
Abstract
Research surrounding tumor boards has focused on patient outcomes and care coordination. Little is known about the patient experience with tumor boards. This survey examined aspects of the patient experience for patients presented at our multidisciplinary endocrine tumor board (ETB). A 15-item survey was distributed via the online patient portal to patients over the age of 18 whose case had been discussed at our ETB over an 18-month period. Descriptive statistics were reported, and a Fisher's exact test was used to examine relationships between variables. A total of 47 patients completed the survey (46%). A majority (72%) report their provider explained what the ETB is, and 77% report being informed their case would be discussed. Most patients were satisfied their case was being discussed (72%). A number of patients did report moderate or severe anxiety knowing their case was being discussed (15%). Sixty-four percent of patients report the ETB recommendations were clearly explained; however, satisfaction with the recommendations was slightly lower (53%). Despite the somewhat low satisfaction with the recommendations, 75% of patients felt more confident in their treatment plan knowing their case was discussed. Finally, if given the chance, 66% responded that they would have been interested in participating in their own ETB discussion. This study provides some insight into the patient experience surrounding tumor board discussions. Overall, patients are satisfied when their case is discussed at ETB. Patients can also experience anxiety about these discussions, and many patients desire to be present for their own discussions.
Introduction
Multidisciplinary tumor boards are commonplace and considered essential in caring for complex cancer patients. 1 They provide a forum for providers to discuss individual patient cases, generating optimal diagnostic and treatment plans. 2 Research surrounding tumor boards has focused primarily on patient outcomes and care coordination. Multiple studies have shown that multidisciplinary tumor boards result in improved adherence to clinical guidelines, faster time to treatment after diagnosis, as well as improved survival.2-5 Additionally, tumor boards can ensure high-value care by preventing unnecessary tests or procedures. 6
Patient involvement and empowerment has been recognized as a core principle of multidisciplinary cancer care from large scientific societies. 1 Despite ample research on tumor boards, there is a paucity of data examining the patient experience as it relates to tumor boards. One study found that a minority of patients even knew their case was going to be discussed at tumor board, which had a negative impact on the way patients perceived collaboration between their providers. 7 When patients were aware of tumor board discussions, it resulted in increased anxiety.7,8 Additionally, patient preferences are frequently not discussed at tumor boards. 9 Finally, there has been resistance to involving patients directly in tumor board discussions for various reasons. 7 These studies suggest that patients are not being involved or empowered in this aspect of multidisciplinary cancer care. More research is needed to better understand the interaction between tumor boards and the patients they serve.
Endocrine tumor boards (ETBs) are potentially less common than tumor boards in other disciplines and represent a unique type of tumor board.6,10 There is considerably less research surrounding ETBs. A multidisciplinary ETB was established at our NCI-designated comprehensive cancer center in 2016. This tumor board convenes monthly, consisting of endocrinologists, endocrine surgeons, otolaryngologists, nuclear medicine physicians, radiologists, and pathologists. This tumor board discusses an average of 8–10 patients each meeting. Not all patients with endocrine tumors are presented; only those that a provider believes would benefit from a multidisciplinary discussion. The providers that participate in our ETB frequently report high satisfaction in a number of domains as demonstrated by end-of-year evaluations (unpublished data), consistent with studies of other tumor boards.3,7 Although patients do not attend our tumor board, the tumor board can impact the patient experience in a number of ways. The purpose of our study was to assess patients’ knowledge of and satisfaction with our tumor board through the administration of a web-based survey.
Methods
Population
The study's patient population included any patient over 18 years of age whose case had been discussed one or more times at ETB over an 18-month period from December 2020 to June 2022. Patients were included if they had an active online patient portal through our medical center, as the survey was distributed electronically through this portal; 102 patients met these inclusion criteria.
Study Design
A 15-item survey was designed and reviewed by content experts with prior experience in survey design. The survey consisted of basic demographic and clinical information, as well as multiple choice, Likert-style, and open-ended questions. The goal of the survey was to ascertain the knowledge, beliefs, and satisfaction of patients who were discussed at our ETB.
Approval was obtained from the Wake Forest School of Medicine Institutional Review Board, as well as the Wake Forest Digital Communication Core, which ensures HIPAA-compliant digital messaging. The survey was formatted through the Research Electronic Data Capture (RedCap) survey platform. A description of the survey and a link to complete the survey was distributed to patients via the online patient portal. Participation was voluntary and no patient identifiers were collected, and thus participation in the study implied consent. Survey IDs were assigned to each patient to identify whether a patient had completed the survey. To help improve response rates, an additional follow-up message was sent to patients who had not responded after 2 weeks. After 2 additional weeks, patients were contacted via phone to encourage participation in the survey.
