionals and patients engage in “dialogue,” which involves people with differing perspectives, they can better understand each other's ideas and opinions. Consequently, this may encourage patients to participate in their own healthcare. Therefore, clarifying the concept of dialog is essential, as it differs from the basic communication between a medical provider and a patient.
The concept of dialog is vague and ambiguous. Specifically in healthcare, healthcare professionals and patients may have different perspectives on the dialog between them. The whole scope of the patient–healthcare professional dialog must be identified from the patient's perspective to facilitate their proactive participation in healthcare and better understand how healthcare professionals can help patients better achieve this facilitation.
By moving beyond the traditional framework-based perspective of training, such as focusing on the provider's attitude and careful explanation and emphasizing the patient–provider relationship based on the concept of dialog, health professionals can provide multifaceted support to enhance patient participation in health care.
Thus, analyzing the patients’ perspective on the patient–healthcare professional dialog by synthesizing previous studies can help build theoretical and more effective support to facilitate their dialog. Therefore, this study aimed to analyze patients’ perspectives on the patient–healthcare professional dialog systematically, identifying its antecedent factors and consequences.
Methods
Concept analysis is the process of examining the basic elements of a concept, refining ambiguous concepts, and promoting understanding of the concept's attributes. 12 Walker and Avant 12 indicated eight steps to capture the essence of the concept analysis procedure: Select a concept; determine the aims or purpose of analysis; identify all uses of the concept; determine the defining attributes; identify a model case; identify borderline, related, and contrary cases; identify antecedents and consequences; and define empirical referents.
Following these eight steps, 12 a dictionary and literature review were conducted to identify the uses of the concept. Subsequently, comprehensive search strategies were conducted to seek all available studies. The author explored patient–healthcare professional dialog from the patients’ perspective through a search in the Cumulative Index of Nursing and Allied Health Literature (CINAHL), MEDLINE, conducted in March 2023. The search terms that were used are provided in the supplement file. The search was limited to articles written in English and published in academic journals. The inclusion criteria were as follows: (1) Study participants had a disease or underwent treatment; (2) the study contained qualitative data on participants’ perceptions of their dialog with healthcare professionals; (3) the study participants could communicate through speech. Articles were excluded if (1) they had no descriptions of patients’ perceptions of their dialog with healthcare professionals; (2) they were focused on only the healthcare professionals’ perspective; (3) it was difficult to distinguish between data on patients and healthcare professionals’ perspectives; (4) the participants were pregnant women, lying-in women, or “clients” (a term typically used in mental health settings).
A total of 460 records were identified through database searching (Figure 1). After eliminating duplicates and incorporating additional relevant publications from the articles’ reference lists, all articles were screened by title and abstract to assess initial eligibility. Subsequently, in-depth reviews of the entire text of all articles were conducted and excluded if found ineligible. Finally, 13 qualitative studies satisfied the inclusion criteria for the concept analysis. All 13 studies are listed in the concept analysis in Table 1.

Search strategy and study selection flow chart.
Confirmed Studies Satisfying the Inclusion Criteria for This Concept Analysis.
