
Abstract
Loop diuretics are strongly recommended in patients with chronic congestive heart failure (HF) to alleviate signs and symptoms of fluid overload. Loop diuretics help relieve congestive symptoms and reduce mortality, but may have side effects. This survey study examined the impact of loop diuretic-induced overactive bladder (LD-OAB) symptoms on quality of life (QOL) in HF patients; and management of OAB by HF patients and physicians. We found that (1) HF patients noted less severity of symptoms but similar QOL with non-HF. (2) HF patients (58.8%) self-managed and underreported symptoms to physicians compared to non-HF (74.8%); accordingly 65% of physicians noticed and managed symptoms. (3) Patients used mechanical solutions (pads/diapers, Kegel exercises, and fluid reduction), and physicians adjusted diuretic doses or prescribed medications for OAB. Our study highlighted that HF patients' QOL associated with bladder symptoms was not better than the non-HF group despite milder symptoms. Many HF patients either did not report or coped with/self-managed their loop diuretic-induced bladder symptoms, pointing to a need for better awareness of patient experiences and patient-physician communication.
Keywords
Introduction
Heart failure (HF) is defined as the heart's inability to pump blood effectively to meet the body's demand. 1 HF can lead to congestion and/or hypoperfusion, causing symptoms such as fatigue, shortness of breath, and weight gain. Untreated HF can result in frequent hospitalizations and reduced quality of life (QOL).2,3 HF is one of the most prevalent conditions worldwide that increases morbidity and mortality among patients. 4 About 6.2 million American adults have HF, and this number is projected to increase to 8 million by 2030.4,5
In keeping with the American College of Cardiology/American Heart Association (ACC/AHA) guidelines, loop diuretics are strongly recommended in patients with chronic congestive HF to alleviate signs and symptoms of fluid overload. 1 Over 80% of HF patients are prescribed an oral loop diuretic, with furosemide being the most common choice.6,7 While loop diuretics can alleviate fluid-related congestion, they have side effects that include worsening of symptoms from overactive bladder (OAB).6,7 Previous studies suggest that the use of loop diuretics is associated with higher prevalence of urinary frequency (adjusted odds ratio (OR) = 3.09; 95% CI = 1.20-7.97), urgency (adjusted OR = 2.50; 95% CI = 1.00-6.27), and incontinence (adjusted OR = 1.88; 95% CI = 0.57-6.17). 7
Urinary frequency is considered abnormal when urination occurs more than eight times within a 24-hour period, and may occur regardless of amount of fluid consumed. 8 Urinary urgency is defined as the sudden need to pass urine that is difficult to defer. This urgency may result in a sudden desire to urinate that is difficult to control, leading to frequent trips to the restroom throughout the day and night (nocturia), disrupting sleep patterns. 8 Urinary frequency and urgency are quite often accompanied by involuntary leakage of urine, known as urgency urinary incontinence. 8 These symptoms collectively contribute to emotional distress, anxiety, and embarrassment, thereby necessitating medical intervention and lifestyle adjustments for effective management.9-11
These symptoms of OAB are associated with an impairment in QOL, with urinary urgency and urinary incontinence being the most bothersome. 9 They may affect the social, psychological, occupational, domestic, physical, and sexual aspects of life for those who suffer from it. 10 For instance, those with OAB may not want to spend time with friends or family members because they are afraid of being far from the restroom and having to make frequent visits to the restroom. The nature of these symptoms may also result in reluctance to report and/or discuss their conditions with family members, caregivers, or healthcare providers. 12 Thus, the management of OAB in HF patients and its impact on QOL has not been well studied.
Furthermore, less than half of these patients seek treatment for their urinary symptoms. 9 Reports from patients with OAB symptoms indicate that while they value physician communication, there is a lack of satisfaction regarding treatment options for OAB and a feeling that their symptoms are not taken seriously.9,12 Therefore, it is imperative to examine physician and patient perspectives regarding management of OAB symptoms among patients with HF who are on loop diuretics, and its subsequent impact on their QOL.
The objectives of this study were to examine (1) the impact of loop diuretic-induced bladder symptoms on QOL in HF patients; and (2) the management of OAB symptoms by HF patients and by physicians managing them.
Method
Study Design
This study used a cross-sectional survey design including patient and physician panels provided by M3 Group, Inc. (a health research company) and Qualtrics platform for electronic survey administration. This study protocol was approved by the Institutional Review Board at Western University of Health Sciences (ID: 2089126-2). Eligible participants provided informed consent upon reviewing the survey introduction.
