
Abstract
This study examined the experience of contraceptive counseling and care in a Federally Qualified Health Center in Maryland. Patients attending medical visits in 2021 were surveyed using the Interpersonal Quality of Family Planning scale to assess the quality of contraceptive counseling. Medical chart reviews were performed to identify alignment between contraceptive care received, and preferences patients had expressed. Primary care providers, reproductive health providers, and a subgroup of patients were interviewed to further contextualize survey and chart review findings. The average item score for the 94 survey participants was 4.39 (SD: 0.9) out of 5. Factor analysis showed high internal consistency reliability (alpha = 0.96). Eighty percent of patients received contraceptive care that aligned with their preferences, 4% did not, and 16% lacked clear contraceptive preferences. Qualitative analysis revealed that patients desired more guidance from providers in selecting a contraceptive method, while providers noted logistical and insurance-related barriers to care. While the quality of contraceptive counseling was high, patient experience of care may be improved by implementing team-based care.
Keywords
Introduction
Person-centered contraceptive counseling and care are central to the protection of human rights in reproductive healthcare. Understanding patient perceptions of contraceptive counseling and related services is critical for supporting patients to achieve their reproductive goals.1,2 Information regarding patients’ preferences around contraceptive use is not routinely collected within health systems, thereby limiting the ability of health services to align care with preferences. 3 Recently, efforts to improve the measurement of the patient experience of contraceptive counseling have resulted in the generation of innovative, self-reported tools,4,5 including the Interpersonal Quality of Family Planning (IQFP) scale 6 (Table 2). The IQFP captures 3 domains of quality in contraceptive care: (1) receipt of adequate information, or comprehensiveness in terms of method options and known side effect profiles, (2) interpersonal connection, or interactions with providers that are congenial or friend-like, ideally contextualized in a relationship built over time, and (3) decision support, or provider involvement in the deliberation process in selecting a contraceptive method.7,8
IQFP Item and Scale Results and Performance from a FQHC in Maryland.

Abbreviations: IQFP, Interpersonal Quality of Family Planning; FQHC, Federally Qualified Health Center.
*Items were evaluated on a scale of 1 (poor) to 5 (excellent).
**SD = the average of how far each item score varied from the mean.
Federally qualified health centers (FQHCs) are designed to meet the primary healthcare needs of socially disadvantaged populations.8,9 In these and other clinic settings, patients consistently report a desire to receive reproductive health services in the same setting as their other essential primary care services.10,11 Within FQHCs and in other primary care settings, provider perspectives regarding the challenges in the delivery of high-quality contraceptive care integrated with other primary care services, have been documented.12–14 In an FQHC in Maryland that serves roughly 40,000 annually, 2 different sets of providers deliver contraceptive services: primary care providers (PCPs; family practitioners) and reproductive health care providers who serve as specialists within the organization. This study sought to characterize the quality of contraceptive counseling according to the IQFP and further describe whether the contraceptive care planned at counseling encounters was eventually received, through the objective lens of the medical record. Further, the study sought to contextualize the context of both counseling and care delivery through structured interviews with patients and providers.
Methods
Study Design
A sequential, explanatory mixed-methods design was used to examine patient perceptions of contraceptive counseling quality and provider experiences with contraceptive service provision among individuals receiving or providing contraceptive services at any of the FQHC's clinic sites in the Baltimore, Maryland area between September–December 2021.
Patient Survey
Characteristics of IQFP Survey Participants.

*Patients self-identified racial and ethnic identities at the time of initial registration for clinical services.
The primary outcome was the quality of contraceptive counseling, measured via the 11-item IQFP scale. Respondents used a 5-point Likert score (1 to 5, with 5 being most favorable) to indicate their level of agreement with each of the 11 IQFP scale items (Table 2). Descriptive statistics were used to assess the distribution and overall level of items and constructs from the IQFP among the study sample. Item-specific means and standard deviations were calculated for each IQFP item and for the overall IQFP scale score. Complete case analysis was used, given our small sample size and concerns related to potential bias arising from the use of multiple imputation to generate data on our key outcome measure.
