
Abstract
Understanding human functioning and disablement, the contributing factors and their interactions in individuals with tetraplegia is important since elective upper extremity (UE) reconstructive surgery is now offered earlier after injury prior to full recognition of what lies ahead. Qualitative and quantitative data were available from a prior series of mixed methods studies, including a case series design capturing the patients’ lived-experience perspectives of nerve or tendon transfer surgery, or not as the case may be. The objective of this study was to perform secondary data analysis to determine whether the recommended outcome tools being used by clinicians reflect the all important domains of functioning identified by people with tetraplegia who were considering UE reconstructive procedures. The original 18 candidate themes derived from qualitative analysis were reviewed in retrospect, along with a content analysis of the tools’ questions, undertaking word mapping links to the ICF taxonomy. The outcomes tools included in the content analysis were the Canadian Occupational Performance Measure, the Capabilities of Upper Extremity Questionnaire, The Personal Wellbeing Index, and the Grasp and Release Test. Comparison between clinical outcomes tools and the patient lived-experience data uniquely identified links to Chapter1 (b) Mental functions, which include consciousness, orientation, temperament/personality, energy/drive, and higher-level cognition.
Introduction
Advanced reconstructive surgical interventions, including nerve transfer (NT) and/or tendon transfer (TT) procedures, can be used to increase upper extremity (UE) function for individuals with tetraplegia, specifically mid-cervical level spinal cord injury (SCI). This improves the individual's ability to perform activities of daily living without the need for adaptive equipment or orthoses.1,2 Recent muscle reanimation procedures using NTs are offered far sooner than traditional TTs, requiring clinical assessment, selection, and decision-making to occur as early as 3 months postinjury.3–6 It is important that health professionals provide expert knowledge to inform key decisions in a person's rehabilitation, determine areas of UE function requiring intervention, create the assessment tools, and even mediate to some extent what shapes “successful” outcomes.1,7 However, the interface between clinicians’ expert knowledge, assessment processes, and shared decision-making for vulnerable individuals with SCI requires careful reflection. 8
With the advent of new and time-limited NT surgeries, significant procedural issues have been raised in terms of evaluation of suitability for UE surgery, shared decision-making processes, referral systems, determining outcomes of interest, approaches to person-centered goal setting and guidelines for best practice, whereby harm is minimized. 9 The justification for more research in this area is linked to an ethical dilemma of offering early elective surgery to people with tetraplegia before they can fully comprehend the daily impacts of living with their disability.8,10
Results of mixed methods, convergent design research exploring the unique intersection between arm/hand surgical reconstructions, intervention timing, physical assessment processes, and the life impacts described by individuals with tetraplegia have been reported previously.8–10 These publications include the primary qualitative analysis using a data-driven inductive reflexive thematic analysis as per Braun and Clarke, 11 details about the utility, feasibility and psychometric properties of the 4 recommended outcome measures and the pre-post score changes following UE surgery, 10 as well as the transformative analysis when integration of the findings using the Stewart Model of Care, drawn from palliative health, enabled the interpretation of higher order messages. 8
The purpose of this paper is to report the secondary analysis from this body of work to determine whether the suite of recommended patient-reported outcome tools capture fully the important aspects of lived-experience in individuals with tetraplegia undergoing UE reconstructive surgery. This involved performing a content analysis of each of the 4 outcome measures used by clinicians in New Zealand, alongside the content of the initial descriptive candidate themes from interview data, subsequent word mapping using the ICF taxonomy and final assessment of convergence between these different data for coverage of ICF domains.
Methods
We linked keywords and meaningful concepts of outcome measures used in UE surgery and candidate themes from qualitative interviews of people who did and did not have UE surgery to second or third level ICF classification categories. Inclusion criteria for this study are shown in Figure 1. In total there were 5 data sources linked, 4 were outcome measures and the final source was candidate themes from qualitative interviews.
