
Abstract
The study explores how Primary Health Care Team managers in Catalonia assess the gold standard criteria for excellence in Primary Health Care and whether there are differences in evaluations between the best and worst-rated centers by patients in a patient experience survey included in the Catalan Satisfaction Survey Plan (PLAENSA). The researchers used mixed methods to analyze 12 interviews done to Primary Care Team (PCT) managers. Interviews were transcribed and analyzed, yielding three themes and 12 subthemes. A Likert-type questionnaire was also used to compare results. Scores were observed between 4.8 and 3.5 regarding a constant relationship with the patient (longitudinality), and patient’s experience, respectively. All managers highlight accessibility, nursing management, and administrative support as essential to patient experience. No significant differences exist in PCT’s scores or gold standard element application. Disposing of good accessibility, crucial in Primary Health Care management, an administrative team, and efficiently prepared and motivated professionals, are key elements to a patient's experience in Primary Health Care. Contrary to other studies, interviewees described better accessibility in rural centers, which is likely why they are better valued by patients.
Keywords
Introduction
The Primary Health Care system is relevant because it ensures universal care. Quality at this first level of care is related to accessibility, longitudinality, comprehensive care, and coordination between professionals. 1
The Catalan healthcare model was established in 1990 and integrates all public and private nonprofit healthcare resources into a network for public use. 2 The Institut Català de la Salut (ICS) is publicly managed. Integrated Health Organizations (OSI) assign economic resources depending on the number of people they take care of, considering their demographic characteristics and health necessities. In Associative-Based Entities, professionals administrate resources autonomously.
World Health Organization defines quality care as effective, efficient, integrated, equitable, safe, and patient-centered service delivery. 3 Berwick et al 4 include the patient as part of quality care and highlight their experience as one of the objectives of the Triple AIM. 5 In 2014, it evolved into the Quadruple AIM 6 to include the well-being of the professional team as a fourth vertex of healthcare quality.
Patient-Reported Experience Measures are validated and internationally recognized instruments to measure patient experience. 7 In Catalonia, the Satisfaction Survey Plan (PLAENSA) offers patients experience results in the Observatory of the Health System of Catalonia since 2012. 8 The latest PLAENSA report, covering 2018 to 2022. It offers data on different healthcare devices such as Primary Health Care (PC). 9
Varela et al 10 defined 22 Gold Standard PC criteria for excellence. Our work's objective is to explore how the Primary Care Team (PCT) managers assess the Gold Standard criteria and the variables’ weight and whether there are differences in the management between the best and worst-rated centers in the PLAENSA surveys.
Materials and Methodology
The PLAENSA surveys from 2015 to 2022 in Primary Health Care and the Gold Standard PC indicators described by Varela et al were used as references.
A mixed methods technique (qualitative and quantitative) 11 was used to mitigate the study limitations, 12 understand the information from a multidimensional prism, and maintain reliability and validity.13,14
Qualitative design with phenomenological approach and nonprobabilistic 15 intentional sampling to identify 21 centers worst and best scoring in the PLAENSA surveys during the 2015 to 2022 editions. Twelve managers of mixed genders, from rural and urban centers, with medical and nursing backgrounds were interviewed. All with experience in management and direction of the three management models in Catalonia. They were identified with alphanumeric codes. Eight professionals who did not respond to the invitation were excluded (Table 1).
Profile of Interviewed Managers: Personal Characteristics (i.e., Gender, Profession, Management Experience), Center (Managing Entity, Rural/Urban), and PLAENSA Rating (Best/Worst).

Abbreviations: ICS, Institut Català de la Salut; OSI, Integrated Health Organizations; EBA, Associative-Based Entities.
The interview guide (Supplemental annex 1) was developed based on published literature, 16 the Gold Standard elements, and the authors’ experience. The 12 interviews, which averaged 35 min, were transcribed verbatim. Braun and Clarke's 17 six-step inductive approach was used for thematic analysis. Thirty-eight codes were identified and synthesized into three themes and 12 subthemes. Data were collected and analyzed until information saturation. 18
The quantitative design used a Likert-type questionnaire of 31 questions adapted from Gold Standard indicators (Supplemental annex 2). Participants were asked to rate the degree of agreement with each Gold Standard indicator on a scale of 1 to 5. The coincidence of the results obtained from the two approaches facilitated comparing the qualitative and quantitative results and allowed the consistency between two kinds of data to be verified. 19 The qualitative and quantitative fieldwork was carried out from June 2023 to February 2024.