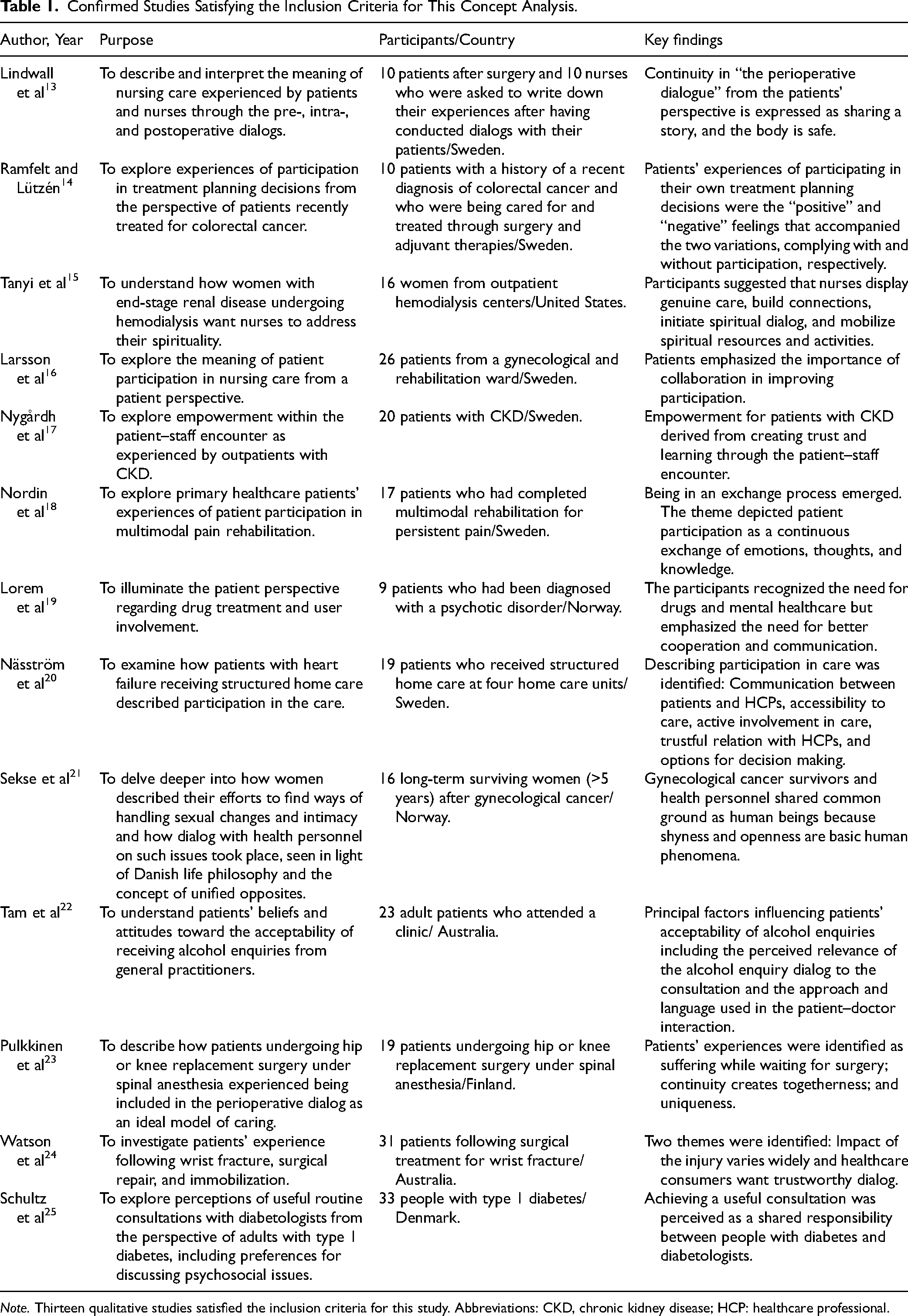
Note. Thirteen qualitative studies satisfied the inclusion criteria for this study. Abbreviations: CKD, chronic kidney disease; HCP: healthcare professional.
Later, the descriptions of the phenomena of the concept from all the studies were extracted. The extracted data containing similar content were clustered to derive their attributes. The derived attributes were named to indicate the occurrence of the particular phenomenon accurately. By comparing the derived attributes with other extracted data, the attributes were repeatedly revised and refined. An experienced researcher supervised the attribute process.
Results
Uses of Dialog
The word dialog comes from the Greek dialogos, dia meaning “through” and logos meaning “word,” or “speech” and by extension, “to speak,” 11 (dialog). According to Bohm, 26 a theoretical physicist, “this [dialogue] will make possible a flow of meaning in the whole group, out of which may emerge some new understanding.”
