
Abstract
The aim was to explore patients’ early experiences of symptoms after hemithyroidectomy and how these symptoms influenced their daily lives. An inductive explorative qualitative research design was performed. Sixteen patients from two hospitals were interviewed between two-three weeks after the surgery. All the patients experienced compression symptoms before the surgery. The study was analyzed with conventional manifest content analysis. The inductive analysis yielded two main categories and one subcategory. The two main categories were: Early postoperative symptoms that caused disadvantage in daily life and Early postoperative symptoms and coping strategies. The subcategory was: Early postoperative experiences of concerns about the future.
Keywords
Introduction
Thyroid nodules are common and may increase in size. Patients may experience compression symptoms because of compression from the thyroid nodule on the anatomical structures of the neck.1–3 Apart from thyroid hormone measurement, preoperative investigations generally include ultrasound and cytology with fine-needle aspiration where the cell formations are evaluated and classified according to cytology scoring systems (THY, Bethesda).4,5
Thyroid nodules may also overproduce thyroid hormones resulting in toxic adenomas. 6 If toxic adenomas are suspected, a thyroid scintigraphy is recommended that reveals functional and anatomical changes of the thyroid gland. 7 Whether surgery is necessary or not is determined by the symptoms, the cytology classification and the imaging results. Patients with a thyroid nodule suspicious for malignancy are recommended hemithyroidectomy. 5 Patients in whom thyroid malignancy is not suspected but who experience compression symptoms from the neck from a predominantly unilateral thyroid enlargement are usually recommended hemithyroidectomy. According to Scandinavian Quality Register of Thyroid, Parathyroid and Adrenal Glands (SQRTPA) hemithyroidectomies are mainly performed due to two indications, either diagnostically for suspicious nodule(s) (46%) or therapeutically to relieve compression symptoms (43%). 8
All the patients included in this study underwent hemithyroidectomy surgery to address compression symptoms related to a unilateral enlarged thyroid. Since these are mostly benign conditions, surgery to relieve the symptoms should not be accompanied with postoperative side-effects and symptoms.9,10
Theoretical Perspectives
Patient's symptoms experience is a manifestation of a wide and complex pattern. Experiences occurred across a variety of situations in the patient's life. The Holistic Theory of Unpleasant Symptoms (HTOUS) describes the complexity of patient's symptom experience, and broadly describes the consequences of symptoms and the holistic perspectives. 11 The theory reflects well our inductive research question based on patient experiences.
To our knowledge inductive research with patients’ experiences in focus after hemithyroidectomy for compression symptoms has been sparsely studied. Most existing qualitative research with focus on thyroid surgery is focused on patients with thyroid cancer12–14 or exploring postoperative side-effects. 15 The patients’ symptoms are of importance for person centered care. Understanding the human experience related to symptoms can provide a holistic understanding of patients essential to guide and enhance clinical surgical practice.
Patients perceived feeling of tailored supportive care may promote their postoperative health by positively affect the recovery process. The aim of the study is to explore patients’ early experiences of symptoms after hemithyroidectomy and how these symptoms influenced their daily lives. The research questions: what symptoms do the patients have after thyroid surgery? and how these symptoms affecting the patients’ health and daily life?
Methods
Design
An inductive explorative qualitative research design guided by Consolidated Criteria for Reporting Qualitative Research (COREQ). 16 COREQ has guided the study to ensure the qualitative scientific quality.
Inclusion and Exclusion Criteria
The inclusion criteria: patient of >18 years old, experiencing compression symptoms and cytology scoring of Bethesda I-IV, planned hemithyroidectomy due to the patient's local discomfort symptoms. Exclusion criteria were patients who have previously undergone neck surgery, patients with a toxic adenoma, and inability to speak the Swedish language.
