
Abstract
Introduction
Medical uniforms have been worn since medieval times. From the fifteenth to nineteenth centuries, physicians wore “plague costumes” and black “frock” coats. As medical education became more formalized and teaching institutions were founded, the attire changed to white clothing to signify cleanliness. In the 1970s, green and blue colored scrubs were introduced as uniforms. 1 Modern traditional physician attire has evolved to business formal attire with a white coat.
Physician attire may impact patients’ perception of how knowledgeable, approachable, and trustworthy their physician is during a patient care encounter.2–5 Nonverbal communication occurs through facial expressions, body language, gestures, and physical appearance. Physical appearance, including physician attire, is one of the first nonverbal communications that patients can evaluate during an encounter. Physician attire is recognized as an increasingly important area of study that can influence patient preferences and perceptions.
Studies obtained prior to the coronavirus disease 2019 (COVID-19) global pandemic revealed adult patient preference for physician attire favored a white coat paired with professional clothing.2,6 A 2017 multisite study of over 4000 surveyed adult patients examining patient preference of physician attire resulted in 53% of respondents reporting physician clothing was important to them, with the majority of this subset noting physician clothing affected their satisfaction with care received, and formal attire with a white coat being the preferred clinical attire among survey respondents. 2 A 2015 review article of 30 qualifying articles which included over 11 000 patients, found that patient preferences of physician attire were affected in 70% of the studies, and that formal attire with white coats was preferred in 60% of the studies, however, these results were influenced by age, setting, location, and clinical context. 7 In a study of 299 patients in Malaysia, patient preferences were based on perceived infection risk and the belief that a white coat may represent increased sterility and cleanliness. 8 A study of 443 patients in Saudi Arabia in the primary care setting found that physician attire was more important to male patients who were working, educated, urbanites, and married and that 70% of those who valued physician attire recognized it as affecting the patient care relationship. 9 However, a study of 154 oncology patients showed a lack of patient preference when studying the effect of physician attire on perceived compassion and professionalism in the palliative care setting in the United States. 10 Nor were there differences identified in patient satisfaction of over 1100 patients in a study of obstetrician/gynecologists encounters when comparing formal attire, casual attire, and scrub suits. 11 There has been recent interest in the effect of COVID-19 on attire in the medical setting. At the height of the COVID-19 pandemic, 1 study conducted in late 2020 and published in 2021 surveyed 368 patients in the outpatient setting and found that scrubs (81%, 298/368) were the most acceptable physician attire. 12
To study if patient perception of physician attire was persistently affected by the COVID-19 global pandemic, we conducted a survey-based study of patients in the primary care outpatient setting in 2022. The primary research aim of our study was to evaluate if there was a difference in patient perspective of physician attire before and after the COVID-19 global pandemic began. We hypothesized that patients would prefer physicians wearing more casual attire in 2022 after the COVID-19 global pandemic began compared to the prior baseline data obtained in 2017 before COVID-19.
Methods
To assess patient preference for physician attire, a paper survey was distributed to patients in an outpatient primary care clinic at Mayo Clinic in Jacksonville, Florida, during 2 separate time periods (2017 and 2022), pre and post the beginning of the COVID-19 global pandemic, respectively. The survey consisted of questions, along with photographs of male and female physicians in 7 different forms of attire along with questions. The attire choices included casual (A), casual with a white coat (B), scrubs (C), scrubs with a white coat (D), formal (E), formal with a white coat (F), and formal attire with a suit jacket (G). Attires A to D were considered casual while attires E to G were considered formal. Patients were asked to choose from the 7 attire options and mark the one they preferred their physician to wear in different clinical settings, including primary care, the emergency room, hospital, a surgeon, and what doctors should generally wear overall (Figure 1).

Survey given to patients in the primary care setting.
Self-reported demographic information was obtained through the survey including the survey respondents’ age, gender, level of education, and race. Study participant numbers were determined to achieve statistical significance resulting in a total of 339 patients included in the study.