Ethical Considerations
Participants were informed about the study's purpose and the possibility of withdrawing at any time, while data confidentiality was assured. Informed consent was obtained and recorded verbally. The interviews were recorded, and the data were stored according to the General Data Protection Regulation (GDPR). Any identifying data inadvertently captured was deleted.
Quantitative Results
Table 2 summarizes the managers’ scores for each question (graphs added in Supplemental annex 3). The best scores with a high degree of coincidence were professional engagement, PCT integration, longitudinality, availability of professionals who act as consultors (clinical reference), teamwork, right care, agenda availability, and adequate treatment areas.
Managers’ Scores on the Gold Standard Dimensions. a

Comparison between the scores of the primary care managers of the centers with the best and worst PLAENSA values.
Other areas that showed good scores but with lesser agreement included positive leadership promotion, burnout prevention, multidisciplinary teams with social services, talent management, updated information on hospital admissions, and community health promotion.
There is a third group of good evaluations but with profound disagreements, such as the relationship with community pharmacies, satisfaction as an indicator of quality, administrative support, clinical sessions between professionals of different levels of care, medical support services, and pediatric care.
Finally, there are criteria with the worst evaluation and most significant disagreement, such as the managers’ importance to the PLAENSA results, pediatric and mental health care by the nursing team, preparation of the medical team in shared decision-making (SDM), use of telemedicine, patient participation in organizational matters, cocreation dynamics with patients, and video consultations.
Upon categorizing the questions, scores of decreasing importance were observed for the work environment, longitudinality, multidisciplinary care, local collaborative strategies (territory alliances), accessibility and administrative team, interconnected activities that add value to patient care (value chains), nursing team, complaints and suggestions, patient satisfaction, biological care, psychosocial, and patient experience, ranging between values of 4.8 and 3.5.
Table 2 compares the scores of the Primary Health Care managers of the centers with the best and worst PLAENSA values. Some considerations stood out when average scores were reviewed on the different subtopics and questions between these two groups of managers. The most critical differences in average scores favor the centers with the worst PLAENSA values. They highlight the better assessment of prescription of activities and community services to improve the physical, mental, and social well-being of patients (social prescription), SDM, budget allocation to realize medical tests, alliances with community pharmacies, and complementary health services such as mental health, sexual health, podiatry, and dentistry.
When analyzing the subthemes, emphasis on the orientation toward biopsychosocial assistance shows a higher accessibility rating in the centers than the others, with no substantial differences in other subtopics. The highest score of the best-rated centers in PLAENSA was given to improving pediatric care (community, nursing, and hospital) concerning longitudinality and the “gaps” (free time to be scheduled) in the agendas.
The worst and best centers rated by PLAENSA scored the same regarding the importance of the patient experience as an element of health quality or nursing demand management.
Qualitative Results
Out of the 12 managers, 3 nurses and 4 doctors with an average of 20 years of management experience got the best scores. Six manage rural centers and 1 manages a rural center. Five are managed by ICS and 2 by OSI and EVA. Alternatively, 1 nurse and 4 doctors, with an average of 5 years of management experience, manage the 5 worst scored centers, 3 managed by ICS and 2 managed by OSI (Table 1).
Below is a comprehensive summary of the results based on 3 themes and 12 subthemes (Table 3).
Verbatim of the 12 Interviewed Directive Grouped by Theme, Subtheme and Characteristics of the Primary Care Team Best and Worst Valued.