Dialog had a crucial role in the establishment of Western philosophy. According to the Dictionary of philosophy and thought, 27 dialog, as elaborated by philosophers such as Socrates and Plato, is a movement in which different logics collide in an open forum and attempt to reach a heightened awareness through confrontation. Furthermore, philosopher Martin Buber's concept of dialog refers to the communion and relationship that occur between I and Thou, as opposed to knowledge, which objectifies everything as it and attempts to grasp it objectively. Taken together, these interpretations perceive dialog as approaching the others’ personality and mutually exchanging words and ideas to create new perceptions.
Attributes
Defining the attributes of a concept is the essence of concept analysis, as they are the characteristics that name the occurrence of a specific phenomenon as differentiated from another. 12 The four attributes identified by this literature review were (1) staying close to the patient, (2) exchanging and sharing, (3) fostering trust as partners, and (4) making decisions.
Staying Close to the Patient
This attribute refers to patients being able to recognize those healthcare professionals who remain close to them. Patients experienced that the physicians and nurses were there to support them. 14 The close connection between patients and healthcare professionals was significant in the decision-making process. 14
Exchanging and Sharing
This attribute refers to patients being able to exchange and share opinions with healthcare professionals. Patients described their dialogs with nurses as sharing their stories with nurses. 13 The dialog process implies a dynamic give-and-take regarding questions or answers in conversations between healthcare professionals and patients; that is, both parties interact.16,18,25
Fostering Trust as Partners
This attribute is characterized by both patients and healthcare professionals as fostering a trusted partnership. Patients perceive the relationship with the healthcare professional as a partnership with their dialog increasing their confidence, trust, and satisfaction with the relationship.14,17,23,25
Making Decisions
This attribute refers to patients who can participate in making decisions about their treatments and care through open dialog with physicians and nurses. 14
Case Examples
Walker and Avant 12 expressed that “A model case is an example of use of the concept that demonstrates all the defining attributes of the concept.” A borderline case is an example that contains most, but not all defining attributes of the concept being examined. A contrary case is a clear example of what the concept is not. This study considered cases and research data from the literature to compile the case studies below.
Model Case
Mark, a three-year old, had a runny nose, cough, and fever of 38 °C. His mother was concerned about his health and took him to a physician. The physician listened to the mother's details regarding the child's health and performed a careful medical examination. The physician said to the mother, “This must be concerning for you. Mark is able to eat and is not cranky; therefore, I will prescribe an antipyretic.” She asked for an antibiotic; the physician inquired as to her reasoning and explained in detail why Mark did not require an antibiotic. She understood and agreed with the physician's explanation. She decided to take only the antipyretic and keep an eye on Mark.
This case was a typical example of all four attributes. The physician listened carefully to the mother's story, stayed close to her, and acknowledged her worry about the child's health. The mother could exchange and share opinions with the physician and participate in making the decision regarding treatment. She agreed with and trusted the physician's opinion.
Borderline Case
Mark had a runny nose, cough, and fever of 38 °C. His mother was concerned about his health and took the child to a physician. The physician listened to the details of the child's health, as reported by the mother, and carefully conducted a medical examination. The physician said: “This must be concerning for you. Mark can eat and is not cranky, therefore I will prescribe an antipyretic.” She asked the physician to prescribe an antibiotic. The physician only answered that Mark did not need to take an antibiotic. The mother wanted to know the reason, but the physician appeared too busy. Therefore, she felt she could not say anything and felt dissatisfied.
The physician listened carefully to the mother's story and stayed close to her worry about her child's health. However, the mother could not fully share her opinion about the antibiotic prescription with the physician; thus, she could not completely exchange opinions with the healthcare professional. She could not take part in the choice of treatment.
Contrary Case
Mark had a runny nose, cough, and fever of 38 °C. His mother was worried about his health and took him to a physician. The physician asked her to provide an abbreviated version of the child's health and conducted a medical examination. The physician stated, “I will prescribe antipyretics and see how they work.” She asked the physician for an antibiotic prescription, but the physician replied, “The treatment should be decided only by the physician.” She could not ask the physician any further questions.