In 2017, patients were recruited to complete the survey by the nurse during the rooming process prior to seeing the physician. Upon completion, the nurse team gathered the survey and placed it in a collection basket in the staff area of the clinic. In 2017, this process included patients paneled to female physicians, as they were the faculty participating in the multi-site data collection. In 2022, a dedicated research intern expanded the recruitment process to include patients in the waiting room. Upon completion, the research student gathered the survey and placed it in a collection basket in the staff area of the clinic. Patients were provided a written copy of the IRB-approved consent script that the survey was optional, that their care would not be affected in any way by their answers, and that all answers were anonymous and deidentified.
Categorical variables were summarized as frequency (percentage). Fisher's exact test was used to compare the answers between the 2 time periods. Multivariable logistic regression models were used to evaluate the survey answers between the time periods with gender adjusted. All tests were 2-sided with P value <.05 considered statistically significant. The analysis was done using R4.1.2. Mayo Clinic IRB approval for this study was obtained.
Results
Survey data of 339 patients were included in the study. A total of 161 and 178 patients were from 2017 and 2022, respectively. Demographic data revealed there was no significant difference in age, education, and race, but there was a statistically significant difference in male patients in 2017 compared to 2022 (16.0% vs 26.9%, P = .021) (Table 1).
Demographic Data of Survey Respondents.
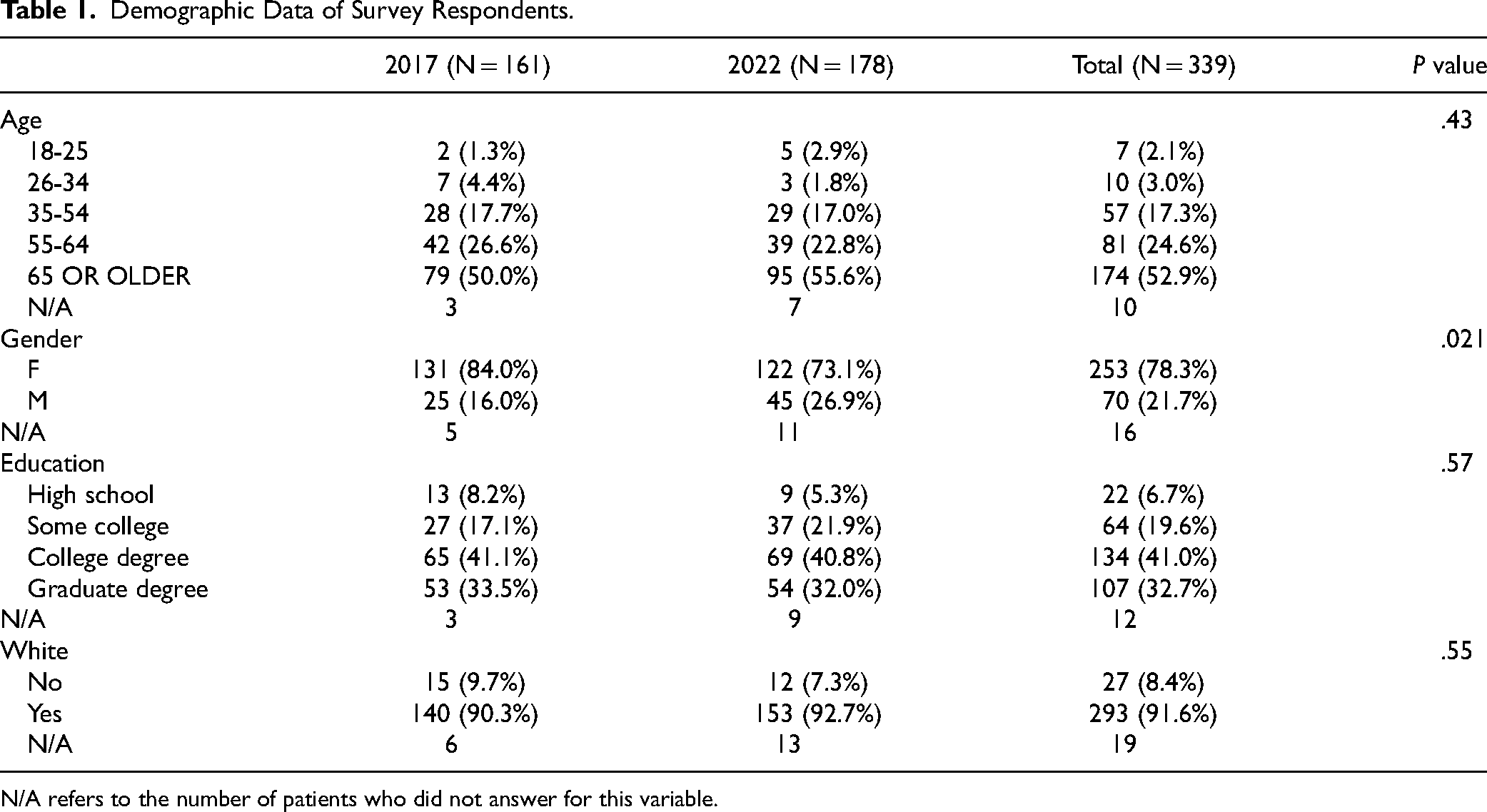
N/A refers to the number of patients who did not answer for this variable.