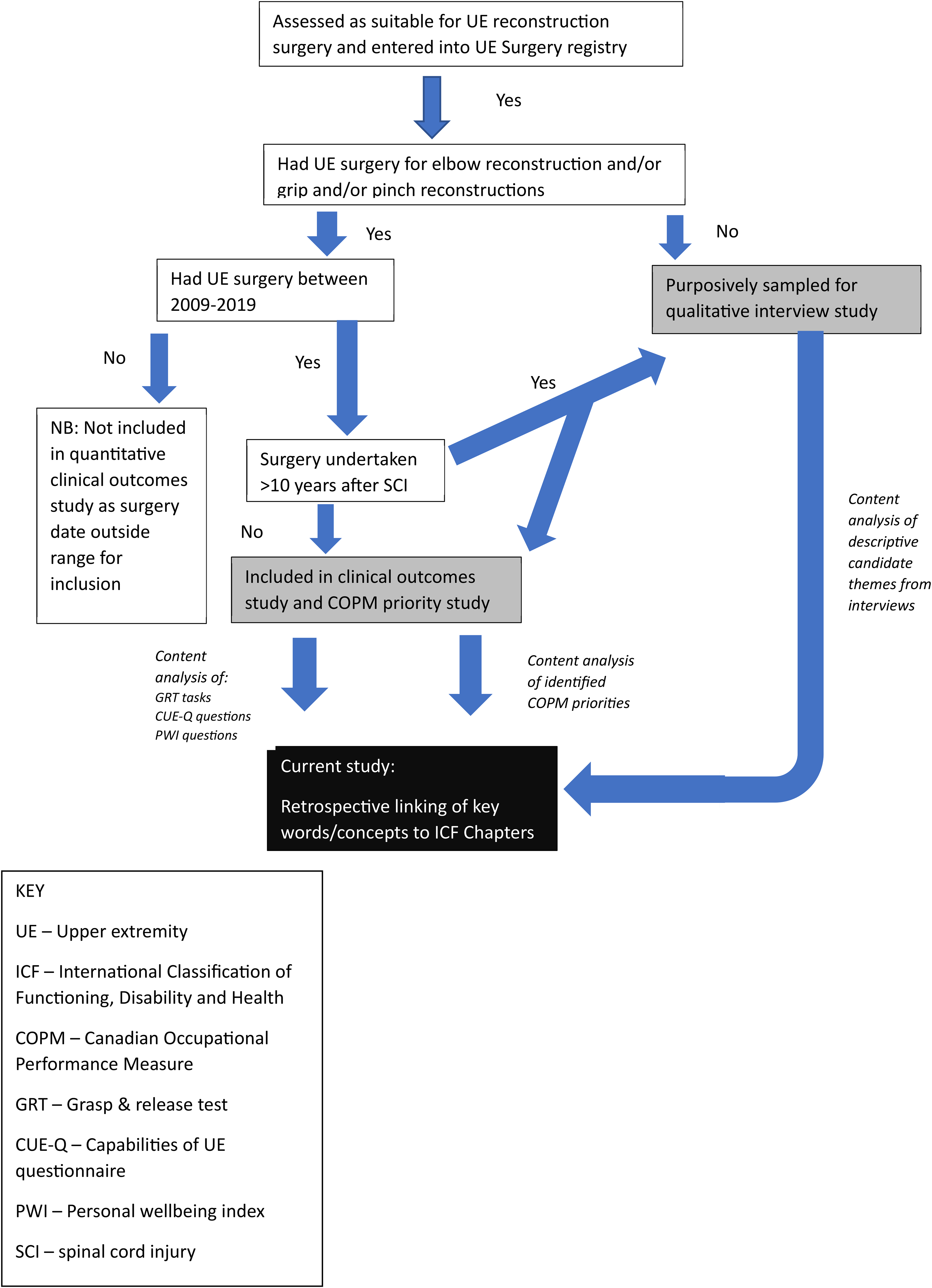
Cohort sampling system.
Outcome Measures
The 4 outcome tools, Canadian Occupational Performance Measure (COPM), Grasp and Release Test (GRT), Capabilities of Upper Extremity Questionnaire (CUE-Q), and Personal Wellbeing Index (PWI), were those in use in New Zealand that were agreed upon by the International Therapist Consensus group in 2009. 12 All data analyzed in this study were derived from New Zealand. First, identified priorities from the COPM 13 were extracted from the International UE Surgery Registry for all people who had surgical reconstructions performed between 2009 and 2019. Secondly, the content of the questions of the CUE-Q, 14 PWI 15 were included in the ICF word-mapping. Finally, each of the 6 tasks of the GRT 16 was evaluated against the relevant ICF chapter content.