Statistical Analysis
Descriptive statistics such as percentages and raw counts were used to assess patient demographics, background, and personal opinions regarding the ETB. Additionally, because of the overall low sample size, a Fisher's exact test was used to determine relationships between the survey variables. To account for potential non-response bias, specific questions with a response rate under 60% were excluded from analysis.
Results
Among the 102 patients that met the eligibility criteria, 47 respondents completed the survey, of which 29 (62%) are female, 24 (51%) live within the metropolitan region, 30 (64%) report Thyroid Cancer as their primary condition, and 31 (66%) have seen “3 or more” providers within our health system for their condition (Table 1). The remainder of the survey response data can be found in Table 2. Regarding patient awareness of the ETB, 34 (72%) patients report their provider explained what the ETB is, and 36 (77%) report being informed their case would be discussed. Thirty-four (72%) patients report being satisfied or very satisfied knowing their case would be discussed. Seven (15%) patients report moderate to severe anxiety knowing their case would be discussed. Thirty (64%) patients report the ETB recommendations were clearly explained with 25 (53%) being satisfied or very satisfied with the recommendations. Additionally, 31 (66%) patients report themselves and their provider followed the recommendation of the tumor board. When asked if the ETB discussion improved their care, 22 (47%) responded yes, 5 (11%) responded no, and 20 (43%) remained unsure. Encouragingly, 35 (75%) patients responded feeling confident in their treatment plan knowing their case was discussed at the ETB. Finally, if given the chance, 31 (66%) responded that they would have been interested in participating in their own ETB discussion.
Demographics and Clinical Characteristics of Survey Respondents.
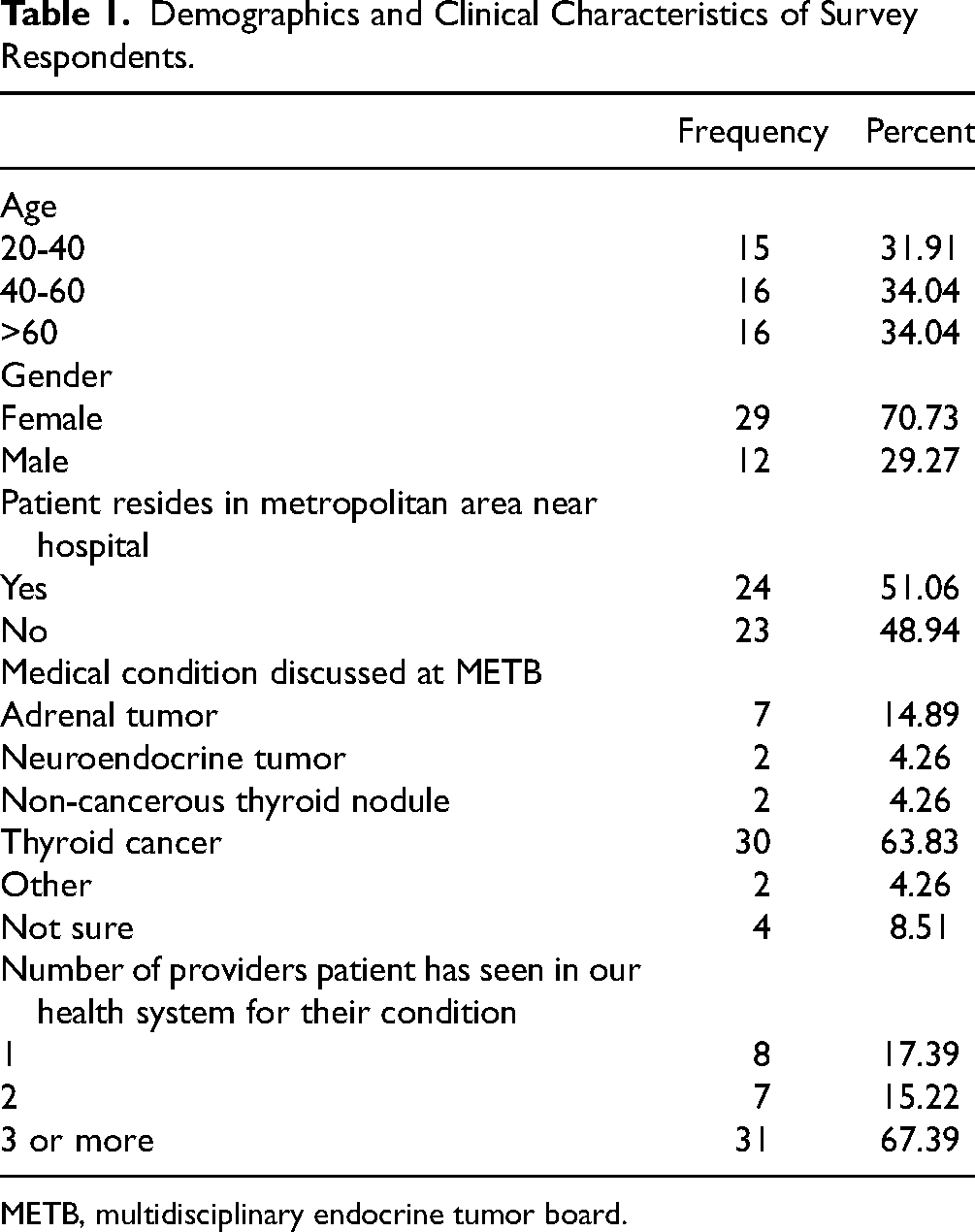
METB, multidisciplinary endocrine tumor board.