The comparison of patient preference for formal attire between 2017 and 2022 found there was a statistically significant decrease in the clinical settings of primary care (87.3% vs 75.3%, P = .007), hospital (55% vs 43.7%, P = .046), and overall clinical settings (79.9% vs 64.9%, P = .004) (Table 2).
Comparison of Attire Preference Between Time Periods.

N/A refers to the number of patients who did not answer for this variable.
Subgroup analysis identified statistically significant differences in preferences based on reported gender. Male survey respondents’ preference for formal attire dropped in primary care (90.9% vs 60%, P = .011), emergency room (31.8% vs 6.7%, P = .11), and overall clinical settings (87% vs 55.6%, P = .014), whereas female survey respondents’ preference for formal attire declined mainly in the hospital setting and was close to meeting statistical significance (56% vs 43.3%, P = .055).
When results were adjusted for gender differences using a multivariate logistic regression model, the odds ratio for preferring formal attire were statistically significantly lower in 2022 in the 3 settings of primary care clinic, hospital, and overall clinical settings (OR 0.46, 0.62, 0.45 respectively, with P values .01, .04, and .003) (Table 3).
Multivariable Logistic Regression Model Evaluating the Difference in Survey Answers with Gender Adjusted.

In every setting surveyed, and for all genders, there was notably a preference towards less formal and more casual physician clothing, even among the areas that did not reach statistical significance (Figure 2).

Bar graph of patient preference of physician attire—all gender, by clinical setting, 2017 versus 2022.
Discussion
Our study findings show that the majority of patients still prefer physicians wearing formal attire in primary care and overall clinical settings. However, this preference decreased significantly in 2022 compared to 2017. In the hospital setting, the preference for formal attire decreased from a previous majority in 2017 to a minority of patients in 2022 with this preference.
It is notable that the clinical settings where decreases in patient preference for formal attire were not significant in 2022, specifically, surgeons and the emergency department, are also the same clinical settings for which baseline preference for formal attire was notably lower in 2017. It is acknowledged that with fewer patients preferring formal attire initially, further decreases in these clinical settings would not likely have practical significance nor statistical significance. Conversely, the areas with the greatest decline in preference for formal attire in 2022, including the settings of primary care, hospital, and overall clinical settings, were the areas that had initially been highest for preference of formal attire in 2017, thus allowing for greater impact from the COVID-19 pandemic.
In the primary care setting where this survey was administered at our institution, the majority of our surveyed patients were female. However, there was a statistically significant increase in the number of male patients in 2022 compared to 2017. This is attributed to our patient survey cohort initially being limited to primary care patients paneled to female primary care physicians in 2017 whereas in 2022, we added a process for surveying patients in the waiting room lobby, which expanded our pool to include patients paneled to both male and female primary care physicians. Although not the primary aim of this study, a subgroup analysis by gender of the respondent was undertaken due to P value < .05 of baseline characteristics noted.