Data Collection
With a purposeful sampling procedure, the interviews were performed between February and July 2022 from patients who were operated in two hospitals in the southeast of Sweden. A purposeful sampling has been chosen to obtain a diversity of informants regarding age, marital status and employment. All operations were performed by endocrine surgeons, and a PhD-student (male surgeon) performed the interviews (not involved in the patients’ care). The interviews were conducted between two-three weeks after the operation before the patients’ sick leave was ended. Interviews lasted on average 42 min (range 11-86 min), and were audio recorded and transcribed verbatim. The patients choose the time and place where the interviews were conducted. The reason why they chose a time/place for the interview was that they would feel safe and comfortable to talk about their situation. Open-ended questions were performed in accordance with a pilot-tested interview guide. No changes were made after the interview guide was tested. The questions were developed to answer the aim to investigate the patients’ early experiences of symptoms after hemithyroidectomy and the influence their lives. The guide included interview questions; “What symptoms do you have after your thyroid surgery” and “Can you describe how these symptoms are affecting your health and daily life?” Clarifying, probing, looping and follow-up questions were used during the interviews.17,18 The interviews were conducted by telephone, face-to-face interviews, or via digital meeting (zoom/teams) between the interviewer and the participants and field notes were made during the interviews. Data saturation was reached after fourteen interviews. This is in agreement with existing literature. 19
Data Analysis
The transcribed data was analyzed with conventional manifest content analysis.20,21 The first author (EB) coded the data and determined the first categories and subcategories. The data were read, and the first author highlighted the exact words from the transcribed text that appear to capture key thoughts (initial analysis). The initial codes were established, and these categories were organized into groups of codes and into meaningful clusters related to the aim. After discussion within the research team, two main categories and one subcategory emerged. All authors read and discussed the result to ensure their consistency to the study’s aim until consensus was reached to increase its trustworthiness.21,22 To enhance the credibility, the research team discussed the interpretation of the data and also representative quotations during the research process.23,24 Careful considerations of the illustrated quotations in the study were applied, to not jeopardized the confidentiality. 25 Quotations represent a selection, accurately reproduced, from different participants, increasing transparency and trustworthiness of the findings and the interpretation of the data. 26
Rigor
To improve the quality of the findings, Lincoln & Guba's trustworthiness criteria were used. 20 The interview guide provided dependability to ensure that certain areas were discussed. To increase the credibility of the study, representative quotations were illustrated. The first author (EB) contributed to the analysis and improved confirmability by attending data analysis meetings and exchanging criticisms in the research group. Furthermore, the data analysis and conclusions were shared with two senior qualitative researchers (JD & ASS) and the research group, who approved the findings and analytical processes. The research team consists of three endocrine surgeons and two registered nurses (PhD). To enhance transferability, a description of the participants and setting was presented.
Results
Sixteen patients participated in the study. The results were based on interviews from 16 patients (12 women) with an average age of 59 years (range 24-83 years). The sample size was appropriate due to the qualitative method used17,18 and we aimed for a variation regarding characteristics (Table 1). Patients’ symptoms and size of goiter removed are shown in Table 2. The inductive analysis of the interviews yielded two main categories and one subcategory, describing the patients’ early experiences of symptoms after hemithyroidectomy. The two main categories were: Early postoperative symptoms that caused disadvantage in daily life and Postoperative symptoms and coping strategies and one subcategory: Early postoperative experiences of concerns about the future.
Patient Characteristics [n = 16].
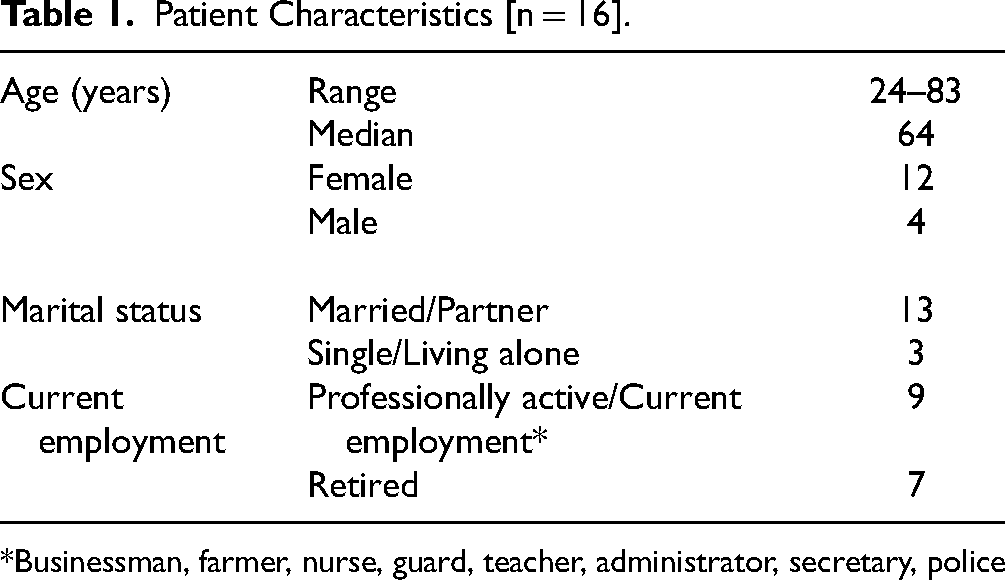
*Businessman, farmer, nurse, guard, teacher, administrator, secretary, police
Patients’ Symptoms and Size of Goiter Removed.

Main Category: Early Postoperative Symptoms That Caused Disadvantage in Daily Life
The first main category illustrated the symptoms that the patients experienced and how those symptoms affected their daily life. Patients expressed swallowing difficulties, voice impairment, pain and also general symptoms from the surgical wound, such as swelling, movement restrictions of the neck and feeling lumpy.