Sampling
The patients were English-speaking, aged ≥55 years, and suffering from symptoms of OAB. HF group consisted of patients with HF who were using a loop diuretic. Non-HF group did not have HF and were not taking loop diuretics. The desired sample size for patients was 176 participants in each group, determined using an independent t-test, with a statistical power of 0.8, an alpha level of .05, and a small effect size (d = 0.3), as calculated using G*Power. 13 To account for attrition, we recruited at least 250 patients for each patient group.
A representative sample of physicians (primary care providers and cardiologists) who prescribed loop diuretics for treating patients with HF were recruited and completed the physician survey. Physician sample size was limited to 200 based on access and funding constraints.
Data Collection Tool
Several tools, including Overactive Bladder Questionnaire (OAB-Q) and Patient Perception of Bladder Condition (PPBC), are available to assess OAB symptoms and their impact on daily life, but they usually do not directly evaluate the symptoms themselves, lack comprehensiveness in assessing disease-specific QOL, and omit a symptom management section. 14 Additionally, to our knowledge, no existing tool is specifically designed to assess these symptoms in HF patients taking loop diuretics. Therefore, we developed more comprehensive and validated instruments to address these gaps and better suit our research questions.
All participant surveys underwent face and content validation involving four physicians for the physician survey and four laypeople for the patient survey. Following validation, two questions from the physician survey and three questions from the patient survey were revised to enhance clarity. Survey responses were collected from patient and physician panels by M3 Group, Inc. using Qualtrics links.
The patient survey included a total of 24 questions related to OAB history, symptoms, management methods, bladder symptom-related QOL, and patient characteristics (health literacy and demographics: gender, race/ethnicity, education level, health insurance, annual household income, health conditions, and number of prescription medications). The HF group completed three additional questions related to loop diuretic use. The physician survey comprised six questions, covering their characteristics, OAB symptoms that patients reported, and management of HF patients with loop diuretic-induced OAB symptoms.
Outcome Measures
The primary outcomes included the bladder symptom-related QOL score (BS-QOL), bladder symptom (BS) severity score, and BS management score. The 10 BS-QOL items were scored on a 4-point Likert scale (never = 4, sometimes = 3, most of the time = 4, and always = 1). The total BS-QOL score (range 10-40) was calculated as the sum of these items, with a higher score reflecting better bladder symptom-related QOL. The BS severity score (3-12) was determined by the sum of three symptom severity questions on a similar scale where never = 1, sometimes = 2, most of the time = 3, and always = 4. A higher BS severity score indicated more severe symptoms. The BS management score (0-8) represented the number of strategies used by the patient to manage their bladder symptoms.
Statistical Analysis
Data were collected through the Qualtrics platform and analyzed using IBM SPSS v29.0. 15 All analyses were conducted at a 95% significance level. Descriptive analysis was performed to summarize survey responses. Independent t-tests, chi-square tests, and one-way ANOVA were used to compare characteristics between groups. A correlation analysis was conducted to assess the association between BS-QOL scores and other outcomes. Physician and patient responses were also compared to assess congruency. Reliability of the scale was assessed utilizing Cronbach's alpha as a measure of internal consistency. Factor analysis with Varimax rotation was conducted to evaluate construct validity of the surveys.
Results
Participant Characteristics
A total of 500 patients and 202 physicians completed the surveys from December 2023 to January 2024. Patients' baseline characteristics are shown in Table 1. Key characteristics were similar between the two groups, except for gender (lower % females in HF group), annual household income (lower income in HF group), number of health conditions, and prescription medications (higher number in HF group). These results align with published prevalence data of HF.16-19
Comparison of Baseline Characteristics and Outcome Measures of Patient Groups.

Abbreviations: BS, bladder symptom; GED, general educational development; PhD, Doctor of Philosophy; SD, standard deviation; QOL, quality of life.
Among the physicians, there were slightly more cardiologists (57.4%) than primary care providers (42.6%). Approximately 60% of these physicians had more than 10 years of practice experience. Group practice was the most common practice setting.