Across all domains of clinical settings and respondents’ gender, there was a decline in the preference for formal attire. However, there were notable differences in our secondary subgroup analysis for different clinical settings when sorted by gender. It is unclear why the male respondents’ preference for formal attire declined more in primary care, emergency room, and overall clinical settings, whereas female respondents declined mainly in the hospital clinical setting.
It is additionally important to recognize that cultural norms for professional business attire are changing across the globe in nonmedical and medical settings. Over the last 30 years, there has been a shift toward a more casual and comfortable dress code in the corporate world. This has been accelerated by the COVID-19 pandemic. 13 For example, JP Morgan Chase has allowed certain employees to wear T shirts and sneakers. In the United Kingdom, the British respondents noted they are less likely to have an office dress code post-pandemic and only 43% believe that formal business attire is required in the office setting. 14 This global trend towards more casual attire may be reflected in patient preferences of physician attire with additional future study needed to evaluate the persistence of this change.
Strengths of our study include using a direct comparison of identical survey materials in the same clinical setting from both before the COVID-19 pandemic in 2017 and again after the COVID-19 pandemic had been underway for 2 years in 2022. Additionally, our sample size was sufficient to meet statistical significance.
Limitations
Limitations of our study include being a single-site outpatient primary care internal medicine clinic and at an academic institution with a historically formal attire dress code. The physician images used were the same images from a 2017 study, published in 2018, at which time it was acknowledged these images were intended to limit confounding variables of bias, however there was a lack of racial, age, and body-type diversity. 2 Additionally, in our study, our patient respondent demographic identified as disproportionately white and female compared to national demographic data. 15 While our findings do meet statistical significance, our sample size and data was limited.
Interestingly, prior to COVID-19, physician demographics influenced the patient's preference for physician attire, with business casual, professional attire, as well as the use of name tags rated positively by patients. However, there was an inconsistent rating of attire preference in subset analysis by physician gender and race, as well as the age of the survey participant. Physician attire was particularly more nuanced for female physicians. 16
Further studies are needed to include respondents from other clinical settings, with broader racial, gender, ethnic, and body mass index (BMI) representation of both patient respondents and physician images to better understand how perceptions may be evolving after the COVID-19 global pandemic. These updated study findings will inform best practices of physician attire to improve patient satisfaction and experience. This information will be applicable to individual practicing physicians as well as healthcare leaders and administrators as they seek to set dress code guidelines and uniform policy.
Conclusion
Patient preference for formal attire among physicians has declined since the COVID-19 pandemic began. This information will help physicians in various clinical settings and healthcare leaders setting attire guidelines for patient satisfaction. Further areas of study include larger numbers, at multiple clinical sites, more clinical settings, and broader racial, ethnicity, BMI, and gender diversity of both survey respondents and physician images.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231203115 - Supplemental material for Patient Perception of Physician Attire Before and After the COVID-19 Global Pandemic Began
Supplemental material, sj-docx-1-jpx-10.1177_23743735231203115 for Patient Perception of Physician Attire Before and After the COVID-19 Global Pandemic Began by Mary S. Hedges, Leila M. Tolaymat, Nicole K. Haskell, Cara Prier, Ashley L. Walker, Claire Haga, Zhuo Li, Mingyuan Yin, Mindy McManus and Nancy Dawson in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735231203115 - Supplemental material for Patient Perception of Physician Attire Before and After the COVID-19 Global Pandemic Began
Supplemental material, sj-docx-2-jpx-10.1177_23743735231203115 for Patient Perception of Physician Attire Before and After the COVID-19 Global Pandemic Began by Mary S. Hedges, Leila M. Tolaymat, Nicole K. Haskell, Cara Prier, Ashley L. Walker, Claire Haga, Zhuo Li, Mingyuan Yin, Mindy McManus and Nancy Dawson in Journal of Patient Experience
Footnotes
Submission Declaration and Verification
We confirm that this work is original and has not been published elsewhere, nor is it currently under consideration for publication elsewhere.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Mayo Clinic Institutional Review Board (IRB) approval for this study was obtained (ID: 21-010389).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Mayo Clinic Institutional Review Board's approved protocols (ID: 21-010389).
Statement of Informed Consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.