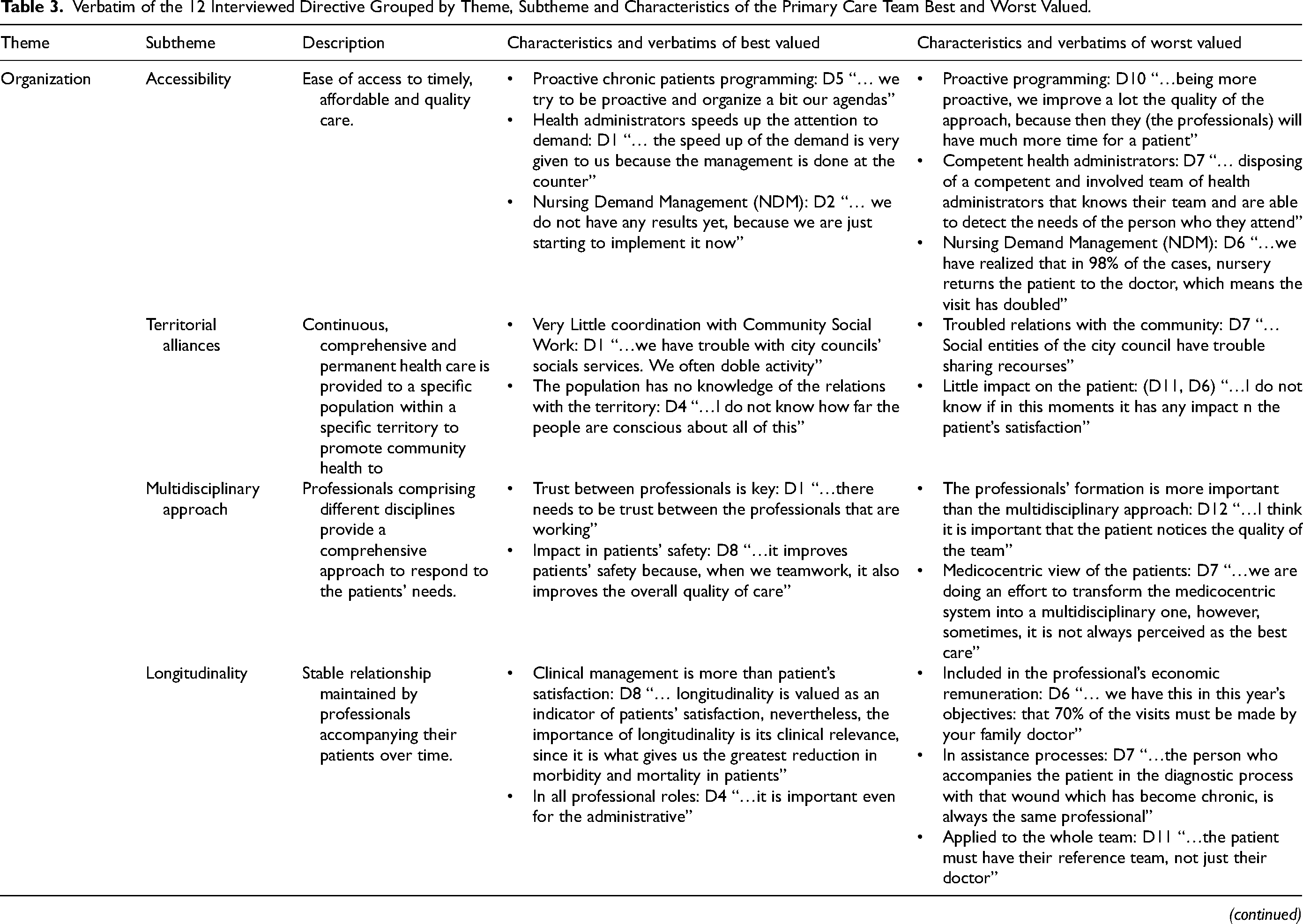
Theme 1: Organization. Five subtopics were highlighted:
Accessibility: Quick access to tests improves the user’s experience, while a lack of maternal and childcare services worsens it. Responsible use of health services by patients is valued. The limited availability of professionals and budget allocation was singled out as a problem in rural areas. Teleconsulting visits can improve accessibility in these areas. Managing care requests remains a problem for some professionals (“…our problem is always with specific professionals who have much tendency to reprogram patients” (D4)).
