
Abstract
Patient experience is a crucial measure of healthcare quality with the potential to increase value for several health stakeholders. However, various barriers often hinder its impact on quality improvement. Therefore, valid and reliable instruments developed through structured and collaborative processes are needed to establish methodological and organizational practices and ensure consensus and credibility among all stakeholders. This study presents the development and validation of the Patient Experience Assessment of in-Center Hemodialysis (PEACHD) survey. An expert panel, cognitive interviews, and a pilot test were conducted, involving both people receiving hemodialysis care and professionals from four Italian hospitals. The questionnaire evaluates key aspects of the in-center hemodialysis experience, including the provision of medical information, involvement in treatment decision-making, and communication with professionals. The PEACHD survey demonstrated strong content and face validity, acceptable construct validity, and good internal consistency reliability. Pilot data highlighted that the professional delivering care (i.e. nephrologist or dialysis nurse) significantly influenced patient experience and emphasized the need for a holistic and person-centered approach. The PEACHD survey enables effective patient experience evaluation, enhancing value for both service users and professionals.
Keywords
Key Points
Patient experience is crucial for healthcare quality, but organizational, methodological, and cultural barriers hinder its implementation.
Developing valid and reliable instruments collaboratively is essential for building stakeholder consensus and credibility.
The PEACHD survey was developed and validated with input from both individuals receiving hemodialysis and health professionals from 4 hospitals.
An expert panel, 21 cognitive interviews, and a pilot test with 366 participants using exploratory and confirmatory statistical analyses were conducted.
Psychometric testing included assessments of content, face, and construct validity, internal consistency reliability, and floor and ceiling effects.
The PEACHD survey is a valid and reliable tool, enhancing value for both service users and health professionals.
Introduction
The complexity of health systems and organizations necessitates the use of multidimensional performance measurement systems to assess the various types of value they produce. 1 Among these, the primary value to consider is that generated for their main stakeholders: health service users. Focusing on this value is crucial as it directly impacts the effectiveness, efficiency, and equity of care provided. 2 By prioritizing value for people receiving care, their families, and caregivers, a positive feedback loop is created, leading to improved outcomes and overall health system performance, ultimately enhancing value for all stakeholders, especially health professionals. 3 In this view, incorporating the service users’ perspective to assess the value delivered to them should be a fundamental pillar of health performance measurement systems.4–6 Patient experience has been described as one of the most effective frameworks to elicit these perspectives. 7 Patient experience encompasses individuals’ perceptions of the range of interactions they have with health services. These interactions cover crucial aspects like the provision of medical information, communication with health professionals, waiting times, and the quality of health facilities. Patient experience offers a unique assessment of these elements directly from the users’ viewpoint, providing insights unattainable from other sources. 8 This information can drive quality improvement interventions, steering health performance measurement systems toward a more holistic and person-centered approach. 4 Additionally, emerging methodologies support its integration with several socio-demographic and psychological traits to develop tailored experience profiles and segment populations, ultimately enabling predictive and personalized models of care for diverse service users.9,10 The importance of this measure is further evidenced by its positive association with traditional quality indicators such as clinical effectiveness and patient safety,11,12 making the assessment of patient experience essential for healthcare quality evaluation.4,5
Despite these claims, the systematic implementation of patient experience measures remains limited.13,14 Researchers have identified numerous methodological, organizational, and cultural barriers that hinder the impact of patient experience on driving quality improvement efforts. These include inadequate data collection methods, insufficient organizational resources dedicated to acting upon patient experience data, and skepticism among health professionals regarding the validity of these measures.15–19 To overcome these issues, it is essential to develop reliable and valid instruments through structured methodologies and collaborative efforts that actively involve both professionals and service users. 20 Such an approach allows for the effective and systematic evaluation of what people receiving care truly value, as well as generating consensus among all stakeholders involved.14,16 This collaborative process not only enhances the accuracy and relevance of the data collected but also builds trust and buy-in from health professionals, facilitating the use of patient experience to drive improvements in healthcare delivery.