Instrument Validation
Cronbach's coefficient alpha of 0.88 revealed high internal consistency and hence strong reliability for the 11-item QOL questions (HF group: 0.89; non-HF group: 0.87). Factor analysis with varimax rotation revealed moderate to strong item-item correlations with the predicted variables indicated in Table 2. Most items loaded as expected, except for the reverse-coded item 9, resulting in the three domains as expected: bladder symptom severity (.611-.832), QOL items (.643-.806), and overall QOL (.653).
Construct Validation of Survey Using Factor Analysis with Varimax Rotation.

The colour shaded cells indicate those with the same colour, which have been loaded in the same domain (as mentioned in the instrument validation section).
Summary of Outcome Measures
Table 1 provides a summary of average BS severity score, BS management score, and BS-QOL between the two patient groups. Although the HF group exhibited a significantly lower BS severity (7.10 vs 7.59; P < .05) and BS management (1.48 vs 2.02; P < .001) than the non-HF group, there was no difference in the bladder symptom-associated QOL between the two groups (28.86 vs 28.69; P = .384). Additionally, these three scores did not differ among individuals using different types of loop diuretics (Furosemide (75% of HF group), Torsemide (17%), and Bumetanide (8%)).
A pooled analysis revealed significant correlations between BS severity score, BS management score, and BS-QOL. Notably, BS severity (r = −.547, P < .05) and management scores (r = −.468, P < .05) exhibited negative correlations with BS-QOL, while a positive correlation was observed between BS severity and BS management scores (r = .284, P < .05). These correlations were consistently significant within each patient group, following the same pattern.
Symptom Reporting Between HF and Non-HF Patient Group
In the HF group, 90.0% had increased urination, 85.6% experienced urinary urgency, and 67.6% reported incontinence, while in the non-HF group, these figures were 93.2%, 92.5%, and 85.6%, respectively. Overall, a significantly higher percentage of HF patients did not report OAB symptoms to their physicians compared to non-HF patients (41.2% vs 25.2%, P < .001). When HF patients reported their loop diuretic-induced bladder symptoms to their physicians, they were more likely to receive suggestions, of which lifestyle modification was more common, followed by prescribed medications, referral to specialists. A similar pattern was seen in non-HF patients, although medications were prescribed more commonly than lifestyle modification.
Comparison of HF Patient-Reported and Physician-Noticed Symptoms
Figure 1 compares HF patient and physician responses on whether patients were reporting loop diuretic-induced OAB symptoms to physicians. Among the three bladder symptoms (increase in frequency, urgency, and incontinence), an increase in urinary frequency was the symptom most commonly mentioned by both groups.

Comparison of HF patient-reported symptoms and physician-noticed symptoms.
About half of the HF patients reported experiencing urinary urgency at some point, while only one-third of physicians observed the same. Patient urinary incontinence was reported by approximately one-third of patients (32.4%) and physicians (36.1%). These results align with previous literature reports. 7
Symptom Management by Patient Groups and Physicians
As shown in Figure 2, in keeping with the pattern of HF patients underreporting their loop diuretic-induced bladder symptoms to their physicians, they also did nothing to manage these symptoms compared to the non-HF group (14.4% vs 4.9%, P < .001). Among HF patients who actively managed their symptoms, the most common methods include wearing pads/diapers (25.5%), avoiding liquids (20.9%), and performing Kegel exercises (12.8%). Non-HF patients employed similar methods such as wearing pads/diapers (24.1%), avoiding liquids (21.8%), and taking OAB medications (14.9%).