Survey Items and Response Data.

Additional Analysis
After testing for associations using Fisher's Exact Test of Independence, we found a statistically significant relationship between confidence in treatment plans and whether ETB recommendations were clearly explained (P = .0307). Specifically, people who reported clear explanations felt more confident in their treatment plans when compared against those without clear explanations (85% vs 46%). Also, despite some missing responses, there is a significant relationship between patient-age and satisfaction with ETB recommendations (P = .019) as well as satisfaction knowing their provider wanted to discuss the case (P = .033). For example, patients aged 40–60 were more satisfied with both the ETB recommendations, and their provider's willingness to discuss their case when compared against older and younger patients (Supplemental Data). There were no other statistically significant associations when examining sex, age, location, and number of providers.
Patient Motivations to Attend Tumor Board
Patients were able to enter a free-text response as to why they would or would not want to be present for the ETB discussion. Thirty-one participants (66%) submitted a free-text response, with 84% of the responses being in favor of attending. These responses can be found in Table 3. For those who wished to attend the ETB, reasons cited include increased transparency and insight into the discussion, the desire to share additional information from the patient perspective, and for increased clarity on the recommendations. The patients who did not wish to be present primarily cited trust in their providers. One patient expressed concern they would not understand the discussion or medical language.
Free-Text Responses Regarding Desire to be Present for Tumor Board Discussion, Organized by Themes.

Discussion
Multidisciplinary tumor boards are very common worldwide.11,12 Assessments of tumor board outcomes have largely focused on diagnosis, treatment, and survival. 3 Limited research has explored patients’ perspectives, experiences, and satisfaction with tumor boards. Furthermore, endocrine-specific tumor boards may not be as prevalent as those in other oncologic disciplines, and as a result, there is a paucity of data. 6 To our knowledge, there have been no studies examining patient experience and satisfaction with a multidisciplinary ETB. With the help of our survey, we hoped to gain some insight into how our tumor board impacts the patient experience outside of the typical outcome-based metrics such as treatment and survival.
Patient satisfaction has become an increasingly important part of cancer care. There are many elements that contribute to patient satisfaction, one of those being clear and effective communication. Clear communication between provider and patient has been linked to patient satisfaction and adherence.13,14 Opportunities exist at multiple time points for clear communication with patients in the tumor board process, including a clear explanation of what the tumor board is, that their case would be discussed, and the recommendations from the tumor board. In our study, most patients felt there was clear communication in these three areas. While greater than 75% of patients were aware their case would be discussed, a lower percentage reported receiving a clear explanation of the recommendations from tumor board. We had theorized that patients who had seen more providers for their condition may have a better awareness of recommendations simply due to increased touchpoints within their healthcare team. However, we did not find a statistically significant correlation between the number of providers and knowledge of the recommendations. This may be attributable to low sample size. There are several potential approaches to improve communication. The tumor board could develop clear expectations for communicating recommendations to patients and provide guidance on how to do so. Documentation of tumor board recommendations in the electronic medical record in the form of a “tumor board note” may be an avenue to increase patient awareness of the recommendations, though to our knowledge, this has yet to be studied. By documenting a tumor board note in the medical record, providers can easily reference recommendations at the point-of-care. Additionally, the tumor board note could be made accessible to patients through their patient portal. However, it is unclear if making the tumor board note accessible to patients would improve the patient experience. Patients may not understand the medical vocabulary in the documentation, leading to confusion. Additionally, reading the recommendations without the ability to ask clarifying questions may contribute to anxiety.