In-center hemodialysis presents an ideal context for studying the empirical application of such an approach to provide effective patient experience assessment. Hemodialysis, while essential for prolonging the lives of individuals with end-stage renal disease, imposes a substantial burden, severely affecting physical, mental, and social quality of life. 21 People undergoing in-center hemodialysis have to visit health facilities at least 3 times per week for several hours and often for many years unless they receive a kidney transplant. This intensive treatment involves extensive interactions with care providers, which have a significant influence on the outcomes and thus the value delivered to these individuals. In this sense, patient experience can provide relevant information to understand “what matters most” to people undergoing hemodialysis, beyond appropriate medical treatments.22,23
However, apart from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) in the United States, 22 there is little evidence of structured patient experience assessments for in-center hemodialysis in other countries, including Italy. Most research on patient-reported data in this context has focused on health outcomes and quality of life, rather than patient experience. 24 Consequently, few valid and reliable instruments have been developed to assess the patient experience of in-center hemodialysis.
Given these premises, this study presents the structured and collaborative preliminary development and validation of an instrument for the systematic Patient Experience Assessment of in-Center Hemodialysis (the PEACHD survey) in the Italian context, aiming to benefit the value yielded to all the actors involved.
Methods
Setting
This study involved 4 public hospitals: 3 in Lombardy, Italy, and 1 in Ticino, the Italian-speaking canton of Switzerland. The dialysis units were staffed primarily by nurses and nephrologists. Dialysis sessions were organized into 2 or 3 shifts per day, with each person typically attending 3 times per week. The number of individuals receiving dialysis ranged from approximately 5 to 15 per shift. The study protocol was approved by the Ethics Committees of the 4 hospitals, and all involved participants explicitly agreed to join the study.
Preliminary Development and Validation of the PEACHD Survey
The development and validation of the PEACHD survey followed a structured process with 3 main steps.25,26 Initially, a draft questionnaire was created based on the validated In-Center Hemodialysis (ICH) CAHPS survey, 27 which was translated into Italian through a forward and backward translation process by 2 independent translators. During this phase, a first cultural and contextual review of the translated items was conducted by a researcher and a nephrologist involved in the project.
In the second step, initial validity evidence was gathered, focusing on content validity and face validity. Content validity, which checks whether the survey adequately covers all relevant areas of what it is intended to measure, was assessed by a panel of 5 nephrologists and 1 dialysis nurse. The panel rated the relevance of each item on a 4-point Likert scale (1 = not relevant to 4 = very relevant). 25 Items rated as 1 or 2 by any expert were revised. Face validity, which evaluates whether the survey items appear clear and understandable to respondents, was evaluated through a cognitive debriefing with 21 people undergoing hemodialysis. These individuals participated in “one-to-one” interviews to assess the clarity and understandability of each survey item. A “think-aloud” technique was used to gather feedback on the meaning of questions and response options, 26 and items reported as unclear by at least 20% of participants were revised.25,26 Qualitative feedback was also used to adjust the wording of some questions.
In the final step, statistical analyses were conducted to further evaluate the psychometric properties of the PEACHD survey. For this purpose, a pilot test was conducted across the dialysis units of the 4 involved hospitals. To provide every individual undergoing hemodialysis the chance to participate, health professionals extended invitations throughout a 1-week period. The survey was anonymous and could be completed either on paper (in 3 hospitals) or online via the Qualtrics® platform (in one hospital, using tablets provided by the dialysis ward). Participants had the option to complete the survey on-site during their dialysis session or take the paper survey home and return it at their next session. To support accessibility, respondents were also allowed to complete the survey with the assistance of a family member or caregiver.
To ensure robust statistical analysis, self-reported demographic, and health status characteristics of participants were compared across the 4 hospitals using chi-square tests, which analyze differences in categorical variables (eg, gender, education). For ordinal variables (eg, age groups), Kruskal-Wallis tests with Sidak post-hoc analysis were used to identify specific group differences.
Subsequently, the total pilot sample was randomly divided into 2 subgroups. The first subgroup underwent an exploratory factor analysis (EFA). The second subgroup was used for confirmatory factor analysis (CFA). EFA and CFA were employed to evaluate the survey's construct validity, which assesses how well the survey captures the theoretical framework it is based on. Specifically, EFA is used to investigate the construct structure of the questionnaire, identifying significant multi-item scales (ie, factors). These factors reflect the underlying theoretical structure of the questionnaire, thus providing validation to the assumptions behind its development. The EFA was configured specifically to analyze ordinal data (in this case patient experience items)28,29: polychoric correlation, minimum rank factor analysis, parallel analysis for factor number determination, and Promin rotation, with factor loadings of 0.6 or higher considered significant. CFA is used to verify the results of the EFA, confirming that identified factors are valid. CFA employed Bayesian estimation, suitable for ordinal data, 30 and assessed fit indices including the chi-square test (χ2), comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Additionally, internal consistency reliability of each factor, which measures how well the items in a factor work together to assess the same concept, was assessed using the ordinal alpha coefficient. Finally, to ensure the survey could effectively distinguished between respondents, floor and ceiling effects were also assessed, which refer to the proportion of respondents selecting the lowest or highest possible scores, respectively.