Sampling and Recruitment for Interviews
A cohort of individuals with C5-7 tetraplegia, assessed as suitable for reconstructive surgery at the Burwood Spinal Unit between August 2010 and August 2019, was extracted from the New Zealand portal of the International UE Surgery registry. Suitability for surgery was based on classification of the level and extent of SCI neurological impairment using the International Standards for Neurological Classification of SCI (ISNCSCI), 17 including the American Spinal Injury Association Impairment Scale 18 and the International Classification of Hand Surgery for Tetraplegia. 19 From this cohort, potential participants were identified for recruitment for the lived-experience interview study as shown in Figure 1 above. Recruitment was purposive to ensure broad representation in terms of the lived-experience response to the offer of elective UE surgery. Individuals who had elected to accept the offer of surgery many years following SCI, in addition to those who had consistently declined surgery were specifically targeted. All participants were provided with an information sheet and signed a consent form prior to interview. Interview questions were open-ended so that the conversations were ultimately guided by the needs and concerns of participants.
Interview Schedule
A semistructured schedule was used to guide the interview process. All the participants in both the late-to-surgery group and the group who declined surgery were explicitly asked about the selection and assessment process, their decision-making experience and what their advice about UE surgery would be based on current knowledge and life experience to: (a) A newly injured person in the spinal cord injuries unit today and (b) younger self with the benefit of hindsight.
Secondary Data Analysis
For all 5 data sources a word-by-word content analysis was performed and linked to the ICF taxonomy using specific linking rules. 20 This included retrospective linking of keywords and meaningful concepts to second or third level ICF classification from the previously completed qualitative data analysis, the preoperative COPM priorities related to each individual surgical procedure, each question within the CUE-Q and the PWI, and each GRT task. This standardized linking procedure is widely used to qualitatively link content within and between outcome measures and is well known to 1 member of the research team (KASJ), as has been used in previous ICF linking projects.21–24 The ICF linking software was used to map the keywords or phrases to create meaningful concepts. 25 Given the volume of data across ICF domains of Body Structures (s), Body Functions (b), Activity and Participation (d) and Environmental Factors (e) and the 1064 possible ICF categories, the first level links to domain chapters for each category was performed for the outcome tools. Specifically, this data integration step was undertaken to represent the content in terms of human functioning by visually representing the ICF chapter coverage across the 5 data sources.
Both the primary and secondary analysis of narrative data were completed by 2 of the team. These were KASJ as the PhD candidate, a physiotherapist and qualitative researcher in SCI, and RPS 1 of 3 academic supervisors, a psychologist with 40 + years of lived experience of SCI and a recipient of UE surgery. This was overseen by academic supervisor (JAD), who is a clinical expert in the topic-field, and primary supervisor (JWM), who is a rehabilitation physician and professor of rehabilitation medicine.
Results
Word Mapping of the Outcome Measures
COPM Priorities
A total of 885 priorities were identified across all UE reconstructions within the COPM categories of (i) self-care (ii) leisure and (iii) productivity. 26 At a macro word-for-word recognition level, 1213 possible meaningful concepts were identified using the ICF search browser. Irrespective of the context in terms of personal experience, all chapters of the ICF components for Body Structures and Functions, Activities and Participation and Environmental Factors were represented by the ICF categories identified by the participants. Thirty-six priorities were not able to be readily classified using the ICF because they were personal factors. Examples include: To be able to help my baby climb onto my lap, To be able to spend time alone without caregivers.
Capabilities of Upper Extremity Questionnaire
The ICF linking suggests that the CUE-Q predominantly covers the Body Function and Body Structures domains of the ICF. 27 Specifically, the Body Function domain of Chapter 7 Neuromusculoskeletal and movement-related functions, and in terms of Body Structures to Chapter 7 Structures related to movement of the upper limb and/or trunk control, head and neck and the scapula. The CUE-Q also covers, but to a lesser extent the Activity domain including Chapter 4 Mobility-related with reference to Chapter 5 Self-care, Chapter 6 Domestic Life, and Chapter 3 Communication.
Personal Wellbeing Index
The ICF linking suggests Part 1 Q1.1 and Part 2 Q2.3 are designated personal factors and therefore not included in the current ICF taxonomy. Part 2 provides more scope within the taxonomy with coverage of the ICF domain chapters of Activity and Participation, and Environmental Factors.