As this was the first implementation of the IQFP in Maryland, exploratory factor analysis (EFA) was conducted to understand IQFP items and scale functioning in this context. Factor loadings were assessed, with an a priori cutoff of 0.4 for acceptable item loading, and item-total correlations, or the correlation of each item with the total scale score, were examined to confirm positive associations. Internal consistency reliability of the IQFP was assessed using a Cronbach's alpha (α) statistic with a preset acceptable minimum of α>0.6, and item-specific changes in overall alpha scores were assessed based on independent removal of each item. One factor was retained after applying EFA and the solution of final results was therefore unrotated only. This approach to factor analysis has been similarly used with validation of the IQFP in new study contexts. 15 Construct validity was assessed using hypothesis testing to examine variation in IQFP scores according to respondent characteristics. Specifically, we hypothesized that IQFP scores would be higher among insured individuals, those of white, non-Hispanic racial/ethnic background, and older age groups. Unadjusted and adjusted linear regressions were used to test these hypotheses and explore associations between patient's IQFP scores and sociodemographic variables that have been documented to be associated with contraceptive care quality and/or access, including age, race, and insurance status.1,8
Chart Review
Following the survey period, medical chart reviews were conducted by an experienced clinician, to collect patient sociodemographic information (eg, age, insurance status, race, and ethnicity), the preferred contraceptive method identified in patients’ recent visit, and any subsequent contraceptive care delivery within 60 days of that visit. Contraceptive care delivery was determined from patient's medication lists, clinical encounters, and procedure notes within the 60-day period. Among individuals with expressed contraceptive preferences, contraceptive care alignment was assessed as a binary outcome (yes/no). Those without expressed contraceptive preferences were categorized as having contraceptive needs that could not be determined—unable to determine.
Patient and Provider Interviews
A subset of patient survey participants who consented to follow-up interviews was contacted via phone for participation in a structured interview in English or Spanish. Interviews were conducted by a trained qualitative interviewer using an interview tool made up of open-ended questions with prompts such as, “tell me more about that,” to elicit patients’ reflections on contraceptive counseling and care they had received at the clinic. Interviews lasted an average of twelve minutes and were audio-recorded, translated into English (as necessary), and transcribed for analysis. A combination of inductive and deductive thematic extraction was employed to distill results, with 2 researchers independently coding the transcribed interviews and convening to determine the final set of themes, which included the 3 quality domains from the IQFP and an additional theme of contraceptive care delivery that arose via induction.
All providers employed at the time of the study were invited to participate in similarly structured interviews through email-based recruitment messages and announcements during clinical meetings. Scheduled interviews were conducted via the outgoing audio call feature of the Microsoft Teams application with calls placed to the participant's preferred contact number. Structured interview tools elicited provider perspectives on challenges to the provision of contraceptive care within primary care visits. For patients and providers who completed an interview, a $25 electronic gift card was provided, as thanks for participation. Both patient and provider interviews were conducted from November 2021 to January 2022.
Results
Survey Results
Among 257 patients who received contraceptive counseling at a recent medical visit according to their response to the recruitment text message, 103 patients completed the survey, with 94 respondents answering all 11 IQFP questions and comprising the final analytic sample. On average, participants were 32.7 years old (SD: 7.6; range: 17-49 years). Nearly half of the participants (43.6%) were uninsured, with the remaining Medicaid-insured (40.4%), private-insured (13.9%), and Medicare-insured (2.1%). Participants were primarily Black (40.4%) or White (31.9%). Roughly half of the participants were identified as Hispanic.
On average, each IQFP item score was 4.39 out of 5 (SD: 0.9), indicating overall positive contraceptive counseling experiences (Table 2). The item with the lowest average score (mean = 4.10) focused on information provision about the risks and benefits of contraception, while the item with the highest average score (mean = 4.64) reflected respectful provider practices.