Although not the primary aim of the study, the extracted factors and satisfaction items in the PEACHD survey were used to provide an overall view of the experiences of care reported by participants through descriptive analysis. Differences among the 4 hospitals were also compared using the Kruskal-Wallis test with Sidak post-hoc analysis. Statistical analyses were performed using Factor software (version 11), IBM® SPSS® Amos™ (version 28), and STATA (version 17) with a significance level set at 5%.
In this study, the term “preliminary” is used to describe the development and validation of the PEACHD survey because, in the initial phase of this process, the ICH CAHPS questionnaire was altered without assessing the impact of these modifications. Changes to a standardized survey—even language translation—can introduce issues with validity, which were not addressed in this study. Future research is recommended to examine these validity concerns and fully assess the effects of the survey adaptations.
Results
Survey Development and Pre-Validation
All items from the original ICH CAHPS survey were translated into Italian. Some terms and verb tenses were adjusted by the 2 independent translators to better fit Italian syntax and vocabulary. The initial cultural review led to the removal of 4 items deemed unsuitable for the Italian context (Additional file 1).
Most items were rated as “relevant” or “very relevant” by the expert panel. However, 6 questions were deemed irrelevant by most panelists and were thus excluded from the questionnaire (Additional file 1). Based on expert feedback, changes were made, including rephrasing items about “dialysis center staff” to focus specifically on “dialysis nurses,” who, along with nephrologists, are the primary health professionals in Italian dialysis centers. Additionally, 3 items were duplicated to separately address interactions with nephrologists and dialysis nurses (Additional file 1).
Individuals undergoing hemodialysis involved in cognitive testing indicated that the items were clear and understandable and showed high interest in the questionnaire topics. Minor modifications were made based on their feedback, including replacing “nephrologists” with “doctors” to avoid confusion. Some participants noted potential difficulties in completing the entire survey during a single hemodialysis session due to both the survey length and side effects experienced during treatment (eg, fatigue, muscle cramps, dizziness). Consequently, the pilot test allowed participants to complete the survey over a longer period, enabling them to take it home and return it during their next dialysis session.
The PEACHD Survey
The final version of the PEACHD survey is detailed in Additional files 2 (English version) and 3 (Italian version). The questionnaire includes 52 items across 4 sections: (1) “Nephrologists,” (2) “Dialysis nurses,” (3) “Treatment,” and (4) “About you.” The first 2 sections feature most items duplicated to separately analyze interactions with nephrologists and dialysis nurses. These sections cover various aspects of patient experience, such as availability, consideration, support, medical information, and communication. The third section explores the provision of information and involvement in decision-making about dialysis modality and treatment options. The final section asks respondents about their health, including diagnosed conditions, symptoms, and overall physical and mental well-being. Items are presented with dichotomous (yes or no) or 4-point Likert scale (from “never” to “always”) response options. The survey also investigates respondents’ satisfaction with 2 scores (one for each of the first 2 survey sections) ranging from 1 (worst satisfaction) to 10 (best satisfaction) and a final item measuring their overall satisfaction. Five initial questions collect demographic information from participants.
Pilot Test Sample
The pilot study sample included 366 individuals undergoing hemodialysis (163, 82, 74, and 47 participants from each center, respectively). While some participants completed the survey during their dialysis session, others chose to complete it at home and bring it back. This approach, combined with limited staff availability, did not allow to systematically record precise completion times. However, dialysis staff observed that older and frailer patients faced some difficulties due to the survey's length, consistent with feedback from the cognitive testing phase.
Of all, 64% of the sample were male, 70% were 65 years or older, and 66% had been on dialysis for at least 2 years. About 48% reported their physical health as “poor” or “bad,” and 24% reported their mental health as “poor” or “bad.” Those with poorer physical health tended to report more diagnosed conditions and/or symptoms. Demographic and health-related variables are summarized in Table 1.