Territory alliances: They are essential but complicated and minimally improve the patient experience. City councils sometimes allocate resources poorly. To avoid this situation, more collaboration between social services and Primary Health Care is suggested (“…It is difficult for the social entities of the City Council to share resources” (D7)). Social prescribing pilot tests are successful but hampered by rural areas’ lack of facilities.
Multidisciplinary care: It is considered essential for quality care, generates trust, and solves problems efficiently. However, the patient’s expectation that care will always be medical can limit the acceptance of other professionals (“…An effort is being made to move from a medico-centric model to a multidisciplinary model, although sometimes, it is not in the expectations of patients.” (D7)).
Longitudinality: Some centers have incorporated it into economic compensation based on objectives achievement (Management by Objectives), which requires adequate provision of professionals to cover sick leaves and vacations. In some cases, it occurs in a specific clinical process. “…we understand it by processes, that is, the same person who accompanies the patient in that diagnostic process” (D7).
Non-face-to-face visits: Doctors can ask for a specialist’s colleague’s opinion and do consults through digital platforms (e-consultations), but not video consultations, which are recommended for some patients, although not for the elderly. In rural areas, video consultations are not necessary, due to good accessibility and lack of demand. They support telephone visits but warn about their excessive use, which could affect the quality of care. “…the convenience of telephone visits has the danger of excessive use” (D9).
Theme 2: Professionals. Four subtopics were considered:
Value chains: Managers are unfamiliar with this tool, which is perceived for high management. They usually have a referring doctor for the most common diseases and specific treatments, such as wounds, but they do not do activities jointly to add value to the patient. “…Maybe at the management level or the SAP level as centers they may have” (D8).
Nursing team: Some centers are developing nursing demand management, valued positively but seen as unresolved and duplicating visits. The nursing team is seen as having little capacity but is essential for proactive visits and as case managers. “…in 98% of cases, the nurse returns the patient to the doctor” (D6).
Health administrative team: Valued for its agenda management and efficient care. In some cases, it is considered part of the healthcare team. “…they respond to administrative requests that can be resolved at the counter” (D1).
Work environment: The work environment influences staff satisfaction and the quality of patient care. In rural settings, it can affect professional retention and team cohesion. “…We always have a full staff of doctors, which impacts user care” (D8).
Theme 3: Patient-centered care. Three subtopics were detected:
Patient experience: Meeting patient needs and responding to their demands improves their experience. “…patients feel satisfied as long as you can respond to the demand they ask of you” (D3).
Complaints and suggestions: Managers give them relative importance and sometimes they relate them to the inappropriate use of services; however, they see them as a tool for improvement. “…we collected many problems from patients’ opinions and improved many of the organizational things” (D10).
Biopsychosocial care: Knowing the patient and their environment is essential for quality care. Young patients require a different approach than older patients. “…in the end, they end up telling you what you say” (D11).
Discussion
In our study, managers from the worst-scored centers value patient feedback as an asset to implement improvements. However, they highlight that patient expectations sometimes don’t align with quality care, and they point out that patients need more skills to participate in organizational decisions or to partake in improvement actions.
Consequently, in line with other published studies, 20 managers have a somewhat contradictory opinion of patients: They consider them competent to evaluate the quality of care but biased by unmet expectations that have little or nothing to do with care quality. 21 This weakens the potential for changes to improve in response to patient feedback. 22
The results of our study coincide with others wherein it is concluded that well-organized multidisciplinary teams improve the experience of patients with increasingly complex needs. 23 At the same time, they can improve accessibility by delegating certain medical team activities to other team members. 24 However, patients’ medicocentric vision and their desire to be treated exclusively by these professionals represent a handicap in its implementation, which is agreed on by all interviewees. This finding complements the barriers described in the literature for multidisciplinary care. 25
Patient demand management by the nursing team was initiated in 2009 by the ICS, 26 considering that part of the activity carried out by doctors could be delegated to the nurse. As in other studies, ours identified barriers in some of the worst-scored centers to have effective and efficient patient demand management by the nursing team, such as the lack of empowerment, knowledge, and skills, as well as the need for more protocolization of interventions. 27 Like other studies, telephonic evaluation of patient seriousness is done by nurses and directs the demand to the most appropriate professional. 28
Managers consider that social prescribing reduces the burden of pharmacological interventions. 29 Thus, yoga, mindfulness, art, and swimming classes may be the most appropriate benefits for some patients. However, some benefits may be very limited in rural areas where these alternatives do not exist. 30 Longitudinality promotes a stable and maintained relationship through time with the patient and has an important role in their experience.