Grasp and Release Test
From our ICF linking the activities in the GRT shows the most specific coverage in terms of ICF Body Structures and Functions.
Qualitative Interview Data
Semistructured in-depth interviews were undertaken with 18 individuals with tetraplegia, including 6 individuals who had accepted early NT surgery, 5 individuals with over 10 years duration who had arm/hand TT surgery, and 7 individuals who consistently declined surgery. The mean current age of participants was 42 years (range: 22-61 years), with a median time since SCI of 18 years (range: 0.5-36 years). The median time from SCI to surgery for the NT group, who had undergone surgery was 7 months (range 5-9 months), in contrast to duration for the TT group of 18 years postinjury (range 11-26 years). Refer to Tables 1a and 1b for participant characteristics.
Participant Demographics, SCI Characteristics, and Surgery Details.

Abbreviations: ISNCSCI, International Standards for Neurological Classification of SCI; SCI, spinal cord injury; NT, nerve transfer; TT, tendon transfer.
Individuals consented for surgery but had not yet undergone first procedure which in both cases to date was subsequently limited to NT.
Participant's Surgery Procedures Details in Order of Study Group.

SPIN refers to supinator to posterior interosseous nerve transfer.
TROIDS is an abbreviation for Posterior deltoid to triceps tendon transfer.
Thumb and/or finger TTs ± distal split flexor pollicis longus (FPL) tenodesis.
While final themes were created and reported elsewhere, 9 the language of the initial themes was more descriptive and illustrative. The initial candidate theme NVIVO mind map is shown in the Supplemental Material and the ICF chapter links are shown in Table 2 along with the ICF chapter links from the 4 outcome measures. The interview data ICF chapter linkages from the NVIVO mind map included 1 from Body Structures relating to movement (Chapter 7), 3 from Body Functions including seven references to Chapter 1 Mental Functions, 6 out of the possible 8 chapters from Activity & Participation (Chapters 1, 3, 4, 5, 7, 8) and 3 from Environmental Factors where Chapter 3 Relationships and Chapter 4 Attitudes, dominated.