Sample's Characteristics.

The comparison of self-reported demographic and health-related variables across the 4 hospitals revealed no significant differences, indicating that the pilot sample was homogeneous and representative across the participating centers.
Statistical Psychometric Testing
The EFA involved 26 items from the questionnaire and the first subgroup of the pilot test sample (n = 183). The EFA identified 3 significant factors explaining approximately 61% of the variance among the items. Factor One grouped items related to nephrologists, Factor Two grouped items related to dialysis nurses, and Factor Three included items on information provision, decision-making about dialysis, and self-care activities at home. The factor loadings are shown in Supplemental Table 1. Item lists for each factor are presented in Table 2.
Survey Items Belonging to Each Factor.

Abbreviation: Q, question.
The Confirmatory Factor Analysis (CFA) assessed the 3-factor structure with the second subgroup of the pilot test sample (n = 183). CFA factor loadings were slightly lower than those from the EFA (Figure 1), and the chi-square test indicated that an exact-fitting model should be rejected (χ²(206) = 345.750, P < .001). However, other goodness-of-fit indices were acceptable (CFI = .925, RMSEA = .061, SRMR = .065), suggesting reasonable model-data fit.
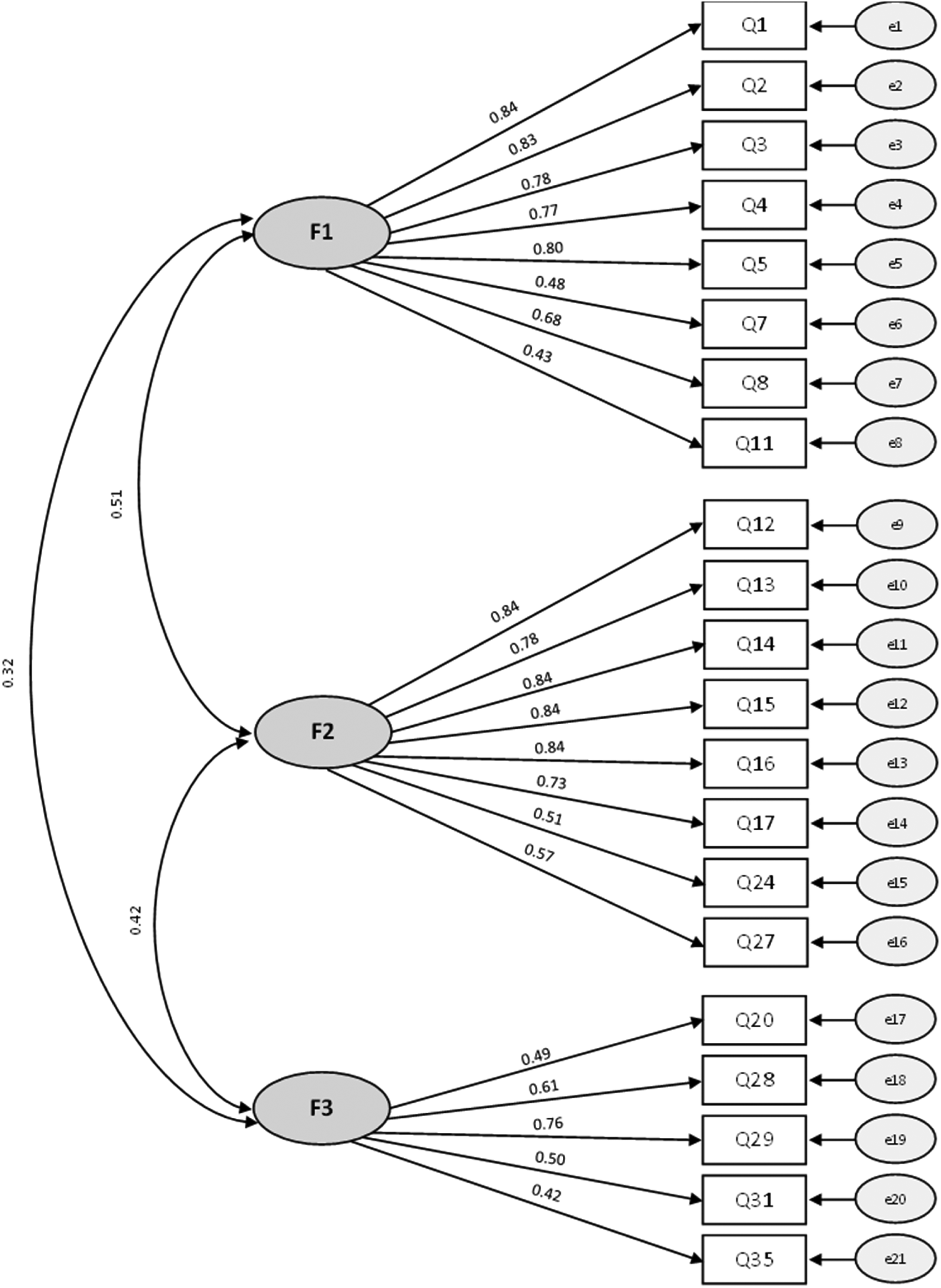
Confirmatory factor analysis: standardized estimates.