Promoting it can be a challenge, since it is subject to the available human resources, especially during vacation periods or due to the rotation of professionals in the work center. To respond to this weak point, the Primary and Community Care Action Plan 2022-2023 31 proposes increasing the number of professionals to improve longitudinality.
The environment and work climate of professionals are essential to good patient care. 32 Despite the efforts of the managers to maintain a healthy work environment, the different developed actions have had little impact. Regarding this gold standard element, a difference in the worst-rated center managers’ narratives is shown, who perceive negative dynamics of some patients toward professionals.
Although e-consultations can improve the patients’ experience, some worst-score urban centers have limited e-consultation because they see patients as hyperdemanding. Those who had the best scores note that not all technologies are suitable for all patients. Due to the digital unfamiliarity, video consultations may not be suitable for older people.
Effective coordination between municipal and healthcare resources is complicated regarding integrated care. This difficulty causes activities to disperse and a lack of communication between both groups. Creating the Social and Health Care Agency (AGAISS) 33 can be an ideal resource for developing more integrated and personalized care.
An essential element highly valued by all interviewed managers is the health administrative team, which allows efficient agenda management and administrative tasks, relieving healthcare professionals of this work.
Managers focus more on the technical quality of the service and leave the quality of the service perceived by the patient in the background. On the other hand, some professionals believe that the association between service quality and patient experience needs to be sufficiently clear.
Limitations: The size of the sample is a possible limitation to generalization. An attempt has been made to minimize this limitation, as convenient sampling was conducted with a variety of participants. Another limitation is possible bias toward self-reported data by managers, as participants may have provided distorted responses to present a more favorable image of themselves. This bias has been reduced through data source triangulation: interviews and surveys.
Catalonia’s geographical limitation may have limited the applicability of these findings in other regions. In future studies, incrementing sample size and including direct commentary from patients will help provide a more balanced and generalized vision.
Conclusion
The present study explores PCT managers’ perceptions regarding the gold standard elements in Primary Health Care in Catalonia. Accessibility, nursing management, and administrative support are highlighted as essential aspects of the patient experience.
There are not any significant differences between best and worst-scored PCTs and the application of gold standard elements. In contrast to other studies, 34 our interviewees described better accessibility in rural PCTs. Likely, this is why rural centers with better temporal accessibility data are better valued by patients.
To respond patients’ demands, professionals must be trained, motivated, and decisive in providing care; otherwise, they can generate an unfavorable patient experience and increase costs.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241282702 - Supplemental material for How do Patients and Managers Value Gold Standard Elements in Primary Health Care
Supplemental material, sj-docx-1-jpx-10.1177_23743735241282702 for How do Patients and Managers Value Gold Standard Elements in Primary Health Care by G Gálvez, ML Jimenez, R Manzanera, A Ávalos, M De Castro, I Moral and A Iruela in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735241282702 - Supplemental material for How do Patients and Managers Value Gold Standard Elements in Primary Health Care
Supplemental material, sj-docx-2-jpx-10.1177_23743735241282702 for How do Patients and Managers Value Gold Standard Elements in Primary Health Care by G Gálvez, ML Jimenez, R Manzanera, A Ávalos, M De Castro, I Moral and A Iruela in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735241282702 - Supplemental material for How do Patients and Managers Value Gold Standard Elements in Primary Health Care
Supplemental material, sj-docx-3-jpx-10.1177_23743735241282702 for How do Patients and Managers Value Gold Standard Elements in Primary Health Care by G Gálvez, ML Jimenez, R Manzanera, A Ávalos, M De Castro, I Moral and A Iruela in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.