While a majority of patients were satisfied that their case was going to be discussed (72%), only 53% were satisfied with the recommendations from the tumor board. Of note, non-response bias is a potential confounder with the latter measure, as 40% of respondents were missing data for this survey item. Lower satisfaction with the recommendations may be a result of the nature of the cases being discussed. Cases presented at our tumor board are typically more complex, where clear evidence-based recommendations may be lacking. Alternatively, patients with diagnostic dilemmas are sometimes presented, without clear consensus or arrival at a diagnosis. Patient satisfaction reflects how well a patient's perceived outcome matches their expectations. 13 In other words, if a patient has particular expectations, and those expectations are not met, then the patient will be less satisfied. We did not assess our patients’ expectations regarding tumor board recommendations. It is possible these patients were expecting the tumor board discussion to result in a final diagnosis, or even a cure for their condition. When this did not occur, the recommendations did not meet the patients’ expectations, and thus they were less satisfied.
Anxiety is prevalent in patients with cancer. One study had observed increased rates of patient anxiety at the time of tumor board discussion. 8 It is not clear why; however, it was postulated to be related to uncertainty in next steps. Among those who responded to our survey, 61% reported no anxiety, while the remaining respondents had varying degrees of anxiety from mild to severe. Given the relatively high prevalence of anxiety, it is important to recognize and acknowledge this when discussing tumor board with patients, both before and after the tumor board takes place.
One of the potential challenges or limitations of tumor board discussions surround the fact that the patient is not typically present to express their goals or point of view. Nurse navigators and social workers are sometimes utilized as representatives to help convey patient preferences and priorities. Some tumor boards have tried to implement patient attendance, citing improved patient education and satisfaction. 15 The results to our survey showed that a large percentage (66%) of our patients wanted to be present for their own tumor board discussion. There are numerous logistical hurdles to achieve this, including maintaining patient privacy (cannot discuss cases in front of other patients), coordination in order to accommodate patient presence, and the added time it would take to incorporate patient perspective and answer their questions. Furthermore, there are concerns about how the presence of the patient may impact the discussions that occur. Would providers be less likely to share their thoughts knowing the patient was present? How would the presence of the patient change the group dynamic, and would this, in turn, impact the outcomes of the discussions in a negative way rather than a positive one? Finally, would the patient feel comfortable enough to speak up, or would the environment be too intimidating? These are all questions to be considered, and ultimately studied, if patients begin to attend multidisciplinary tumor boards.
There are several limitations to our study. While the survey response rate approached 50%, the overall sample size was small. As such, we could not fully explore relationships between many of the variables. Furthermore, some survey items had poor response rates, potentially contributing to non-response bias. It is possible respondents did not answer certain questions based on previous responses. For example, if a participant was not aware their case was going to be discussed at tumor board, they wouldn’t have experienced anxiety knowing it was being discussed. Therefore, they may have self-selected the appropriate questions for them, leaving some of the survey items unanswered. While recall bias was a concern, we tried to mitigate this by limiting survey participants to those presented at tumor board in the last 18 months. Our survey had equal age distribution; however, the majority of respondents were female, possibly contributing to selection bias. Finally, we did not collect additional demographic information on race/ethnicity, education, or socioeconomic background.
There are plenty of opportunities for further research. Our findings reflect a single type of tumor board at a single institution. Additional studies could assess similar metrics among other ETBs, as well as tumor boards in other specialties. Quality improvement studies to optimize communication regarding tumor board recommendations may be beneficial. Given the strong desire for patients to be present, effective strategies for involving patients in these discussions are needed.
In conclusion, our findings help contribute to a better understanding of the patient experience surrounding ETB discussions. Specifically, we find it encouraging that most patients report clear communication from providers, overall satisfaction, and high confidence with ETB discussions and decisions. Providers should be aware that patients may experience anxiety knowing their case is being discussed. Finally, most patients expressed interest in being physically present for their case discussion, suggesting the need for innovative ways to involve patients in the tumor board process.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241229383 - Supplemental material for Multidisciplinary Endocrine Tumor Board: Assessment of the Patient Experience
Supplemental material, sj-docx-1-jpx-10.1177_23743735241229383 for Multidisciplinary Endocrine Tumor Board: Assessment of the Patient Experience by Matthew A Gorris, McKenzie L Needham, Kayla C Finnegan, Corey S Obermiller, Lauren Witek, Reese W Randle and Cynthia A Burns in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Wake Forest School of Medicine Institutional Review Board, North Carolina, United States.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
All procedures in this study involving human subjects were conducted in accordance with the Wake Forest School of Medicine Institutional Review Board (IRB00084647).
Statement of Informed Consent
Participation in this anonymous electronic survey study was voluntary, and thus informed consent was implied. No verbal or written consent was obtained.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.