Factors One and Two demonstrated high internal consistency, with ordinal alpha values of .89 and .91, respectively. Factor Three had a lower but acceptable internal consistency (ordinal alpha = .69). Floor effects were minimal, with a maximum of approximately 4% for Factor Three. Ceiling effects were 15%, 38%, and 34% for Factors One, Two, and Three, respectively, and ranged from 69% to 87% for satisfaction items.
Reported Experiences of Care
Overall, participants reported positive experiences with nephrologists. However, about one-third experienced issues with communication, availability, and consideration from nephrologists (Figure 2). Regarding treatment options, 13% felt they did not receive enough information, and 19% felt insufficiently involved in decision-making.

Patient experience of hemodialysis: nephrologists and dialysis nurses.
Experiences with dialysis nurses were generally very positive (Figure 2). Nonetheless, nurses sometimes failed to provide information on self-care activities at home, with 24% and 25% of respondents reporting no information on diet and health problems, respectively.
High satisfaction levels were reported for both nephrologists and dialysis nurses, with median scores of 8 and 9, respectively, on a 10-point scale. Additionally, 78% of respondents reported never being dissatisfied with the overall care received.
Comparison of experiences and satisfaction scores across the 4 hospitals highlighted significant differences only for Factor One (χ²(3) = 33.787, P < .001) and satisfaction with nephrologists (χ²(3) = 20.644, P < .001). Post-hoc analysis indicated that these differences were both attributable to the same hospital, where more positive experiences and higher satisfaction with nephrologists were reported compared to the other hospitals.
Discussion
Patient experience is increasingly recognized as a key measure of healthcare quality because it provides essential insights directly from service users, identifying what they truly value.4,5 The structured and collaborative development and validation of instruments for patient experience assessment are crucial to generate consensus and legitimize this measure,14,16 helping to overcome barriers to its adoption for quality improvement in healthcare delivery. This approach offers several benefits: (1) it establishes a normative expectation regarding the importance of this measure, overcoming skepticism about its validity; (2) it identifies the aspects and interactions that need evaluation, minimizing “blind spots”; (3) it considers and weighs the needs and preferences of all stakeholders; (4) it defines the correct methodology for data collection, ensuring systematic and reliable data gathering; (5) it allocates workloads and responsibilities among health staff dedicated to this activity; and (6) it facilitates benchmarking, accountability, and the sharing of best practices.22,23 This approach aims to produce commitment and generate value for all stakeholders involved to ensure effective evaluation of patient experience, thereby promoting the maximization of its potential in enhancing healthcare delivery.
Following this approach, this study showcased the structured and collaborative preliminary development and validation of an instrument to for the systematic Patient Experience Assessment of in-Center Hemodialysis (the PEACHD survey) in the Italian context. By actively involving professionals and service users to provide a valid and reliable instrument, the aim was to enhance the value for all stakeholders involved. Questionnaire items were initially developed based on a validated instrument used within the CAHPS program in the United States. The research then moved to the field, involving the dialysis centers of 4 public hospitals with an expert panel, cognitive interviews, and a pilot test of the questionnaire. The developed questionnaire demonstrated good content and face validity, though there were some concerns related to its length. Despite the model not perfectly fitting the data, it was considered acceptable as the first specification of the newly developed questionnaire's construct structure. The PEACHD survey showed good internal consistency reliability, as indicated by satisfactory ordinal alpha analysis. Finally, although not the primary aim of this study, comparing experiences and satisfaction among pilot test participants across the 4 participating hospitals demonstrated the practical utility of the PEACHD survey for quality improvement, also through cross-site learning. Further research is recommended to enhance the survey's psychometric properties and address issues related to its length.