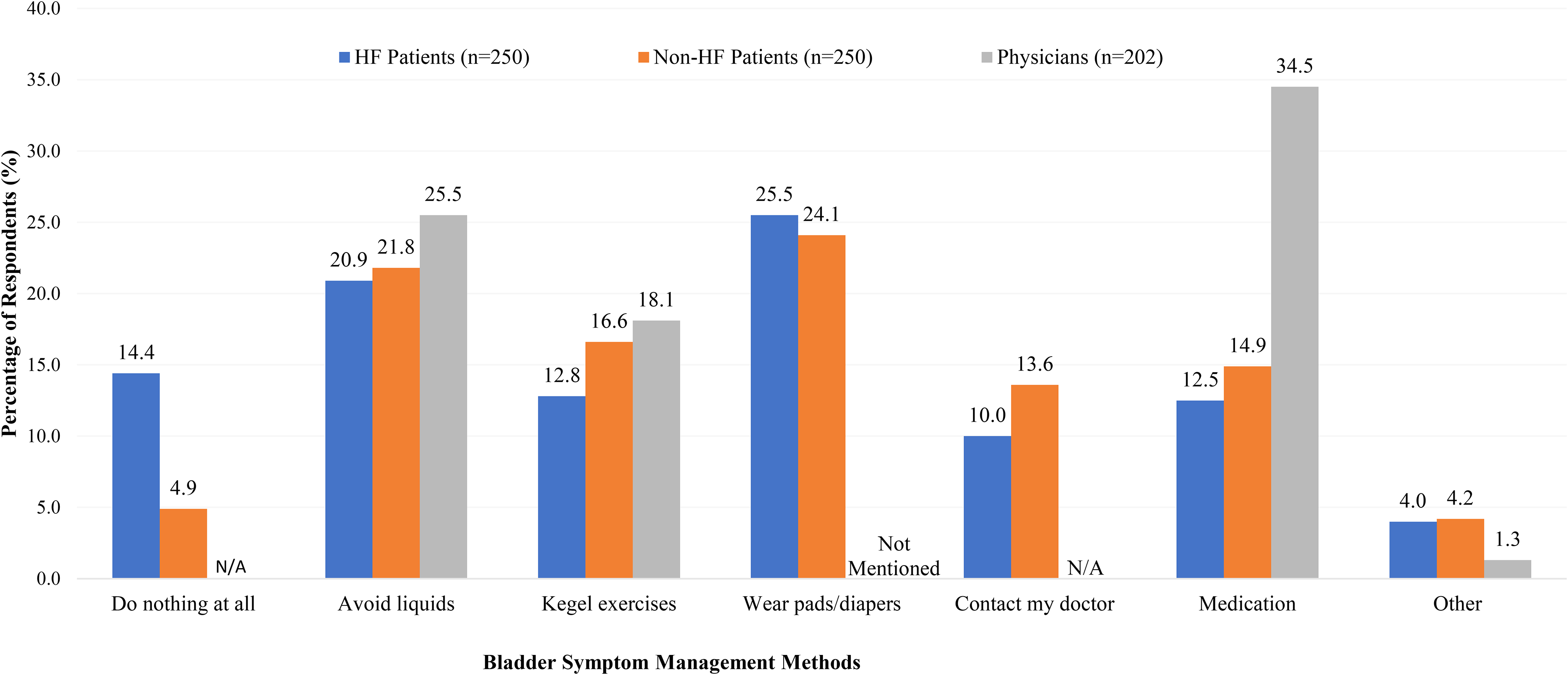
Comparison of bladder symptom management between patient groups and physicians.
Physicians did not mention wearing pads/diapers as a technique to manage these bladder symptoms. Instead, they recommended medication-related methods (over the counter [OTC] and prescription medications) and adjusting time and dosages of the loop diuretic administration.
Discussion
This study assessing OAB symptom incidence, management, and impact on QOL used a survey tool that also underwent psychometric testing and demonstrated strong reliability and validity. The study results revealed differences between HF and non-HF patients and between patient and physician perspectives.
The patient groups differed in gender, income, number of health conditions, and prescription medications. Although prevalence data mention that more males in the age group of 60 to 70 years have HF, there is also data indicating that OAB impacts more females.16,19 Our HF sample consisted of more females with the combination of HF and OAB. Income levels in the HF group were lower than the non-HF group which aligns with previous research indicating an association between lower income levels and increased cardiovascular risk.17,18
Our study revealed that despite experiencing milder bladder symptoms than the non-HF group, HF patients reported similar QOL associated with bladder symptoms. This finding points to a need for better management of OAB symptoms overall; regardless of the HF condition, these bladder symptoms were noticeable in both patient groups, which had a significant impact on patients' QOL.
Another key finding was the asynchrony of symptom experience and the reporting to physicians; and the subsequent or correlated differences in how patients self-managed their symptoms and what physicians recommended to patients for managing bladder symptoms. This is exemplified by more HF patients reporting “doing nothing” to manage their bladder symptoms and also not reporting symptoms to their physicians, compared to the non-HF group. This tendency of HF patients to be less actively engaged with reporting and managing these bladder symptoms could be explained by several factors: (a) the lower severity of bladder symptoms experienced by HF patients; (b) HF patients may have developed acceptance/coping skills for the unavoidable side effects of loop diuretics; (c) HF patients may prioritize managing their heart condition over addressing bladder symptoms; and (d) more than half of the HF patients in our sample had more (3-5) concurrent health conditions hence they may be more focused on dealing with those, diverting attention away from bladder symptom management. The converse could be true for non-HF patients in our sample, who had OAB but less than three health conditions.