Data Source and ICF Linking to Second (or Third Level Coding if Provided Clarity).

Secondary Data Convergence
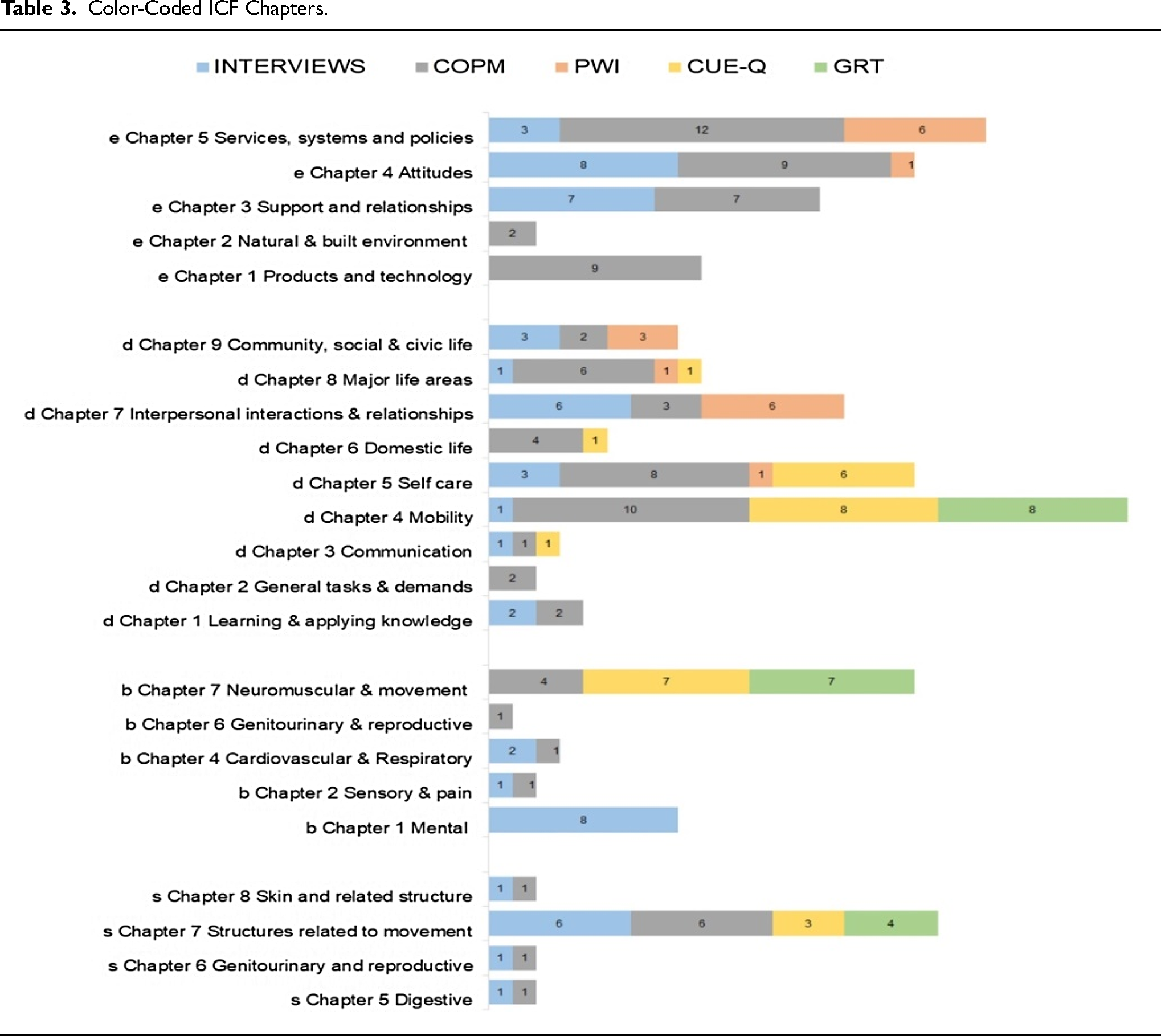
The qualitative interview data was the only source of linkages to Body Functions (b) Chapter 1 Mental Functions (n = 8). In terms of total scores per domain across the 5 data sources Chapter 4 (b) Mobility showed the greatest frequency of ICF chapter links (n = 27) from the 5 data sources. Following this, from the Environmental domain's Chapter 5 (e) Services, systems and policies were next highest with 21 chapter links from three data sources. This was followed by Body Structure's (s) Chapter 7 Structures related to movement (n = 19) and an equal number of links to Body Function's (b) Chapter 7 Neuromuscular and movement (n = 18), Activity and Participation's (d) Chapter 5 Self-care (n = 18) and Environmental domain's (e) Chapter 4 Attitudes (n = 18). All these ICF domain chapters had links to 3 or 4 of the 5 data sources, with the COPM data source making up the majority of the links in these chapters. Both the COPM and qualitative interview data sources provided similar numbers of linkages to the Environmental chapters. The PWI and the interview data shared the majority of activity and participation (d) Chapter 7 Interpersonal and relationships linkages (n = 6). Table 3 represents these ICF chapter links in a color-coded display.
Color-Coded ICF Chapters.

There was 1 significant feature drawn from the 18 interviews of the participants’ collective experience of their own SCI and diagnosis of tetraplegia. Each participant referred back in some detail to their experience of being a patient assessed as suitable for UE surgery. Furthemore each participant was readily able to provide definite feedback about this process in light of the necessity now with newer NT procedures for assessment performed far earlier, and how this would change the decision-making process following SCI. The demands of the decision-making process in terms of higher level cognitive and emotional functions were most evident in the individuals who declined surgery. Examples are provided in Table 4.
Interview Data with ICF Linkages to Mental Functions.