The developed questionnaire comprehensively evaluates various aspects that significantly shape the perceptions of people receiving in-center hemodialysis, as evidenced by the 3 underlying dimensions identified through factor analysis in this study. Specifically, the analysis distinctively separated survey items pertaining to nephrologists (Factor One) and dialysis nurses (Factor Two). Therefore, the category of health professionals emerged as a pivotal determinant of the patient experience in in-center hemodialysis. Specifically, in the pilot study, care provided by dialysis nurses received significantly higher evaluations compared to that by nephrologists. However, while individuals have continuous interactions with nurses during dialysis sessions, interactions with nephrologists are more intermittent and contingent upon visit frequency and duration. Moreover, staffing levels vary considerably between these roles, with a higher nurse-to-patient ratio observed. Consequently, it is plausible that individuals are likely to report more positive experiences with nurses, particularly in terms of availability and attentiveness. However, past evidence has highlighted that while improved patient experiences were observed in dialysis centers with higher nurse-to-patient ratios,31,32 more patient-nephrologist visits were not associated with better experiences of care.33,34 Therefore, further research should be carried out to investigate potential drivers for improving the experience of people undergoing hemodialysis related to nephrologists.
Factor Three focused on information about self-care activities and engagement in choosing dialysis modality. A significant number of participants in the pilot study reported not receiving adequate information about self-care activities at home and felt insufficiently involved in the decision-making process. Patient education and engagement are key principles of person-centered care, leading to positive outcomes such as increased satisfaction, reduced anxiety, and improved treatment compliance.35,36 Therefore, dialysis staff should ensure that individuals are well-informed and actively participate in shared decision-making. This approach is crucial in providing holistic and value-based care for people whose concerns and needs persist beyond each dialysis session.
Finally, the PEACHD survey also comprises 3 items to measure satisfaction with the received care in dialysis centers. In the pilot study, high scores were reported for all 3 items. While this represented a positive result for the dialysis centers involved, it also meant that elevated ceiling effects were observed for these items. This suggests that the included satisfaction scores may be limited in their ability to distinguish among respondents. Specifically, high satisfaction may be reported even in the face of less positive experiences of care, as repeatedly shown in the literature.9,37–39 Consistent with these findings, the ceiling effects of the 3 experience factors fell within normal ranges, proving a certain degree of discrepancy between the reported experience and satisfaction with care for a significant portion of the respondents. This discrepancy likely arises because patient experience focuses on objective events and interactions, whereas satisfaction is a more subjective, volatile, and often optimistic measure, heavily influenced by treatment outcomes. 9 In this sense, satisfaction often reflects patients’ gratitude for the care received, which may present a somewhat limited and favorable view. Additionally, in this study, this effect may stem from the limited availability of alternative care options, particularly for a burdensome treatment like hemodialysis, where patients may be less willing to travel long distances to receive care. These considerations should stimulate reflection on the future use of the satisfaction scores included in the developed questionnaire. In this sense, they should not be used as synthetic indicators but rather as a complement to patient experience assessments, which provide a more objective description of the quality of care as perceived by health service users.
The present study had several limitations. First, as mentioned, this was a preliminary development and validation of the PEACHD survey, representing an initial project with a limited scope. Future research should expand upon this work to conduct a comprehensive assessment of the survey's validity and reliability, especially regarding the effects of adapting the standardized ICH CAHPS instrument. Second, although the survey was anonymous, the mode of survey administration in the pilot study—on-site completion during hemodialysis sessions—could have introduced potential mode bias, particularly in how participants perceived anonymity and confidentiality. Similarly, to increase accessibility, participants were allowed to complete the questionnaire with the assistance of a family member or caregiver, which may have influenced some responses. These potential sources of bias were not addressed during data analysis and should be considered when interpreting the findings. Third, due to the requirements for anonymity and the project's duration, it was not feasible to administer the questionnaire to the same group of respondents twice, preventing the evaluation of test–retest reliability. Future research should focus on assessing test–retest reliability to further validate the instrument. Finally, no demographic information was collected for those who chose not to respond to the survey, making it impossible to estimate nonresponse bias.