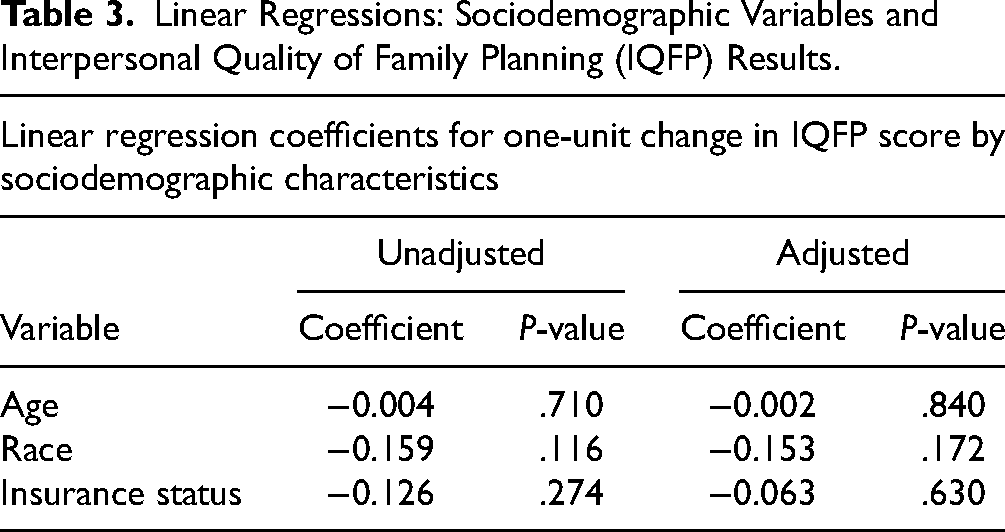
Factor analysis identified 1 factor with an eigenvalue greater than 1 (Factor 1, eigenvalue 7.72) with all items loading >0.4 to Factor 1, confirming the scale's unidimensionality. 16 The total variance explained for the first dimension was 87%. In contrast, the second dimension (eigenvalue = 0.941) only explained 11% of the total variance and did not meet established criteria for being retained as a separate factor. Item-total correlations for were positive for all items (range: 0.72-0.89), indicating consistently positive associations across items with the full IQFP scale. Cronbach's alpha for the IQFP was 0.96, with little variation with the removal of any items from the set (range: 0.95-0.96), suggesting high internal consistency reliability. 17 Results of the hypothesis testing for construct validity found no significant differences in IQFP scores by participants’ age, race, or insurance status (Table 3, indicating that hypotheses related to potential biases in quality counseling were not confirmed.
Linear Regressions: Sociodemographic Variables and Interpersonal Quality of Family Planning (IQFP) Results.
Among survey participants, 16% had contraceptive needs that could not be determined based on documentation in the medical record. Most participants (80%) received desired contraceptive care, with only 4 (4%) who had not received desired contraceptive care. There were 54 (57%) contraceptive users and 40 (43%) nonusers (Table 4. Five patients expressed a desire to avoid pregnancy in the immediate near-term but were not interested in a contraceptive method.
Contraceptive User Characteristics by Contraceptive use status among Participants from a Federally Qualified Health Center (FQHC) in Maryland, U.S. (2021) (N = 94).

Patient and Provider Interviews
Eleven patients participated in structured interviews. Qualitative participant characteristics varied in terms of insurance status, race, and ethnicity, with 5 uninsured, 5 Medicaid-insured, and 1 private-insured patient. Five identified as Black, 5 White, and 1 unspecified race. Five of the 11 participants identified with Hispanic ethnicity.
Ten out of 42 providers participated in interviews, including 7 PCPs and 3 reproductive health providers. Results from patient and provider interviews are presented together in relation to IQFP domains, as well as contraceptive care delivered after counseling.