In this case, the physician did not stay or offer sufficient explanations to the mother from beginning to end. Furthermore, she could not give her opinion in the choice of treatment. She did not trust the physician's examination.
Antecedents
Antecedents are those events or incidents that occur prior to the occurrence of a concept. 12 Two antecedents to dialog emerged from this literature review.
Need for Communication
This antecedent refers to the need for patients to communicate about their health problems, their desire for knowledge and information to understand more about their illness and what has happened to them. 19 Furthermore, patients need to communicate about their health issues or spiritual needs and hope that their healthcare professional will initiate the dialog.15,21,22,24
Space and Time for Dialog
This antecedent was characterized as healthcare professionals providing patients with time and space, and thus allowing patients to feel free to ask questions. Home visits provide increased time and space that improve communication between patients and healthcare professionals; that is, time (visit) and space (home) for dialog. 20
Well-Known to Each Other
This antecedent is explained as patients and healthcare professionals knew and trusted each other, which began the dialog. 23
Consequences
Consequences are those events or incidents that occur as a result of the occurrence of a concept. 12 The consequence of dialog extracted from the literature review is the emergence of a desire for recovery and feelings of reassurance. The first can be explained as a desire for health recovery which can emerge from participating in constructive dialog with the healthcare professional. 18 The second consequence is characterized by patients feeling a sense of relief and support from the dialog with healthcare providers. 20 Through dialog, patients feel safe, and trust the nurses with caring for their bodies. 13
Empirical Referents
This study could not locate instruments that measure all four attributes of patient–healthcare professional dialog from the patient's perspective. However, one instrument was identified that measures how patients participate in making decisions regarding treatment and care. Kaplan et al 28 developed an instrument that asks adult patients to rate how physicians involve them in making decisions about their care. This scale consists of the following three items: (1) Involving patients in treatment decisions, (2) giving patients a sense of control over medical care, and (3) asking patients to take some responsibility for care. Kaplan et al 28 reported three items with a Cronbach's alpha reliability coefficient of 0.74, indicating the validity of the scale.
Discussion
Concept Analysis of Patient–Healthcare Professional Dialog from Patients’ Perspectives
Based on the results of the analysis, the concept of patient–healthcare professional dialog from patients’ perspectives was defined as exchanging and sharing opinions with healthcare professionals who stay close to patients, fostering trust as a partner, and allowing patients to participate in making decisions about their treatment and care. When a healthcare professional conversed with a patient in a manner that respected the patient's choice without denying their preference for alternative medicine, the patient was satisfied with the exchange of ideas and chose complementary medicine instead. 29 The attitude of the healthcare professional in respecting the patient's wishes without denying them also implies being attentive to those wishes. When healthcare professional shares opinions and ideas with patients, they are able to make satisfactory decisions about their healthcare.
However, an analysis of recorded conversations between patients with atrial fibrillation and their physicians regarding anticoagulant decision-making showed that all seven elements of informed decision-making, as outlined by Braddock et al, 30 were included only twice (5%;. 31 The data for this analysis were obtained from the Verilogue Point-of-Practice database, which contains audio recordings of patient-physician encounters that have been transcribed. 32
Using this database to analyze recorded conversations regarding the attributes of dialog would likely also prove useful in promoting participation in patients’ decision-making.
The identified antecedents for dialog are the need for communication, time and space for dialog, and being well-known or trusting of each other. Dialog is facilitated when the healthcare professional provides an environment—implying space and time—in which the patient is comfortable talking, or when the two are familiar with each other. When the healthcare professional creates a comfortable environment for the patient to talk, the latter perceives that the healthcare professional is there for them. Thus, the concept analysis of this study revealed that the foundation of patient–healthcare professional dialog is the patient's realization that their healthcare professionals are there for them.
Practical Implications
Dialog determines the emergence of a desire for recovery and a feeling of reassurance. Patients’ discomfort and anxiety were significantly reduced when they perceived that they had discussed their treatment plan with their physicians. 33 Similarly, this study showed that when patients are able to exchange ideas about their treatment plans with their healthcare professionals, they are reassured and their desire for recovery is ignited.