Conclusions
This study underscores the crucial role of patient experience assessment in guiding interventions aimed at improving care quality. Through the structured and collaborative preliminary development and validation of the PEACHD survey, our goal was to establish consensus and credibility for this measure, enabling its effective implementation in assessing patient experience across in-center hemodialysis care settings. As a result, the PEACHD survey has emerged as a practical tool that is methodologically sound and relevant to both healthcare professionals and service users, ultimately enhancing the value provided to all stakeholders. Further steps are necessary to establish this instrument as a consistent tool for ongoing monitoring and quality improvement. These steps include developing the technological, organizational, and human resources required to support the systematic collection, management, and application of patient experience data. In essence, this study serves as a critical first step in a broader journey. The structured and collaborative approach adopted here has laid a strong foundation and a clear path forward, with the PEACHD survey expected to yield valuable insights into areas for improvement as well as shed light on aspects of care perceived positively by individuals receiving hemodialysis.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735251314653 - Supplemental material for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey
Supplemental material, sj-docx-1-jpx-10.1177_23743735251314653 for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey by Nicola Spezia, Cristina Masella, Carla Colturi, Gianvincenzo Melfa, Ines Ullo, Silvio Pianca, Maria Laura Costantino and Giustina Casagrande in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735251314653 - Supplemental material for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey
Supplemental material, sj-docx-2-jpx-10.1177_23743735251314653 for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey by Nicola Spezia, Cristina Masella, Carla Colturi, Gianvincenzo Melfa, Ines Ullo, Silvio Pianca, Maria Laura Costantino and Giustina Casagrande in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735251314653 - Supplemental material for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey
Supplemental material, sj-docx-3-jpx-10.1177_23743735251314653 for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey by Nicola Spezia, Cristina Masella, Carla Colturi, Gianvincenzo Melfa, Ines Ullo, Silvio Pianca, Maria Laura Costantino and Giustina Casagrande in Journal of Patient Experience
Supplemental Material
sj-docx-4-jpx-10.1177_23743735251314653 - Supplemental material for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey
Supplemental material, sj-docx-4-jpx-10.1177_23743735251314653 for Unlocking Patient and Professional Value Through Patient Experience: Preliminary Development and Validation of the Patient Experience Assessment of In-Center Hemodialysis (PEACHD) Survey by Nicola Spezia, Cristina Masella, Carla Colturi, Gianvincenzo Melfa, Ines Ullo, Silvio Pianca, Maria Laura Costantino and Giustina Casagrande in Journal of Patient Experience
Footnotes
Acknowledgments
We would like to thank all the study participants who made this research possible.
Author Contributions
NS developed the study concept and design. NS organized and facilitated activities related to the expert panel, cognitive interviews, and pilot study, with operational support from CC, GM, IU, and SP. NS conducted the statistical analysis of the pilot study data and drafted both the initial and revised versions of the manuscript. All authors contributed to data interpretation. CM was the principal supervisor of this work and provided critical revisions. All authors read and approved the final manuscript.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been carried out within the activities of the InterACTIVE-HD 2.0 project that has received funding from the European Union’s Interreg V-A Italy-Switzerland Co-operation Programme 2014-2020 (ID: 1441882). The authors received no financial support for the authorship and publication of this article.
Ethical Approval
This study was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. Ethical approval was obtained from the Ethics Committees of the 4 hospitals involved. For ASST Lariana and ASST Sette Laghi hospitals, the study protocol was approved by the Ethics Committee of Insubria (session of 28 September 2021). For ASST della Valtellina e dell'Alto Lario hospital, approval was granted by the Ethics Committee of Brianza (session of 18 November 2021). For Ente Ospedaliero Cantonale, the Ethics Committee of the Canton of Ticino approved the study protocol (session of 24 November 2021).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the approved protocols of the Ethics Committee of Insubria (session of 28 September 2021), the Ethics Committee of Brianza (session of 18 November 2021), and the Ethics Committee of the Canton of Ticino (session of 24 November 2021).
Informed Consent
The individuals engaged in the expert panel and cognitive interviews provided verbal informed consent to participate. Participants in the survey pilot test provided written informed consent to join the study and for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.