IQFP Domain—Interpersonal Connection
Overall, patients expressed positive perceptions of their experiences attending FQHCs for contraceptive care and described pleasant interactions with the clinic staff. I love [the clinic]. Everyone there is so respectful. It's so sad to even have to say that people are respectful, but the fact is a lot of times, [healthcare providers] are not respectful, which is why I’ve had to change doctors so many times. Anytime I feel that, as a Black woman, I’m not being treated properly or people are going on stereotypes of other Black people they’ve worked with, you know, I try to just not work with that person anymore. But at [the clinic], everybody is respectful, nice, and not fake. (Patient seen by PCP)
IQFP Domain—Adequate Information
Several patients reported side effects as a critical to their decision-making about contraception and appreciated when providers took the time to describe side effect profiles and carefully considered patients’ prior experiences with side effect. I’ve had not great experiences in the past where [providers are] like, ‘No, you should just use this one,’ even though I said I didn’t like how that made my body react … she [the provider] was super cool about that, did not even bring up the pill, and only targeted the conversation to what I was asking for. (Patient seen by reproductive health provider)
Providers expressed a sense of being limited to provide as much information in counseling sessions as they would consider ideal due to time constraints and multiple priorities. Just because of time, I don’t go into a lot of detail with patients. (PCP)
The main thing is [decision-making about contraception] deserves a full conversation … We are just rushed, rushed, rushed, and patients have unrealistic expectations of how much can be addressed in one visit. (PCP)
IQFP Domain—Decision Support
A few patients expressed appreciation for an approach to counseling that relied on answering patient questions only when posed. So, every question I had she was amazing at answering, and it made me feel like she was not pushing me toward a specific thing, which I thought was great. (Patient seen by reproductive health provider)
A more common sentiment, however, was the desire for direction from providers to help patients choose a contraceptive that met their needs and preferences. I don’t think anything has necessarily been offered beyond what I explicitly asked, which isn’t necessarily bad, but some people don’t know what to ask. (Patient unsure if seen by PCP or reproductive health provider)
When I ask them, “can I change birth control?,” they just say, “OK, what do you want to change to?” It's not like, “OK, well, I would suggest this”, or “What would you look for in birth control?” (Patient seen by reproductive health department)
I’m uneducated and ignorant to the medicine portion of [contraceptive options], and they have the knowledge, and they are asking me my input and I don’t know. Essentially, just be more informative, more sensitive to the fact that you are the expert, and I am not. (Patient seen by reproductive health department)
In contrast to many patients’ preference for more directive counseling, providers expressed some hesitancy. As 1 provider described: I will say, even if it's clear in the scope of the discussion that they don’t want pregnancy and they’re having behavior that is going to lead to pregnancy, if they clearly shut it down, I don’t push it because I don’t want to ruin my rapport with them. (Reproductive health provider)
Contraceptive Service Delivery
Providers expressed a desire to be able to meet patients’ individualized needs for contraceptive care, describing frustration related to time constraints on care. Providers also emphasized challenges they faced with scheduling and logistics as hindering their ability to provide the highest quality contraceptive care. For example, PCPs shared their reliance on the reproductive health department for ensuring patients’ contraceptive care needs were met, due to conflicting priorities within routine visits and full schedules. This was also apparent to reproductive health staff. I know there are issues sometimes with the other [non-reproductive health] departments having sessions or blocked procedure visits. That's probably the biggest issue [for delivering high-quality care] is them having the time. I know sometimes they will refer to our department because it's such a long wait for them to see their own patients, even when I think they probably would like to [care for] their patients themselves. (Reproductive health provider)
PCPs outside the reproductive health department also reported insufficient schedule space and therefore insufficient patient volume to remain comfortable with the insertion and removal procedures. I don’t really do Nexplanon's at [this site] because there are plenty of other people that want to do it, and it takes too much time … I’m booked out until [four months from now], so I want to maximize the number of patients who can come in and see me. I don’t really want to take 40 min to do that right now. That's not really on my radar of most important things.’ (PCP)
I’m new to practice, I would definitely need to increase my volume very soon in order to remain competent. (PCP)
