
Abstract
Patient satisfaction is important in healthcare as it affects the quality of care and can lower costs in hospitals. This study aimed to measure immigrant satisfaction with outpatient services at Firoozabadi Hospital's pediatric clinic. Data were collected from immigrant patients from January to July 2023. The Patient Satisfaction Questionnaire 18 and the personal information checklist were used in oral interviews with caregivers. The overall satisfaction score was 72.95 out of 90, with a standard deviation of 12.57. Financial issues received the lowest satisfaction scores, while interpersonal manner received the highest ratings. Out of the 241 respondents, 48.6% were completely satisfied, 32.7% were satisfied, 10.6% had no opinion, and 4.4% expressed dissatisfaction. Satisfaction levels were not correlated with income, education, possession of identification documents or health insurance, and length of stay in Iran. Overall, most participants were happy with the outpatient services, but many lacked health insurance. Providing easier access to health insurance for immigrants could help reduce dissatisfaction with expensive medical bills.
Introduction
Healthcare systems worldwide are dedicated to delivering high-quality care, a mission that not only benefits individual health but also contributes to the broader economic and social well-being of society. 1 In the pursuit of this objective, the measurement of patient satisfaction has emerged as a crucial tool for evaluating the effectiveness of healthcare services provided within medical facilities. 2
Studies have consistently shown that heightened levels of patient satisfaction correlate with improved healthcare quality and increased operational efficiency. This connection translates into better treatment outcomes, reduced mortality rates, 3 and shorter hospitalization durations.4–6 Moreover, patient satisfaction has been linked to a decreased demand for intensive care, hospitalization, 7 and laboratory services, thereby underscoring its far-reaching impact on healthcare resource allocation and utilization. 8
Patient satisfaction is a multifaceted concept influenced by several critical factors. These factors encompass effective doctor-patient communication, 9 waiting times, healthcare costs, 10 interactions with other healthcare providers, and various sociodemographic variables such as age, 11 gender, 12 income, and educational attainment. 13
According to the 2022 International Migrant Report, Iran ranks among the top 10 countries globally in terms of hosting refugees. Furthermore, in 2020, the migration of Afghans to Iran stood out as the 7th most significant country-to-country migration worldwide. 14 It is noteworthy that immigrants often encounter barriers in accessing healthcare services, a concern highlighted by the fact that they typically receive fewer health services compared to the general population. 15 This vulnerable population is also at an elevated risk of noncommunicable diseases and mental health issues, further accentuating the importance of addressing their healthcare needs. 16 Additionally, immigrants can pose challenges related to the potential spread of infectious diseases within the population. 17
An examination of the health status of immigrant children compared to native Norwegian children revealed disparities, with immigrant children experiencing a higher prevalence of certain health issues, including infectious diseases, obesity, nutritional deficiencies, skin conditions, blood disorders, and reproductive health problems. Notably, systematic reviews have indicated that immigrant children often arrive in receiving countries with elevated rates of anemia (14%), tuberculosis (11%), and vitamin D deficiency (45%).
During the recent COVID-19 pandemic, studies have established a connection between illegal immigrants and the occurrence of COVID-19 outbreaks and associated fatalities. 18 In Iran, research has indicated that immigrants face a heightened risk of mortality due to COVID-19. 19 Moreover, a substantial portion of specific infectious diseases in Iran, including multidrug resistant tuberculosis (55%), malaria (44%), tuberculosis (29%), and Crimean-Congo fever (25%), are linked to Afghan immigrants. 19 Additionally, diseases such as cholera, 20 leishmaniasis, 21 and hepatitis B 22 are prevalent among the Afghan immigrant population residing in Iran.