Increase in urination frequency was the most prevalent loop diuretic-induced bladder symptoms reported by both the HF patients and by physicians. However, physicians reported lower frequencies of urinary urgency and incontinence than the HF patients, indicating a need for promoting clear communication and mutual understanding between patients and physicians. In short, patients need to feel comfortable reporting symptoms and/or physicians should be encouraging patients to report all symptoms.
Limiting fluid intake was a common non-pharmaceutical technique used by patients and suggested by physicians to control symptoms; however, disparities were noted in bladder symptom management. Patients who actively managed their symptoms commonly used wearing pads/diapers, a method that was not mentioned by physicians in our sample. Instead, physicians were more inclined to recommend medication-related methods, such as prescribing OAB medications, adjusting loop diuretic dosages, and counseling on the timing of loop diuretic administration. This disparity may be because wearing pads/diapers primarily addresses symptom management rather than targeting the underlying causes. While it can be a practical solution for managing these symptoms, physicians may prioritize interventions that address the root cause or provide more comprehensive symptom relief.
Although our study did not examine the QOL of HF patients in general, previous research has shown that HF can severely impact patients' QOL by reducing their independence and daily activities.2,3 Poor QOL is also associated with high hospitalization and mortality rates. 3 It is important to recognize the significant impact of HF on QOL, as well as the potential dual impact of HF and loop diuretic-induced bladder symptoms. These bladder symptoms can be managed more effectively compared to heart conditions. However, unlike non-HF patients, many HF patients in our study hesitated to report their loop diuretic-induced bladder symptoms to physicians, often resorting to self-management or no management. Patients might not feel comfortable discussing these symptoms or may accept them as an unavoidable side effect of taking loop diuretics. Our results point to the need for physician awareness of the impact of these bladder symptoms on QOL and subsequently, the need to proactively ask patients if they experience these symptoms and attempt resolution, in the event that patients do not bring them up.
HF and non-HF patients employed similar strategies for symptom relief, such as fluid restriction and using pads/diapers, but physicians typically used different approaches with HF patients. They were more inclined to address root cause by adjusting loop diuretic administration time and/or dosage or prescribing OAB medications. Additionally, cardiologists might not consider managing bladder symptoms given their specialized focus on cardiovascular conditions and the need to manage patients' edema. Enhancing patient-physician communication regarding symptom reporting and management is imperative to understand patient needs and identify the most effective interventions for symptom alleviation and improvement of QOL.
Limitations
A limitation of our study, as is true of survey studies, could be the reliance on self-reported data that may have introduced bias or inaccuracies in bladder symptom reporting. Future studies could improve by incorporating objective measures alongside self-reported data. Research also needs to examine factors contributing to disparities in perception and developing interventions to enhance patient-physician communication and symptom management.
Conclusion
HF patients' QOL associated with bladder symptoms was not better than the non-HF group despite milder symptoms. Many HF patients either did not report or coped with/self-managed their loop diuretic-induced bladder symptoms, indicating a need for improved communication with physicians, to help subsequent physician-aided management. Discrepancies in perception and symptom management between patients and physicians highlight the necessity for better patient-physician communication and understanding of patient preferences.
Footnotes
Acknowledgments
We would like to express our gratitude to Eunhee Kim, PharmD; Sun Jin (Olivia) Lee, PharmD; and Tina Nguyen, PharmD for their contributions to this study.
Authors’ Contributions
XP contributed to study design, data acquisition, analysis, result interpretation, and drafting the manuscript. CW contributed to the conception and reviewed the manuscript. BP contributed to the conception and reviewed the manuscript. SS contributed to the conception and reviewed the manuscript. AL contributed to conception, study design, result interpretation, and manuscript preparation.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SS is affiliated with the funding organization, but there was no conflict of interest as the study focused on patient-reported outcomes related to a class of medication and did not examine any specific product produced by the company.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Sarfez Pharmaceuticals Inc. The funders contributed to the concept and reviewed the manuscript but had no role in the study design, data collection and analysis, or decision to publish.
Ethical Approval
This study protocol was approved by the Institutional Review Board at Western University of Health Sciences (ID: 2089126-2).
Informed Consent
Eligible participants provided informed consent upon reviewing the survey introduction.