I wish we had a little more practice where we had somebody mentor us to see how we are inserting and removing, to give us more confidence. (PCP)
Providers also discussed the need for device ordering and stocking procedures to be consistent and clear for support staff to efficiently set up for procedures, without a detrimental impact on their clinic flow. Providers emphasized the importance of having designated procedure slots in their schedules to accommodate LARC procedure visits without significant delay. We do have slots which enable us to kind of have blocked time to do procedures, so that is really helpful in getting people in quickly for those [LARC] procedures. (Reproductive health provider)
Providers noted that there is a discrepancy in care for insured versus uninsured patients in terms of financial access of LARCs. In terms of the patients who are uninsured and want an option that is unaffordable for them, we do have a system in place whereby we can send them through to access some of our funding for patients who need financial care, but it's not real well-honed … It's definitely an area for improvement, I would say. (Reproductive health provider)
We’re an access point for so many patients who don’t have easy access to healthcare … I think there are good questions to continue to ask in terms of access within our own organization, especially financially. (Reproductive health provider)
Patients also recognized schedule- and insurance-related barriers to accessing care. For example: I don’t know if [the clinic] is understaffed, like if I call to make an appointment today, I probably won’t be seen for two to three months … If I didn’t have horrible health insurance, I probably would go elsewhere. (Patient seen by PCP)
Discussion
Ensuring high-quality contraceptive care is a vital function of any primary care system, especially those that serve historically disenfranchised patient groups. Our mixed-method study of an FQHC in Maryland applied the IQFP, a validated instrument for measuring quality of contraceptive counseling. Results indicate positive patient experiences with providers in their counseling encounters. These results did not vary by patients’ sociodemographic factors, contrary to findings from previous studies,1,8 suggesting that the FQHC care environment may achieve more equitable counseling experiences than in other settings. However, provider interview results caution that inequitable financial accessibility of effective contraceptive methods (eg, prescription-based or long-acting reversible contraceptive methods) persists based on insurance status, with uninsured patients experiencing higher contraceptive costs than insured counterparts.
The methods used in this study demonstrate that while a validated quality measurement tool can successfully be applied as the basis of quality improvement measures for the contraceptive counseling experience, additional tools are required for characterizing broader interactions with the care environment and discovering opportunities for improvement. For example, patients reported a desire for more direction from providers when selecting a contraceptive method during their interviews, while providers highlighted schedule-related challenges to addressing contraceptive care along with all other primary care services. PCPs were also reportedly less available than reproductive health care providers to meet contraceptive care needs. This highlights the potential for the organization to enhance internal referral systems and to ideally create a team-based care structure that would optimize timely appointments for contraceptive care needs within the reproductive health department.
Limitations
The FQHC serves a diverse population in terms of gender and sexual identity, but study participants were limited to cisfemale (for interviews) and either transmale or cisfemale for survey respondents. Furthermore, the patient survey did not include a measure to assess the IQFP scale's validation, such as general patient satisfaction, against which to compare participant responses to the IQFP items. Self-selection bias by those who had a positive contraceptive counseling experience, or positive response bias regarding perceptions of interactions with providers may also have contributed to results that do not vary significantly by sociodemographic characteristics.
Research Agenda Recommendations
Ongoing implementation research at the service delivery level is recommended to identify effective ways of delivering high-quality, person-centered reproductive health care in the FQHC clinic setting. Developing a team-based care system where continuity may be pursued with a team made up of a PCP and a reproductive health department “partner” presents an innovative solution to providing high-quality contraceptive care alongside primary care services in the FQHC setting. 18
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Johns Hopkins Bloomberg School of Public Health.
Ethical Approval
The Johns Hopkins Bloomberg School of Public Health IRB reviewed and approved the study in September 2021. Survey participants consented to participation in a text message-based survey by proceeding to voluntarily enter responses after reviewing and agreeing to written informed consent. Interview participants provided verbal, recorded consent. No signatures were collected, in the interest of anonymity.