Research investigations into the healthcare experiences of immigrant patients have highlighted several significant barriers and facilitators in healthcare centers. Notably, language disparities, inadequate training of healthcare providers, and a dearth of available translators have posed substantial challenges to delivering effective healthcare to immigrant populations. 23 Enhancing healthcare services for immigrants has been distilled into 2 crucial principles: establishing empathetic patient-provider relationships and fostering clear and effective communication channels. 23
In Iran, various initiatives have been implemented to improve healthcare access and quality for immigrants. Irrespective of possessing identification documents, immigrants can avail themselves of essential healthcare services free of charge. 24 These services encompass vaccinations, prenatal care, family planning, psychological and nutritional counseling, tuberculosis treatment, and antiretroviral therapy for HIV. 25 Moreover, access to treatment and rehabilitation services is extended to immigrants, with costs determined by their insurance type. 26 In a significant development, Iran expanded its Universal Public Health Insurance program in 2015 to encompass all immigrants possessing valid identification documents, thereby broadening access to healthcare services for this vulnerable demographic. 27
The World Health Organization (WHO) underscores the imperative of enhancing the quality, accessibility, affordability, and acceptability of healthcare services for migrant populations. 28 These principles align with the Sustainable Development Goals, which prioritize the achievement of healthy living for all and the improvement of health across all age groups, including immigrants. 29
It is essential to recognize that findings from studies conducted within a specific country regarding patient satisfaction may not be directly transferable to other nations due to contextual differences. 30 In Iran, numerous studies have explored patient satisfaction with medical services over the years. 31 However, there remains a notable dearth of research in the realm of immigrant satisfaction with healthcare services. Given that outpatient services represent the initial point of interaction with the healthcare system, assessing immigrant satisfaction at this juncture holds significant potential for enhancing both hospitals and the broader healthcare system. 32 Additionally, considering the vulnerability of immigrant populations, which includes a higher prevalence of infectious and mental health conditions, appropriate interventions in this domain have the potential to ameliorate some of the healthcare system's challenges.
This study endeavors to evaluate the satisfaction of immigrants with outpatient services offered at the pediatric clinic of Firoozabadi Hospital. The outcomes of this research have the potential to offer valuable insights for healthcare professionals, policymakers, and hospital administrators. These insights can inform the design of targeted interventions aimed at improving the healthcare experiences of immigrant populations.
Method
This study adopts a cross-sectional research design, employing both descriptive and analytical methods to investigate the topic. The research sample comprises children of immigrants, specifically Afghan nationals, aged between 0 and 18 years. These participants were referred to various pediatric clinics within Firoozabadi Hospital, encompassing general pediatric care as well as specialized clinics for nephrology, endocrinology, infectious diseases, neonates, and neurology. The data collection period for this study spanned from January to July 2023.
To determine the sample size required for estimating the satisfaction average, several parameters were considered. A confidence level of 95% and an estimation accuracy of 8.0 were selected for the calculation. Additionally, the maximum estimated standard deviation from previous studies was set at 6.40. The following sample size formula was employed for this purpose: n represents the sample size. Z denotes the confidence level, which corresponds to a Z-score associated with a 95% confidence level. σ represents the estimated standard deviation. d signifies the estimation accuracy.


Data Collection
To account for potential response bias, data distortion, or incomplete responses, a total of 251 participants were included in this study. The inclusion criteria specified that participants must be immigrants with children aged between 0 and 18 years who sought admission to the clinic. Exclusion criteria were applied in cases where participants demonstrated a lack of willingness or cooperation in responding to the survey questions. Furthermore, individuals who skipped more than 1 question were excluded from the final analysis.
The study's procedure commenced with a comprehensive explanation of the research objectives to the participants’ companions. Subsequently, a structured questionnaire was administered, comprising 2 sections: a personal information checklist and the Patient Satisfaction Questionnaire 18 (PSQ18). Participants were given the option to skip any questions they preferred not to answer, and ask for assistance in understanding any unclear questions at any point.
For parents who brought multiple children to the clinic during a single visit, only 1 questionnaire was collected. However, parents who sought care across different pediatric clinics within the hospital were administered separate questionnaires for each clinic visit.
The personal information questionnaire encompassed inquiries related to insurance coverage, possession of identification documents, duration of residence in Iran, educational background, and income level.