The results of this study suggest that strategies can be implemented in practice to establish opportunities for dialog and improve mutual understanding between health care professionals and patients. Some of these strategies are described as follows.
Creating a Hospital Setting Conducive to Communication
Health care professionals should ensure that patients feel comfortable initiating conversations. Professionals should not appear overly busy and must demonstrate that they have time to listen. It is necessary to create a comfortable environment with appropriate placement of chairs and desks.
Fostering Rapport Through Initial Casual Conversation
Even when meeting a patient for the first time, health care professionals should avoid immediately discussing the patient's physical condition or treatment. Instead, they should begin with casual, everyday conversation to ease the patient's tension and understand their personality.
Providing Holistic Care
Healthcare professionals should be proactive in understanding the patient's disease as well as their overall context, including their daily lives, values, and thoughts. It is important to ensure conversations proceed at the patient's pace rather than the professional's.
Encouraging Two-way Interactions
Health care professionals should avoid one-sided statements, paying close attention to the patient's words to understand their underlying meaning. This approach empowers patients to take the initiative in the conversation.
Building Trust as a Health Care Professional
Healthcare professionals must earn patients’ trust by providing clear, appropriate explanations about their therapy and how the disease affects the patient's daily life.
These respectful attitudes will lead to the development of a partnership between patients and healthcare professionals, who can then work together on the best treatment.
To facilitate dialog between patients and healthcare professionals, it is essential that the latter respect the former's opinions and remain close to them. In other words, patients should feel acknowledged and respected by healthcare professionals as individuals, not as one of many patients.
The concepts identified in this study can strengthen relationships between healthcare professionals and patients by fostering a deeper understanding of each other's values and contexts. This understanding can enhance patient engagement in shared decision-making and improve satisfaction with medical care.
This concept analysis revealed how support should be provided to encourage dialog. Understanding patient–healthcare professional dialog from the patient's perspective can support patients in actual practice.
This concept of dialog can add a new dimension to the framework for communication training programs for patients and healthcare professionals and promote patients’ involvement in their healthcare.
Limitations
A limitation of this study is that only qualitative data on participants’ perceptions were considered. Future studies should quantitatively examine the relationships between the identified attributes, antecedents, and consequences, incorporating empirical validation to bolster the credibility of the findings.
Furthermore, research should explore healthcare professionals’ perspectives of dialog to provide a balanced view of the barriers to and facilitators of effective communication.
Conclusion
The author has defined patient–healthcare professional dialog from the patient's perspective as the process in which patients can exchange opinions with healthcare professionals and foster a partnership based on trust, for joint decision-making regarding their medical care. The concept analysis showed that through the patient–healthcare professional dialog, patients are respected as individuals and can actively address their own medical care. The patient's perspective on the concept of dialog between patients and healthcare professionals can help understand patients as individuals. This study has provided a unique and novel approach to analyzing the concept of patient-provider dialog from the patient's perspective. Further investigation into this concept from healthcare professionals’ perspectives is essential to develop more effective strategies for supporting patient participation in healthcare.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251324395 - Supplemental material for Patient-healthcare Professional Dialog from the Patient's Perspective: Concept Analysis Based on Literature Review
Supplemental material, sj-docx-1-jpx-10.1177_23743735251324395 for Patient-healthcare Professional Dialog from the Patient's Perspective: Concept Analysis Based on Literature Review by Akiko Yamada in Journal of Patient Experience
Footnotes
Acknowledgments
The author would like to thank Honyaku Center Inc. for editing and reviewing this manuscript for English language.
Authors Contributions
AY designed, collected data, analyzed, drafted the manuscript.
Data Availability Statement
The data generated by this study has been included in this paper.
Declaration of Conflicting Interests
The author declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not required as the study was a literature review.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (Grant Number: JP19K11071).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.