Having a lumpy feeling and a painful sensation when swallowing was common. Difficulties connected with drink and food intake were common topics, wherein patients had experienced problems with nutrition. For example, patients tried to live as usual, but often became aware that this was not possible. “I drank water yesterday and then I tried to drink as usual. Then I figured out that it kind of stopped and then I had water up in my throat, because it didn't have time to come down.” (Patient 7)
Social situations were described to be troublesome when voice impairments were encountered. Some patients were not able to communicate with their partner, their relatives or going out with their pet. Voice impairments distance the patients from family and friends and affected their ability to interact in different social environments such as social gatherings or singing. “I mean, I can't strain my voice. I can't go into a debate or a discussion where I wanted to point something out with my voice.” (Patient 1) “Yes, hoarse and then that voice could almost go away. Or, I felt like I was getting a weaker voice. And I feel I'm grateful I have the voice, but if I try to sing or something, I can't.” (Patient 12)
Prolonged pain after the surgery generated extended sick leave and additional contacts with the health care system. Referred pain to the nearby regions was described for example earache or shoulder pain. Patients experienced pain when swallowing or talking, because of the surgical affection on anatomical structures of the neck, such as the pharynx and larynx. “I didn't feel much pain relief in the moments afterwards, but I was in a lot of pain and it hurt a lot to talk. It hurt a lot to eat. The first few days I had a lot of difficulty eating and talking.” (Patient 14) “But what I felt most was that it felt like a sore throat when I swallowed.” (Patient 2) “I was in a lot of pain, by the way, the first few days. Both here and then, shoulders and neck something absolutely terrible.” (Patient 13)
Some of the interviewed patients had experienced complications after the surgery such as bleeding, nerve paresis, tingling and numbness in hands and feet, atrial fibrillation and hypertension. Post-operative hoarseness and cough gave the patients shame feelings as these symptoms mimic Covid-19 infection symptomatology. Some patients had an extended hospital stay, being in a dependent position from the healthcare personnel and resulting in loss of independency. The complications gave rise to existential thoughts and doubts about performing the surgery. “So if someone asked me, I would say ‘I wouldn't redo it’. With hindsight, maybe, I should have backed off.” (Patient 6)
Main Category: Early Postoperative Symptoms and Coping Strategies
The second main category outlined how the patients cope with the early subjective postoperative symptoms. Difficulties to swallow solid foods, forced the patients to change their food patterns from solid to soft foods and warm beverages. “The first meal at the hospital was a really soft omelet with ham sauce, and it was standing on the menu at home because it was easy to swallow.” (Patient 14)
Voice impairments led to impair ability to talk so patients developed other methods of communication such as sending sms messages from their mobile phones instead of talking or writing down thoughts at home instead of talking to their partner. Patients developed coping strategies trying to maintain their voice intensity with diminishing their talking to not talking at all. “Of course I don't want to talk with this voice to my family. They said “are you sick or do you have a cold or something?” (Patient 9)
Patients reported the feeling of a lump on the wound and tightness or being unable to stretch the neck. T-shirts with wide neck were preferred instead of tighter clothes around the neck because they felt like pushing against the neck. Most of the participants described that these symptoms impaired their ability to swallow or move of the head. “My neck tightened a lot when I stretched my head up, which also made me unconsciously maybe go and look down a lot because I didn't want to stretch the wound. And then I realized… Instead, I got a pain in my neck because I was walking and looking down the whole time, instead of stretching.” (Patient 14)
Patients described difficulties moving the head and neck sideways impairing in such a way their ability to look at a blind spot when driving a car. Some patients refrained from driving, and this was a very important feature not being able to perform everyday activities or being dependent on others for transportation help. “But I didn't drive, it took over a week before I got in the car anyway.” (Patient 15) “So, I've tried to avoid actually driving a car, because… Straight ahead there are no problems, but I feel that I'm a little limited in moving my head to the side.” (Patient 11)
Subcategory: Early Postoperative Experiences of Concerns About the Future
The subcategory outlined how patients managed to deal with the future. The patients were concerned about their future to come. The patients who experienced complications after the surgery had anxiety but also thoughts and fears of the future. The patients wonder about the healing process, if their complications were going to be long lasting and when they could start working again. “That's the one I'm most disappointed with. Just this not knowing how long it will be like this. Will it get better? Won't it get better? How to deal with it.” (Patient 6) “But the hard part is that it has started to feel like I have my thyroid back, because I have such a lump. So I've started having a bit of trouble swallowing again.” (Patient 7) “But when I feel the scar, it feels like there is some elevation two centimeters … one centimeter on each side of the wound which is lumpy and hard. But I don't know if it's because it's sewn under, that is what is not fully healed yet.” (Patient 4)
Patients dealing with uncertainty about the future and perceived worries on the final pathological examination. Many patients were concerned if the pathological examination should revile that they have cancer. These thoughts made them question their lifestyle, some kept it secret from family and friends that they were operated and some have had cancer before and they were worried if they would get it again. “Since it is still not 100% determined what type of tumor was removed, then perhaps you can sit and think what the next step is? Because I think as soon as you hear the name cancer or a possible cancer, you automatically … feel a little different. Then you feel worse psychologically.” (Patient 1) “Now we go and just wait for the pathological examination response so that's it.” (Patient 3)