Patient Satisfaction Questionnaire (PSQ18)
The PSQ18 was originally developed by Marshall and Hays in 1994. 33 Comprising 18 questions distributed across 7 subscales, this questionnaire assesses various facets of patient satisfaction, including general satisfaction, technical quality, interpersonal manner, financial matters, time spent with the patient, communication, and accessibility and convenience.
In 2016, Thayaparan and colleagues affirmed the validity and reliability of the PSQ18 questionnaire in diverse research studies. 34 In Iran, its reliability and validity have been substantiated through the work of Mr Ziyai and Mr Zahdenjad, they have reported.35,36 The Cronbach alpha coefficient for this questionnaire is reported at .82, 37 while the kappa coefficient stands at 0.96. 36 Additionally, Dr Theofilou conducted a study to assess this aspect. They found that the coefficient values for the specific variables (a total of 18) were 0.877 or 0.879, considering shared variance, indicating a relatively high level of internal consistency for the items. Furthermore, they noted that removing any variable would not lead to an increase in Cronbach's alpha coefficient. 38
Responses to the PSQ18 are graded using a 5-point Likert scale, where a score of 1 indicates the lowest level of satisfaction, and 5 represents the highest level of satisfaction. Scoring for individual questions ranges from 1 to 5, with some questions using an inverse scale. The total score for the 18 questions ranges from a minimum of 18 to a maximum of 90. Subgroup scores vary, with point ranges spanning from 2 to 10 or from 4 to 20.
Considering the limitations of the 5-point Likert scale such as results may not be objective, some respondents will lean toward a neutral opinion or evaluation, while others will skew toward choosing the most extreme option; various response options were deliberately arranged with differing approaches to minimize the potential for response distortion, including some with a strongly positive orientation and others with an opposite perspective. This strategy aimed to ensure the robustness of the collected data and minimize response bias. Given the established reliability and validity of the PSQ18 and its concise nature, it was selected as the preferred instrument for this study. Its brevity streamlined the data collection process while maintaining rigorous measurement standards.
Data Analysis
The collected data underwent analysis using SPSS version 26 software. Descriptive statistics, including measures of central tendency (mean) and data spread (standard deviation), were computed. The results were also presented in terms of frequencies and percentages to provide a comprehensive overview of the data.
Analytical tests were employed to gain deeper insights into the dataset. The Kolmogorov-Smirnov 1-sample test was utilized to assess the normality of the data distribution, ensuring that the assumptions for subsequent statistical analyses were met. The Kruskal-Wallis test, a nonparametric alternative to the analysis of variance (ANOVA), was applied to examine potential differences among groups.
Results
A total of 251 participants, all of Afghan nationality, were enrolled in this study. Of the participants, 88 were fathers, 133 were mothers, and 29 were other relatives of children. Over half of the participants (54.6%) had prior experience with the pediatric clinic at the hospital, while 44.6% were visiting for the first time. Only 20 participants (8.0%) held medical insurance, while the vast majority (92.0%) did not. Notably, 77 participants (30.7%) lacked any form of identification documents (Table 1).
Characteristics of the Participants.