Discussion
The purpose of this paper is to report the secondary analysis which comprised ICF linking to represent human functioning in the context of UE surgery for individuals with tetraplegia. We have attempted to determine whether the domains of human functioning portrayed through in-depth interviews are reflected in the question coverage of the outcome tools in use in New Zealand (the COPM, CUE-Q, PWI, and the GRT). From this study, we have shown that the questions/activities of the CUE-Q and GRT mostly cover the ICF's Body Functions and Body Structures domains, the questions of the PWI that can be categorized cover the ICF's Activity & Participation, and Environmental domains. The self-identified priorities of the COPM cover all domains of the ICF. While individual outcome measures are obviously limited in terms of the dimension of human functioning that is measured, 28 once the lived-experience ICF-linked data was superimposed the picture changed. Without the interview data, the complexity of the patients’ experiences of UE surgery that deals with cognitive and executive functions of the brain would have been omitted. The ICF refers to Mental Function as global mental functions, such as consciousness, as well as the functions of psychic energy and drive, and the specific mental functions, including memory, cognitive-linguistic, and numeracy capabilities. 25
Not surprisingly, the greatest number of links to the ICF from all 5 data sources was Chapter 4 Mobility. These were associated with fine hand use including grasping, manipulating (objects), reaching, and turning or twisting the hands or arms and broader mobility activities include changing basic body position, maintaining a body position, transferring oneself, lifting and carrying objects, moving around in different locations, moving around using equipment and driving. There are clear limitations to the ICF in the context of measurement, not least the absence of personal factors from the taxonomy.29–31 However, the ICF does explore the extent to which human functioning is considered within outcome measures , and as such provides a repeatable systematic evaluation. Given what we know about psychosocial consequences and demands of living with SCI,32,33 the coverage of human functioning excluded Chapter 1 (d) Mental functions unless the patient lived-experience data was viewed. This is particularly important given recent work from our broader research group on SCI in relation to cognition and psychosocial adjustment.34,35 While there are several valid measures to assess cognition and psychosocial adjustment, one straightforward approach for development of future outcome measures might be the creation of an item bank of UE surgery priorities. The clinician-lead interview used with the COPM for priority identification might be an opportunity to address higher executive cognitive demands at play. With the advent of early NT procedures following SCI this is more urgent. This would allow for an individual to be better targeted in terms of what it is they desire for themselves from the surgical reconstructions. This would allow for specific capabilities to be clarified, thereby making the process more acceptable to the individual considering surgery. This is not meant to sound like a “pick and mix” process, rather that functional priorities identified by others before them and “banked” for future identification would at least ensure better integrity in terms of the identification of priorities that extend beyond what might be considered by well-meaning clinicians.
Conclusion
The results of this secondary content analysis showed clearly how the ICF domains of human functioning were largely represented across the different outcome tools, where there was common coverage, where gaps existed and how representative the data sources were in terms of the patients’ lived experience contribution. We know that evidence is stronger for the value of lived-experience research in SCI particularly to ensure that the experience of living with severe disablement is considered. We are not saying that qualitative interviews ought to replace the use of standardized tools. Rather, the clinicians’ evaluation for UE surgery suitability might include careful consideration of an individual's emotional well-being, psychological readiness, and the cogntive demands of the decision-making process. These are important implications for the validity of informed consent under such circumstances, where the influence of clinician confidence on decision-making may dominate.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231211886 - Supplemental material for International Classification of Function, Disability and Health (ICF) Word Mapping to Determine the Human Functioning Associated with Upper Extremity Surgery for Tetraplegia
Supplemental material, sj-docx-1-jpx-10.1177_23743735231211886 for International Classification of Function, Disability and Health (ICF) Word Mapping to Determine the Human Functioning Associated with Upper Extremity Surgery for Tetraplegia by K Anne Sinnott Jerram, Jennifer A Dunn, Richard P Smaill and James W Middleton in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735231211886 - Supplemental material for International Classification of Function, Disability and Health (ICF) Word Mapping to Determine the Human Functioning Associated with Upper Extremity Surgery for Tetraplegia
Supplemental material, sj-docx-2-jpx-10.1177_23743735231211886 for International Classification of Function, Disability and Health (ICF) Word Mapping to Determine the Human Functioning Associated with Upper Extremity Surgery for Tetraplegia by K Anne Sinnott Jerram, Jennifer A Dunn, Richard P Smaill and James W Middleton in Journal of Patient Experience
Footnotes
Acknowledgement
We dedicate this body of work to the late Dr Richard Smaill, who died on 30 May 2023 during the review phase of this final manuscript. Richard’s contribution to this academic body of work, and many more in the SCI lived-experience research field, is unprecedented, given his professional background in organizational psychology. Aroha nui - kia kaha.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Canterbury District Health Board Ethics Committee (RO 14063-A1).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Burwood Upper Limb Surgery Endowment Fund (grant number n/a).
Informed Consent Declaration
Informed consent was obtained via the opt-out option for data collection as per the Canterbury District Health Board Ethics Committee
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.