Some patient wondered if the laboratory analysis of thyroid hormones would recommend lifelong substitution, since this would made them dependent on the availability of medicine in crises or war. “It's probably more this feeling that you have a dependence to a drug that I can find a bit difficult considering … well, you get a lot of bad thoughts with war and what happens if you don't get your medicine?” (Patient 11)
Discussion
To our knowledge, this is the first study to explore patients’ experiences of symptoms after hemithyroidectomy in the early postoperative phase. The findings show that patients experienced and expressed a variety of symptoms and coping strategies were necessary to endure the daily life. Concerns about the future were common and the postoperative symptoms affected their social relationship. Patients experienced pain from the surgical wound and tightness of the neck after the surgery. Results from a trial 27 highlight that omitting the platysma muscle suturing resulted in significantly less wound-specific pain in the initial postoperative period. Patients interviewed in this study were operated with suturing of the platysma muscle. It would be of special interest to conduct a qualitative study to investigate whether omitting to suture the platysma muscle would result in less tightness in the neck and decrease some of the symptoms experienced by patients. Findings from previous studies of how patients with thyroid and head/neck cancer experienced pain and symptoms, is similar as our results despite a benign situation.28,29 Previous evidence also shows that patients had physical and emotional symptoms, in similarity with our findings.30,31
In relation to the theory HTOUS the symptom experience manifestations reflect pattern manifestations of the human energy field. 11 The patients’ symptoms, despite the benign condition, are of importance for person centered care. Understanding the human experience related to symptoms can provide a holistic understanding of patients essential to guide and enhance clinical practice. Even though the patients in our study did not have a cancer diagnosis, they experience their early postoperative period stressful. Consequentially, to reduce anxiety and distress in patients and relatives, the health care professionals should among other things provide relevant knowledge and supportive care to stimulate the patients to cope easier in the early postoperative period. Evidence shows that shared decision making, between patients and healthcare professionals, around treatment options is important so that patients are fully aware about their management options.30,32 The psychosocial and coping components experienced by the patients due to the symptoms during the early postoperative recovery seemed to be important to be aware of in the health care to tailor the individualized support and care. The strengths of our study are the interviewed patient's diversity of current employment and age and interpreted to enhance credibility. To ensure credibility and trustworthiness of the study's results, each author read, thoroughly discussed, and reflection on the entire analytical process involved in creating main categories and subcategory. The research team consisted of a variety of professions which is interpreted as a strength and has enriched the study's data analysis. Triangulation developed a comprehensive understanding of the research data 17 and increased the credibility and trustworthiness of the study. 33
Furthermore, the findings may guide the professionals to tailored extensive preoperative information to optimize the care for this patient group. Easy-to-understand sources to access information seem to be of importance. 34
Limitations
The interviews were conducted between two-three weeks postoperative to investigate the patients’ experiences in the early postoperative phase. The interviews were face to face, by phone and digital which may have affected the duration of the interviews and influenced the data corpus. Telephone interviews can limit non-verbal communication and make it more difficult with probing. According to previous evidence, postoperative symptoms, such as dysphagia 35 tend to resolve spontaneously after the first year. However, even in benign conditions, the patients’ perspectives are of great importance to capture to conduct patient-centered care.36,37 It is of importance to clarify the patient's individual daily life to tailor information and person-centered care to make the patients feel safe and have an optimal recovery. Patients were only recruited from two hospital, which may be a limitation. The sample size can be interpreted as small, but relevant to the qualitative study design and the data corpus. The findings are transferable to other surgery contexts according to trustworthiness criteria transferability. 22 We have tried to illustrate the demographics in detail, the possibility to other researchers to judge transferability of our findings.
Conclusions
Patients experienced early postoperative symptoms that affected their lives in multiple levels, making them develop coping strategies and awaking concerns about the future. The effect of hemithyroidectomy influenced patients’ daily life in the early postoperative phase considerably. The findings may guide professionals to tailored extensive preoperative information to optimize the care for this patient group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
International ethical guidelines were followed, and study participation was voluntary. Oral and written informed consent was obtained before the interviews. The participants were informed that they could discontinue study participation without giving reasons. The data are presented in a way to protect the participants identity. The study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 2023) and the ethical guidelines of the Swedish Research Council. The study was approved by the national ethical committee (Diary number: 2021-06404-02).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.