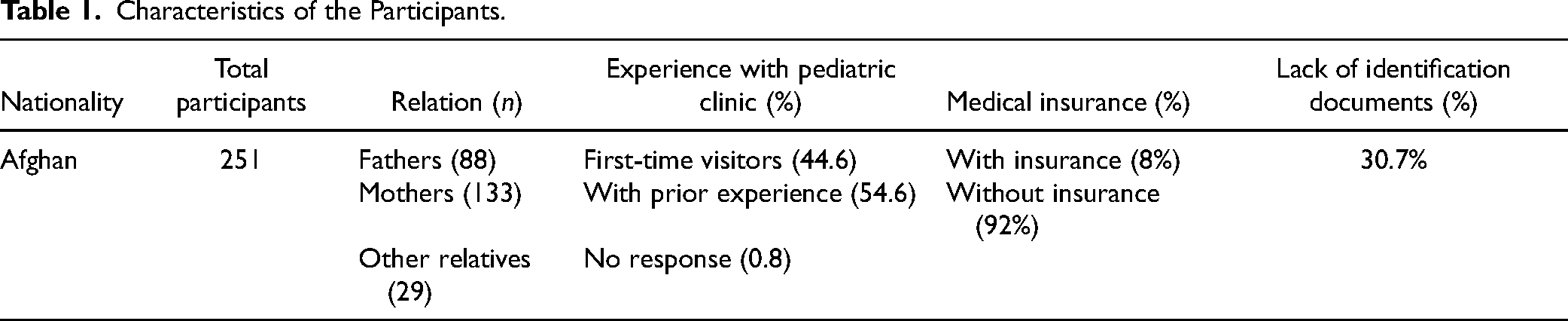
In terms of income distribution, the largest proportion of participants (55.8%) reported earnings between 50 and 100 million Rials per month [100–200 USD]. Furthermore, 70% of the participants had an educational level below a secondary high school diploma. A significant portion of the population (57%) had resided in Iran for more than 10 years.
Regarding family size, the majority of patients (81.3%) came from households with 4 or more individuals. On average, each family had 5.22 members (±2.02).
Patient Satisfaction
The average overall satisfaction of participants with the outpatient services provided in this study was 72.95 out of 90, with a median score of 76.0. The highest recorded total satisfaction score was 90, while the lowest was 20. Among the various aspects of satisfaction, the lowest score was attributed to financial issues, while the highest score was associated with interpersonal manner (Table 2, Figure 1).
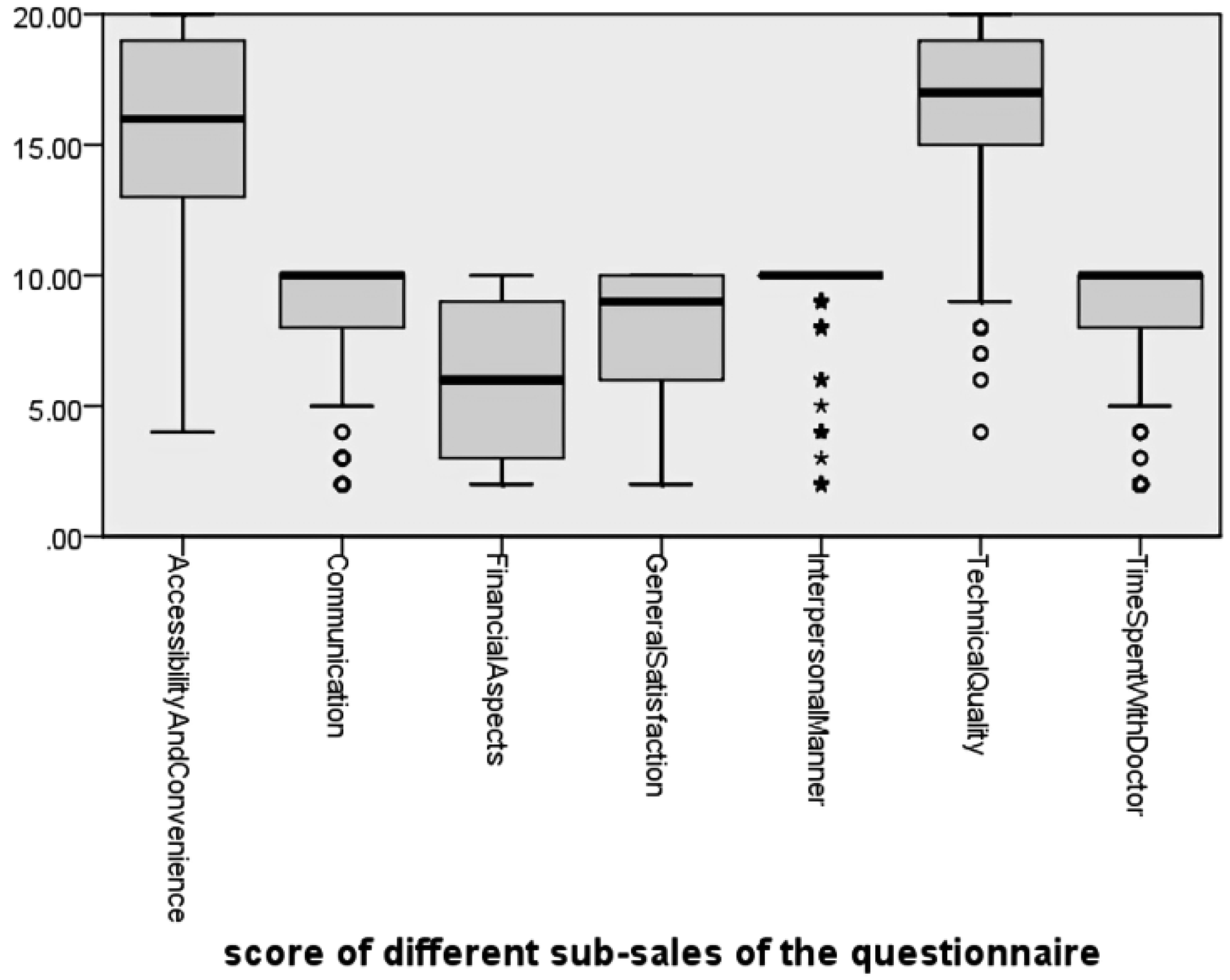
Boxplot of the scores of different subscales of the questionnaire.
Mean Score of Different Subscales of the Questionnaire.

The survey employed a 5-point Likert scale for participants to express their level of satisfaction. Based on the scores assigned by each individual, satisfaction within each subscale was categorized as follows:
Completely satisfied: 145 participants (57.8%) Satisfied: 42 participants (16.7%) No opinion: 26 participants (10.4%) Dissatisfied: 22 participants (8.8%) Completely dissatisfied: 16 participants (6.4%)
These categories offer a comprehensive overview of the distribution of satisfaction levels among the 251 participants who completed the PSQ18 (Table 3).
Level of Satisfaction in Different Subscales.

Statistical Analysis
Due to the nonnormal distribution of the data, nonparametric tests were employed for analysis. The Kruskal-Wallis test was used to explore the relationships between various factors and patient satisfaction. Findings indicated no significant correlation between family income, education level, length of stay in Iran, use of health insurance services, or identification documents with satisfaction scores (P-values = .94, .288, .98, .441, .395, respectively). However, a notable exception was observed in the relationship between family relationships with the child and satisfaction levels, where individuals other than the child's parents showed significantly higher satisfaction levels (P-value = .01).
In summary, the Kruskal-Wallis test revealed no significant associations between most variables and satisfaction scores, except for the noteworthy finding that individuals other than the child's parents had notably higher satisfaction levels. This highlights the importance of considering diverse factors when assessing patient satisfaction in healthcare settings.
Discussion
Our study focused on 251 Afghan immigrants referred to the pediatric clinic of Firoozabadi Hospital. The respondents were primarily companions of the children, with over half being mothers, and the majority of clients had prior experience with the clinic. Most clients lacked health insurance but had valid identification documents, mostly census cards. The respondents had diverse lengths of residence in Iran, with many residing for over a decade. Education levels were generally below a secondary high school diploma, and family incomes predominantly fell between 50 and 100 million Rials per month [100–200 USD].
The results revealed a high level of satisfaction among immigrants with the outpatient services of the pediatric clinic at Firoozabadi Hospital. Over two-thirds of Afghan immigrants expressed satisfaction, with the highest satisfaction related to interpersonal interactions and the lowest regarding financial aspects. 39 Additionally, more than half of the respondents were satisfied across various subscales, including general satisfaction, communication with the patient, accessibility, and convenience, time spent with the doctor, and technical quality. 39 Notably, demographic factors like education level, length of stay in Iran, and identification documents did not significantly impact satisfaction. 39 However, companions other than the child's parents reported higher satisfaction levels. 39 Our findings indicated that the majority of subcategories displayed a trend of decreasing satisfaction levels from highest very satisfied to lower levels. However, financial issues stood out with high levels of both very satisfied and very dissatisfied responses in total population. Additionally, subgroup analysis revealed that 29.9% of participants without health insurance expressed dissatisfaction, compared to only 5% of those with health insurance. This specific factor may be the underlying reason for this discrepancy and could serve as a valuable insight for healthcare policymakers.
Comparing our findings with prior research, a study on outpatients at Ayatollah Taleghani Hospital Clinic in Tehran found that 53.8% of patients were satisfied with their doctor. 39 Another study evaluating outpatient services in 6 military hospitals in Iran reported 96% satisfaction among the population. 40 Furthermore, Mr Pouragha and his colleagues investigated patient satisfaction with outpatient services in 4 teaching hospitals in Tehran, Iran, and found that 61% of patients rated the services as good. 41 The satisfaction level at the center of focus in this study, which is among the primary hospitals frequented by Afghan immigrants, exceeded that of Mr Pouragha and the study of Ayatollah Taleghani Hospital, but it was lower than the level of satisfaction in military hospitals in Iran. This high level of satisfaction could be due to the improvement of medical services over time in Iran, the differences in hospital management, the cultural and social differences, and the level of expectations between immigrants and native Iranian people.
We also explored satisfaction levels among minority populations in different studies across the globe. For example, a study in Germany found that migrant families were less satisfied with outpatient services in a pediatric nephrology clinic than nonimmigrants. 42 Conversely, a study of racial and cultural minorities in a Midwestern region in the United States reported low levels of racism and mistreatment by physicians, coupled with good access to health care. 43 A study in Istanbul revealed that waiting times at hospitals and negative attitudes of healthcare staff reduced satisfaction among Syrian refugees regarding healthcare services. In a study by Kohlenberger and colleagues in Australia, barriers to access to health services for refugees were examined. The most critical barriers included scheduling conflicts, long waiting times, lack of knowledge about doctors, and language barriers, with treatment costs being less frequently cited as an issue. 44 In our study, the greatest satisfaction was related to interpersonal interactions, suggesting that doctors in this clinic establish empathetic and respectful relationships with immigrants. Unlike the study in Istanbul, immigrants in our study did not express concerns about long waiting times in the clinic. However, unlike the study in Australia, the financial aspects of healthcare in this clinic were not satisfactory for them.42–44
Although some studies have established a relationship between sociodemographic indicators and patient satisfaction.,30,45 we found no significant correlation between education level, length of stay in Iran, identification documents, and the level of satisfaction. 39 The sole significant finding was that companions other than the child's parents reported higher satisfaction levels. 39
For future research, we strongly suggest expanding the inclusion of centers that primarily serve immigrant populations. This will not only increase the number of participants but also allow for a more diverse representation of immigrants from various geographic regions and nationalities.
Conclusion
The subscale with the highest dissatisfaction in our study was financial issues. More than 90% of immigrants lacked health insurance services. Over half of the families had an income between 50 and 100 million Rials per month [100–200 USD]. Considering this issue, any treatment cost was considered expensive for them. 39 The issue of high medical expenses for immigrants requires the participation and consultation of hospital managers, politicians, and experts in the fields of health and the economy to reduce dissatisfaction with high treatment costs. 39 It seems that, if we think of solutions for immigrants to benefit them from health insurance services, it is possible to reduce dissatisfaction with high medical costs. 39
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Standards
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Our research involves human participants; We hereby confirm that written, informed consent has been obtained from the patient, for the publication of his/her case and related information. The purpose of obtaining this consent is to ensure the patient's involvement in contributing valuable medical knowledge and to promote advancements in healthcare practices. It is understood that all personal identifying information will be kept confidential, and the case will be presented anonymously. The study was approved by the ethical committee of the Iran University of Medical Sciences with the ethical code of “IR.IUMS.FMD.REC.1401.539.”
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.